
Abstract
Introduction
Patients commonly present to the ear, nose, and throat (ENT) emergency unit and outpatient department with foreign bodies (FBs), with the external auditory canal (EAC) as the most frequent site.1-4 Although some patients with EAC FBs are asymptomatic upon presentation, others complain of otalgia, otorrhea, tinnitus, dizziness, bleeding, or decreased hearing.5-7 Most EAC FBs are removed using forceps or hooks under direct vision, 8 but endoscopic/microscopic removal under general anesthesia (GA) in the operating room (OR) may be required, particularly in uncooperative children. 9 Common complications following removal procedures include EAC laceration, tympanic membrane (TM) perforation, acute otitis externa (AOE), and acute otitis media (AOM).3,6,7,10-12 Ossicular chain destruction, hearing impairment, and facial nerve paralysis have also been reported.6,7,12,13 Ungraspable beads are the most common in children,9,11,12,14-20 while graspable insects and cotton tips are common in adults.6,11,12,15,21 Although several studies had conducted univariate analyses of the complication rates,6,12,21 Cho et al. found that age <7 years, failed attempts, longer impaction time, ungraspable FBs, TM-touching FBs, and biotic FBs significantly increased the complication rate. 12 However, the most frequent type of EAC FB varies depending on the age of the patient, and univariate analyses of the age-dependent complication rates have seldom been performed independently in the literature. Therefore, we identified the clinical features and complications in patients who visited the ENT emergency unit for the removal of an FB in the EAC in a single tertiary medical center, and univariate analyses were performed separately in different age groups to determine the risk factors for developing complications.
Materials and Methods
This retrospective study was approved by the Institutional Review Board of Chang Gung Medical Foundation (IRB No. 202400884B0). The medical charts of patients who visited the ENT emergency unit of Chang Gung Memorial Hospital, Linkou, Taiwan, between August 2016 and May 2023 with the complaint of EAC FB were reviewed. Removal procedures were initially performed by otolaryngologists in the ENT emergency unit using forceps or hooks under direct vision aided by headlamps. If direct removal in the ENT emergency unit failed or the patient was uncooperative, he or she was transferred to the OR for endoscopic/microscopic removal of the FB under GA. Patients with an FB in the EAC were included in the study. Patients in whom only cerumen was found or nothing from the EAC was recovered were excluded. The sex and age of the patients as well as the type, laterality (bilateral or unilateral), nature (biotic or abiotic), and graspability (graspable or not graspable) of the FB, the requirement for operative removal (yes or no), and the development of complications following the removal procedure were recorded. Complications were defined as TM perforation, AOM, myringitis, AOE, or EAC laceration/erosion/bleeding/hematoma. All patients were also classified into two groups according to age: <10 years and ≥10 years. Univariate analyses of the complication rates for all patients as well as patients in the age <10 years group and the age ≥10 years group were performed using a chi-squared test, or if the excepted frequencies were low, Fisher’s exact test. 22 A P-value <.05 was considered to indicate statistical significance. Means with standard deviations and odds ratios with 95% confident intervals were calculated. All statistical analyses were performed using MedCalc Statistical Software version 23.0.2 (MedCalc Software Ltd, Ostend, Belgium).
Results
A review of the medical charts of 493 potentially-eligible patients showed that in 36, either only cerumen was found (n = 4) or there was no FB (n = 32) in the EAC. After excluding these patients, 457 patients presenting with EAC FBs were included. Of these, 261 were male and 196 were female. The mean age of the patients was 29.9 ± 19.9 (range, 1.0-89.0) years, with 195 patients aged between 0 and 9 years (Figure 1). The right ear was affected in 250 patients, the left ear in 195, and both ears in 12 (Figure 2).
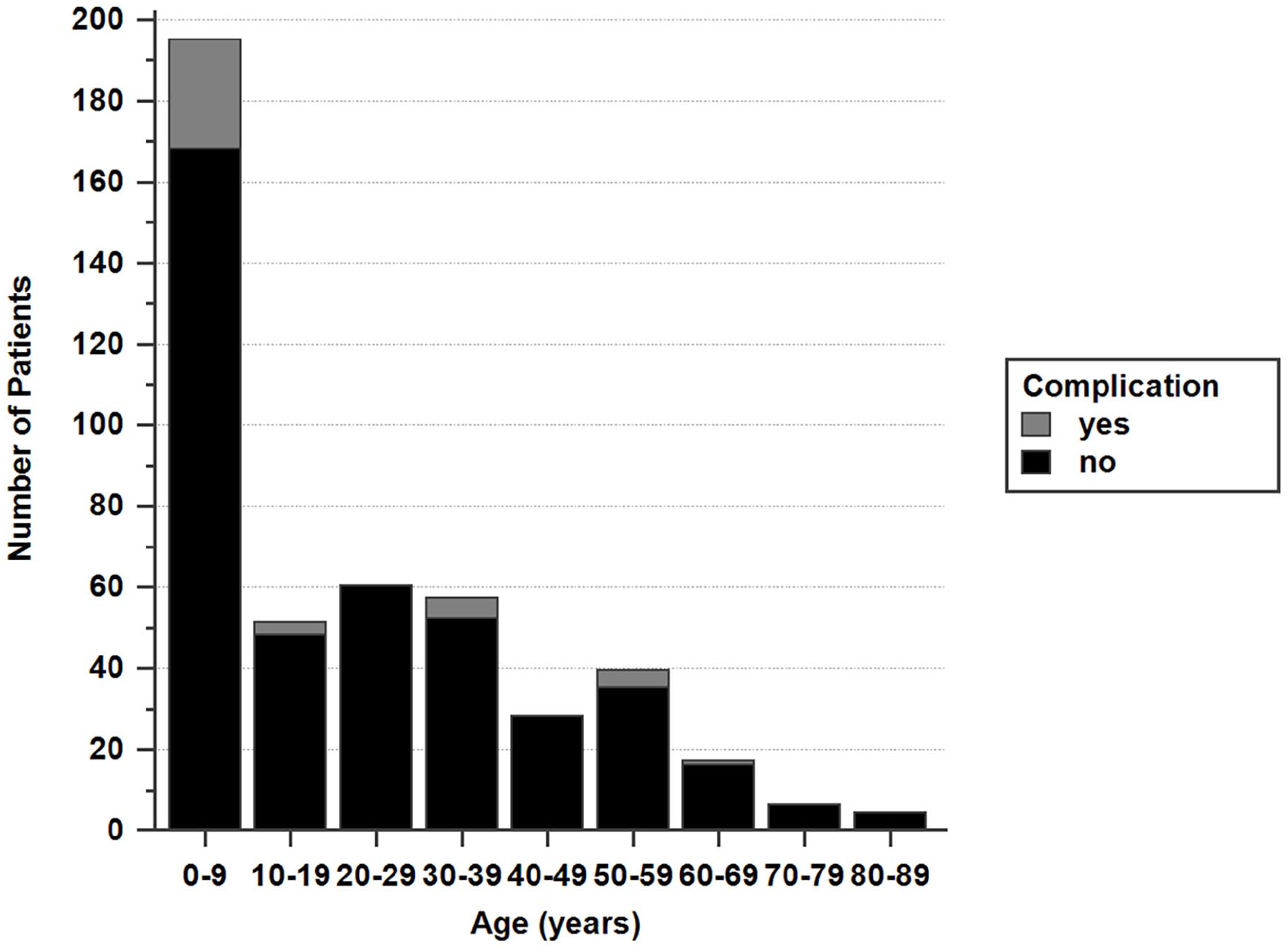
The age distribution of patients with EAC foreign bodies.
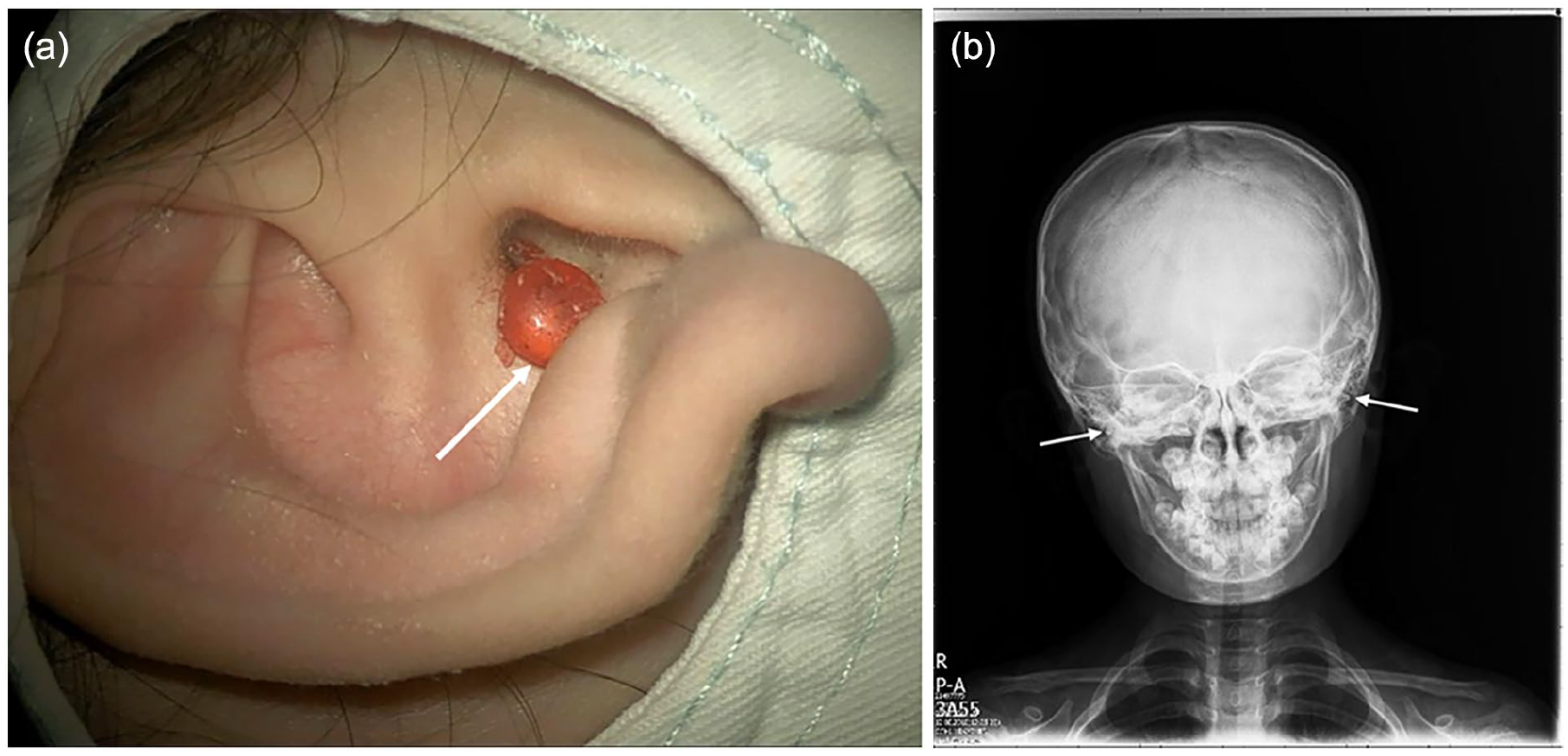
(a) A 9-year-old girl who inserted a bead (white arrow) into her right EAC underwent microscopic removal under general anesthesia because of failed removal of the bead using a hook. (b) A 5-year-old girl inserted beads into both EACs. Skull radiography shows two small radiopaque foreign bodies (white arrows) bilaterally in the EAC.
Biotic and abiotic FBs were found in 209 and 248 patients, respectively. Graspable and not graspable FBs were found in 295 and 162 patients, respectively. The most common types of FB for all patients were insects (n = 184), beads (n = 84), and cotton tips (n = 41). Table 1 summarizes the types of FB found in the two age groups. In the age < 10 years group (n = 195), the most frequent types of FB were beads (n = 74), seeds (n = 23), and paper/plastic (n = 18). In the age ≥10 years group (n = 262), the most frequent types were insects (n = 178) and cotton tips (n = 33). The FBs were removed in the ENT emergency unit under direct vision aided by headlamps in 411 patients, and in the OR by endoscopic (n = 9)/microscopic (n = 37) removal under GA in 46 patients in whom either direct removal failed or the patient was uncooperative.
Types of foreign bodies according to age groups.
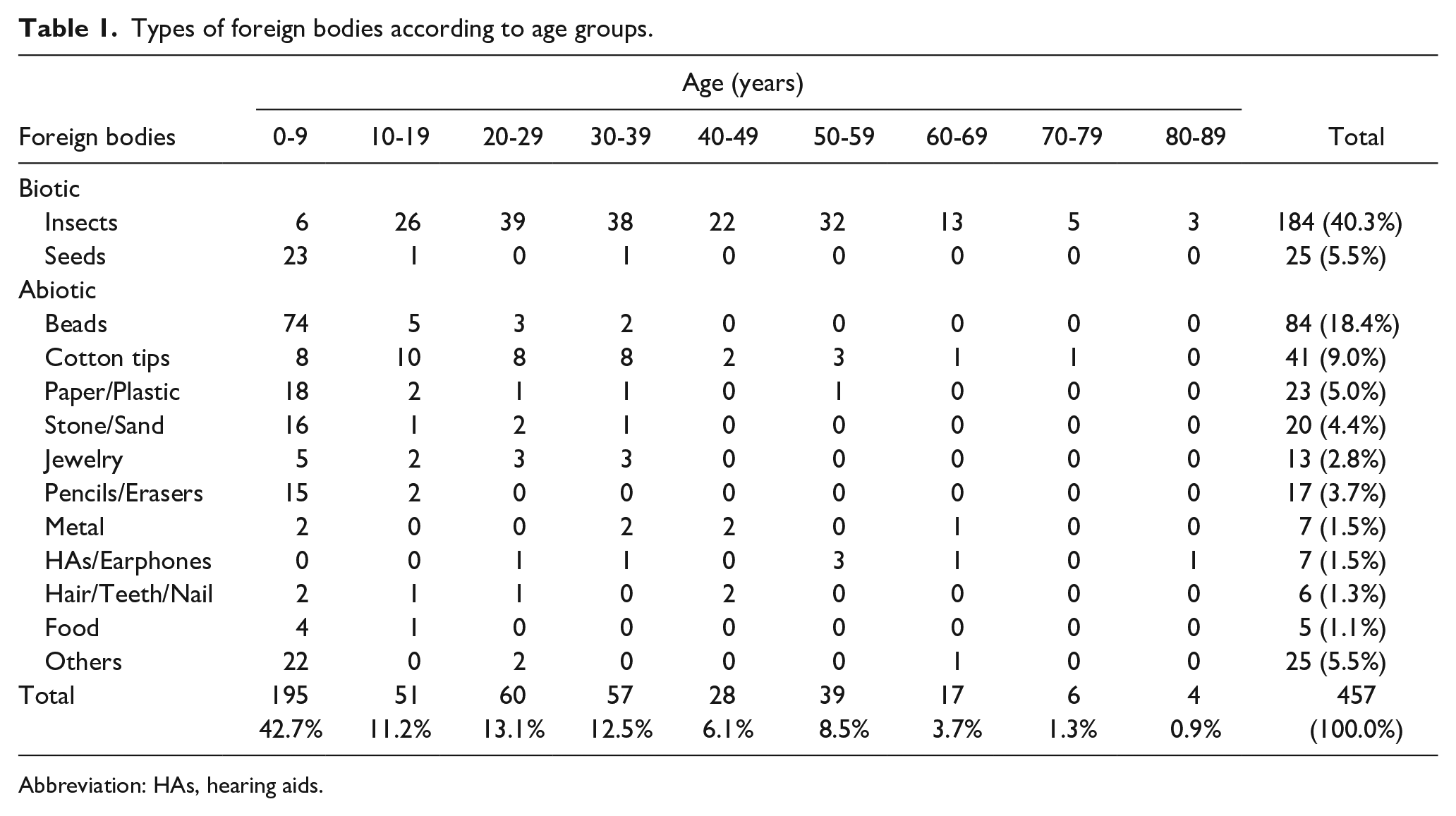
Abbreviation: HAs, hearing aids.
The overall complication rate following removal procedures was 8.8% (40/457). In the age <10 years and age ≥ 10 years groups, the complication rates were 13.8% (27/195) and 5.0% (13/262), respectively, and the difference was statistically significant (P = .001). The most common complication was EAC laceration (n = 20) followed by TM perforation (n = 7), EAC erosion (n = 5), EAC bleeding (n = 3), myringitis (n = 2), AOE (n = 2), AOM (n = 1), and EAC hematoma (n = 1). Significant higher rate was determined for EAC laceration (6.7% vs 2.7%, P = .039) in the age <10 years group than in the age ≥10 years group. Table 2 summarizes the complications in the two age groups. One patient developed both TM perforation and AOM.
Complications following removal procedures according to age groups.
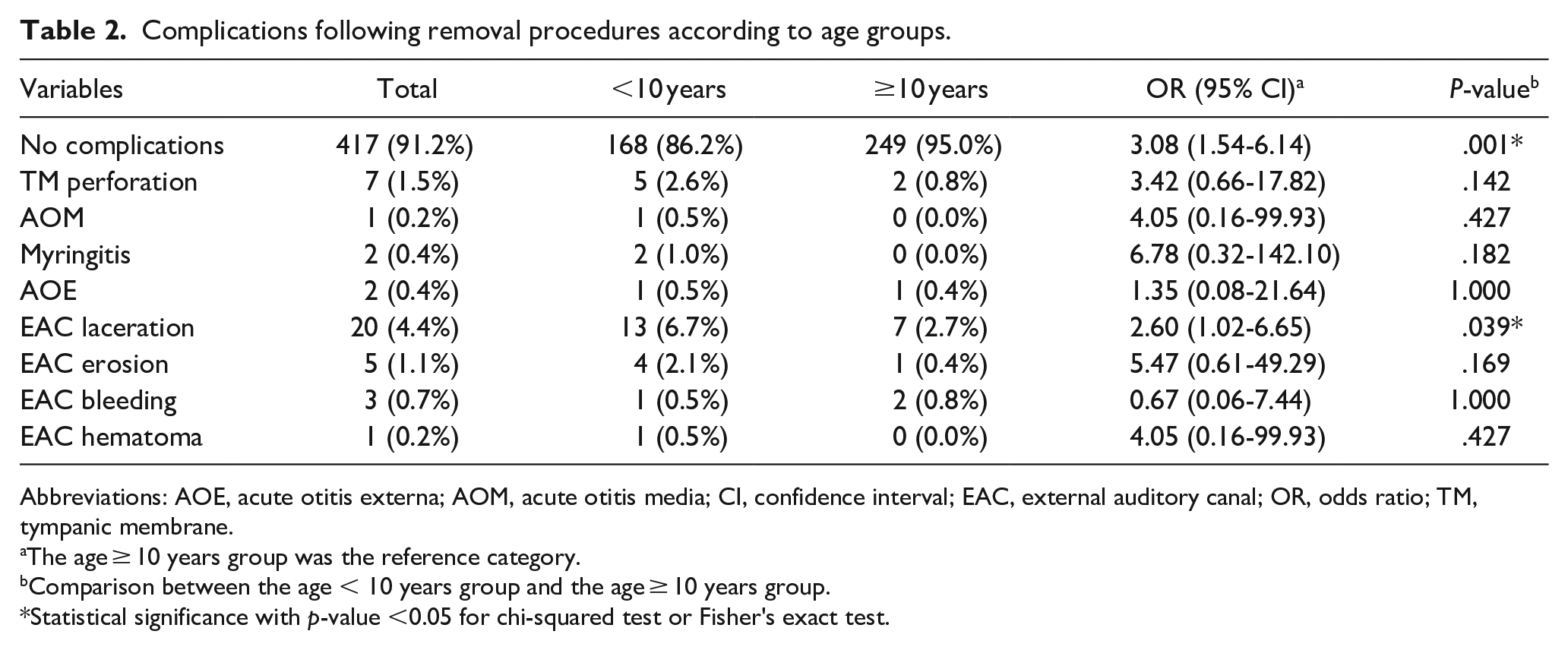
Abbreviations: AOE, acute otitis externa; AOM, acute otitis media; CI, confidence interval; EAC, external auditory canal; OR, odds ratio; TM, tympanic membrane.
The age ≥ 10 years group was the reference category.
Comparison between the age < 10 years group and the age ≥ 10 years group.
Statistical significance with p-value <0.05 for chi-squared test or Fisher's exact test.
In univariate analyses of all patients (Table 3), there were statistically-significant differences in the complication rates with respect to patient age, the nature of the FB, the graspability of the FB, and the requirement for surgical removal. No significant differences in the complication rates were determined with respect to the sex of the patient or the laterality of the FB.
Complication rates of overall participants according to features of patients and foreign bodies.
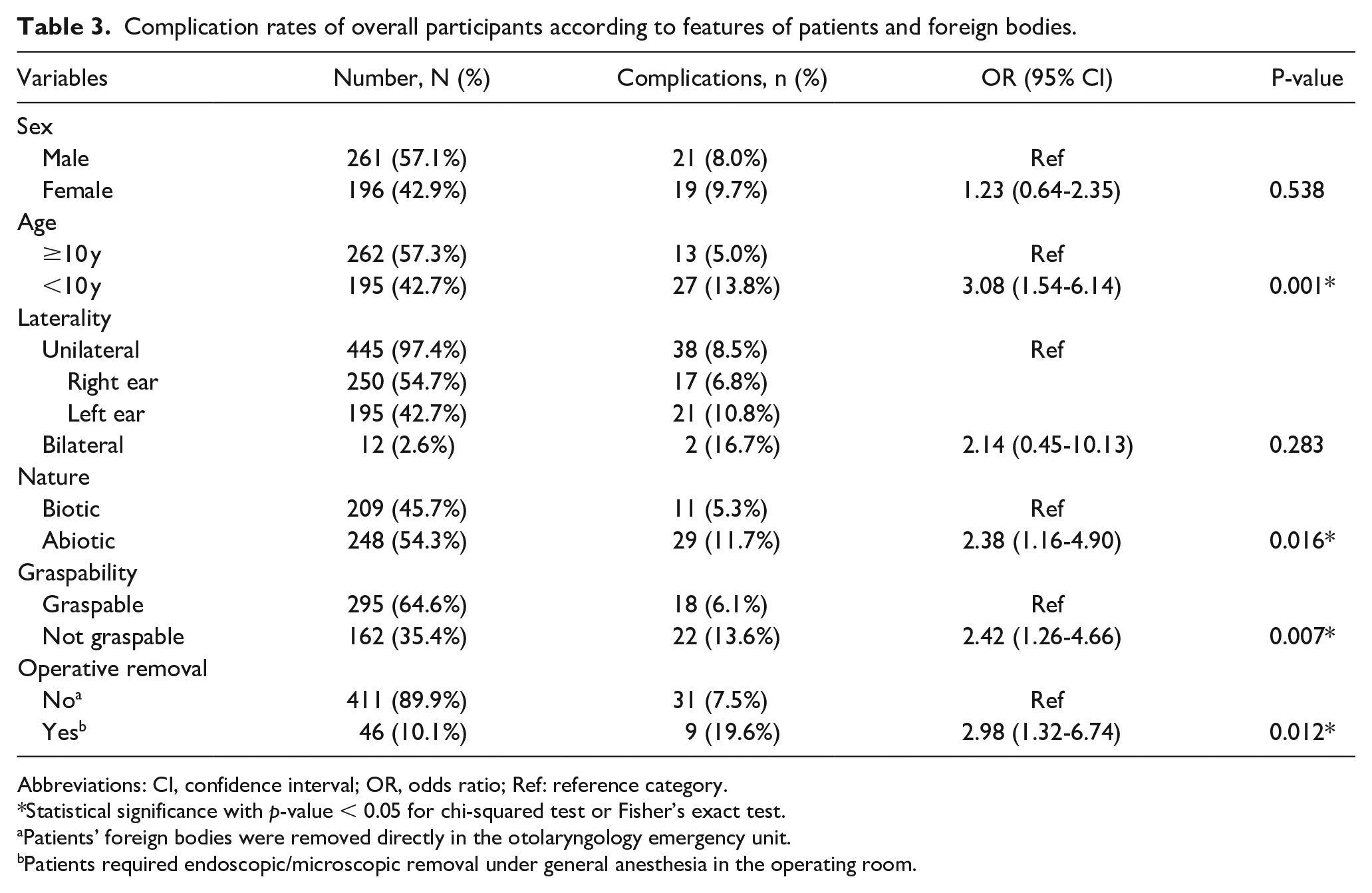
Abbreviations: CI, confidence interval; OR, odds ratio; Ref: reference category.
Statistical significance with p-value < 0.05 for chi-squared test or Fisher’s exact test.
Patients’ foreign bodies were removed directly in the otolaryngology emergency unit.
Patients required endoscopic/microscopic removal under general anesthesia in the operating room.
Among patients in the age <10 years (n = 195, Table 4) and age ≥ 10 years (n = 262, Table 5) groups, 63.1% and 52.7%, respectively, were male. The right ear was involved in 60.5% and 50.4% of cases, respectively. In the age < 10 years group, 85.1% of the FBs were abiotic and 69.7% were not graspable. In the older group, 68.7% of the FBs were biotic and 90.1% were graspable. Surgical removal of the FB was necessary in 23.1% of the patients in the age <10 years group but only 0.4% of the patients in the other group. The age <10 years group accounted for 66.9% (166/248) of the abiotic FBs, 84.0% (136/162) of the not-graspable FBs, 97.8% (45/46) of the patients requiring operative removal of the FB, and 67.5% (27/40) of the patients with complications. The older group accounted for 86.1% (180/209) of the biotic FBs, 80.0% (236/295) of the graspable FBs, 63.5% (261/411) of the patients not requiring operative removal of the FB, and 59.7% (249/417) of the patients without complications.
Complication rates of the age <10 years group according to features of patients and foreign bodies.
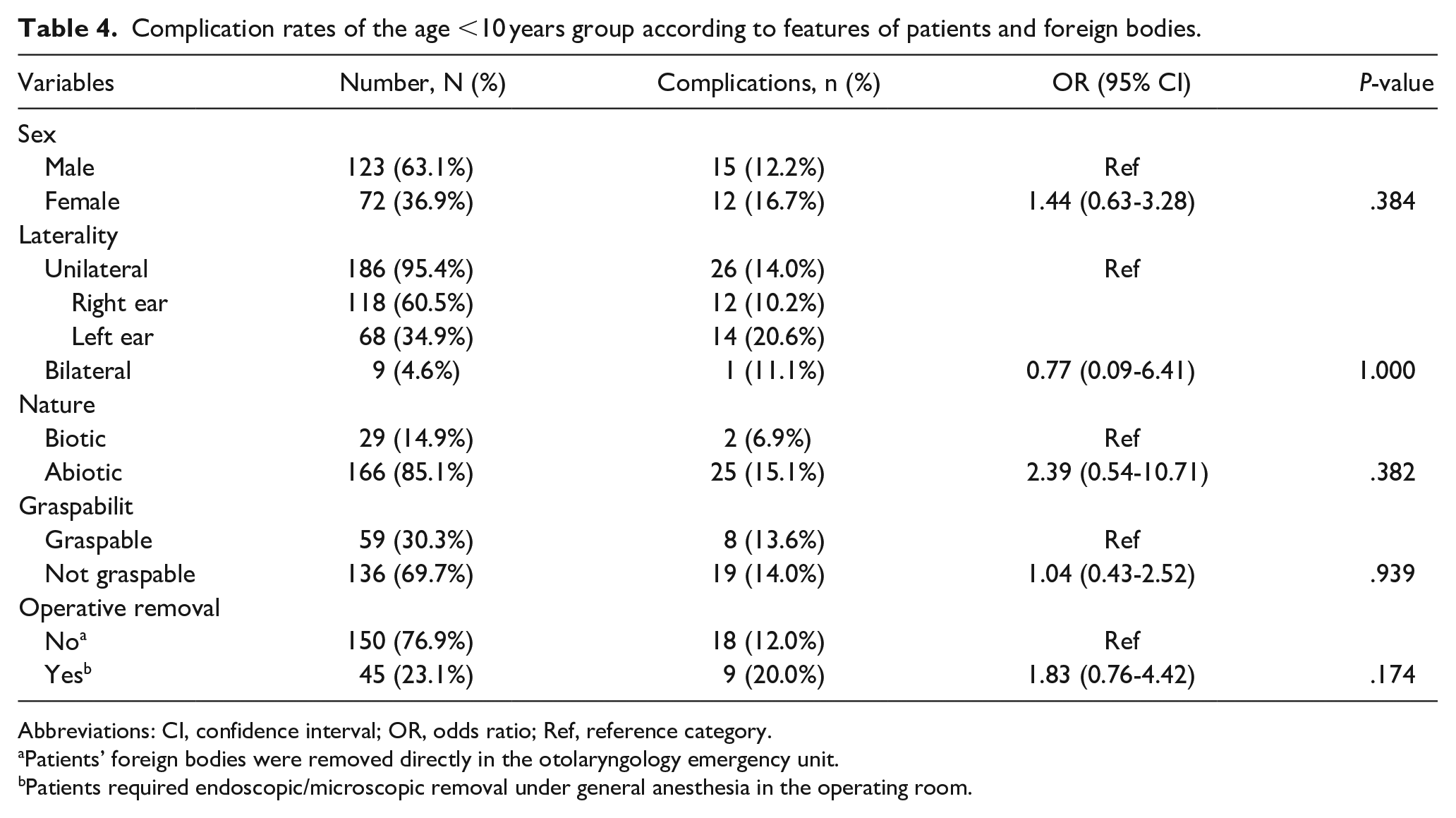
Abbreviations: CI, confidence interval; OR, odds ratio; Ref, reference category.
Patients’ foreign bodies were removed directly in the otolaryngology emergency unit.
Patients required endoscopic/microscopic removal under general anesthesia in the operating room.
Complication rates of the age ≥10 years group according to features of patients and foreign bodies.
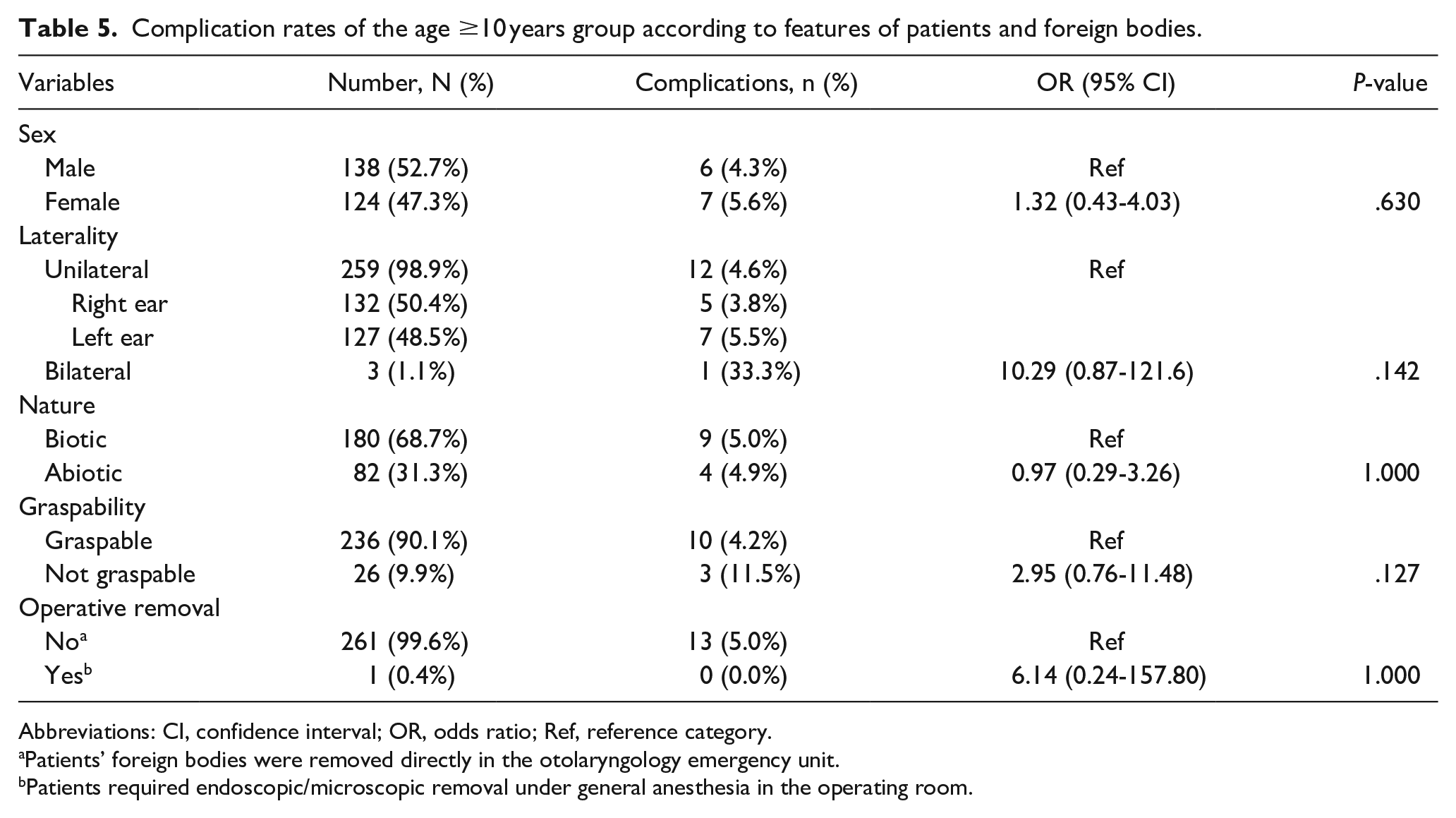
Abbreviations: CI, confidence interval; OR, odds ratio; Ref, reference category.
Patients’ foreign bodies were removed directly in the otolaryngology emergency unit.
Patients required endoscopic/microscopic removal under general anesthesia in the operating room.
Univariate analyses of the two age groups (Tables 4 and 5) both showed no statistical differences in the complication rates with respect to the sex of the patients, the laterality of the FBs, the nature of the FBs, the graspability of the FBs, or the need for operative removal of the FBs.
Discussion
Among patients with EAC FBs, 42.7% were between 0 and 9 years of age. In the series of Cho et al., patients in this age range accounted for 25.5% of those with EAC FBs, while in the series of Al-Juboori et al. and Olajide et al., patients aged 0 to 10 years accounted for 25.5% and 61.0%, respectively, of the patients with EAC FBs.7,10,12 In Morris et al., 85.9% of the EAC FBs occurred in children <15 years of age, which was attributed to the curiosity and carelessness of children in this age group. 23 In patients <10 years of age, males accounted for 63.1%, and the right ear was affected in 60.5%. These findings are compatible with those of other studies of pediatric patients, in which males made up 55.5% to 66.7% of the cohort,8,9,13,17,18,20,24-27 and the right side was affected in 61.0% to 67.2% of cases17,24,26,28,29. The predominance of right-ear involvement can be explained by the fact that most people are right-handed and children tend to insert FBs into their EAC using their dominant hands. 8 In the age ≥ 10 years group, there was only a slight preponderance of male patients (52.7%) and right-ear involvement (50.4%), which can be explained by the fact that insects were the most common type of FB found in this group (67.9%) such that the sex and the handedness of the patient was irrelevant. For the 178 patients, age > 10 years with insects as the FB, 51.1% were male and the right ear was involved in 51.1% of cases. There was also no predominance of male patients or right-ear involvement in the adults included in Nakao et al. or Ryan et al.15,21
The most frequent types of FB in the age < 10 years group in our series were beads (37.9%), seeds (11.8%), and paper/plastic (9.2%), in agreement with previous studies.14,30 Other common FB types that have been found in children include stones and toy pieces.1,8,9,12,16,17,20,28 In the older group, the most frequent types of FB were insects (67.9%) and cotton tips (12.6%), with similar types found in patients 10 to 19 years of age and ≥20 years of age. In earlier studies of adult patients, the most common types of FB were also insects and cotton tips.12,15 The rate of operative removal for patients in our study was 10.1%, in line with the rates of 0.0% to 19.5% reported in other studies.2,4,6,7,11,12,15,21,31,32 In the younger group, the rate (23.1%) was comparable to those in other studies of pediatric patients, which reported rates of 0.0% to 29.8%.1,8,9,13,14,17,18,20,24-27,29,30,33
The complication rate following removal procedures was 8.8% in our study; previous studies reported rates of 4.3% to 31.4%.3-5,7,10-12 Among our patients, the complication rate was higher in the younger group (13.8% vs 5.0%, P = .001). Other studies of pediatric patients reported complication rates of 13.6% to 25.6%.1,9,29,30 Cho et al. reported a significantly-higher rate in patients <7 years of age (45.1% vs 28.0%) than in older patients. 12 Frequently-mentioned complications in previous studies included EAC laceration, TM perforation, and AOE, and the reported rates were 0.9% to 27.7%, 0.5% to 4.9%, and 0.7% to 8.1%, respectively.1,3-5,7,9-12,29,30 The rates of EAC laceration, TM perforation, and AOE for all patients in our study were within this range: 4.4%, 0.4%, and 1.5%, respectively. EAC laceration was the most frequent complication both in our study and in previous studies.1,4,7,9,10,12,29,30 Additionally, a significantly-higher rate of EAC laceration was found in the younger group (6.7% vs 2.7%, P = .039). This may be explained by the younger patients' relative lack of cooperation and the smaller EAC,14,19 which increases the likelihood of injury from forceps or hooks during removal procedures. Other studies in pediatric patients have reported EAC laceration rates ranging from 4.1% to 34.8%.1,8,9,13,18,20,25-27,29,30,33
It is crucial to perform univariate analyses of complication rates for different age groups in our study, as the type of EAC FB varies with patient age. Relying solely on univariate analyses for the entire patient population could lead to misinterpretation of the statistical results. According to univariate analyses of all patients, age <10, abiotic FBs, not-graspable FBs, and the requirement for operative removal increased the complication rate following the removal procedures. By contrast, in univariate analyses of each age group, none of these variables was significantly associated with the complication rate, which implies that, among our study patients, age <10 was the most important risk factor for developing complications. The differences in statistical results among all patients and between the two age groups can be explained by the characteristics of the patients and the types of FB. Patients in the younger group had much higher frequencies of abiotic FBs (85.1% vs 31.3%) and ungraspable FBs (69.7% vs 9.9%); they also had higher rates of operative removal (23.1% vs 0.4%) and complications (13.8% vs 5.0%). They accounted for 66.9% (166/248) of those with abiotic FBs, 84.0% (136/162) of those with not-graspable FBs, 97.8% (45/46) of those requiring operative removal, and 67.5% (27/40) of those with complications.
As noted above, Cho et al. found not only that patients under 7 years of age had a significantly-higher complication rate, but also that ungraspable FBs and biotic FBs were risk factors for developing complications, in contrast to our findings. 12 Nonetheless, both Olajuyin et al. and Mingo et al. reported that the graspability of FBs did not significantly influence the complication rates,13,33 and Kim et al. found no evidence that biotic FBs significantly cause complications. 19 Previous studies have reported that multiple attempts increase the complication rate,12,14,27,31,33 as does removal procedures performed by non-ENT specialists rather than otolaryngologists.7,13,18,28,32 Accordingly, it has been suggested that all patients with EAC FBs should be referred to an otolaryngologist for proper management and better outcomes.18,28,32 Based on a meta-analysis, White et al concluded that patients presenting to an otolaryngologist after previous failed attempts are more likely to require sedation or GA. 34 Because a failed attempt might lead to patient sensitization, subsequent attempts might be difficult due to a lack of cooperation, particularly in young children.14,27 Since multiple attempts also increase the complication rate, sedation or GA should be considered for uncooperative patients and those with EAC FBs that are difficult to remove.9,19
A limitation of this study was its retrospective design; thus, whether the complications were caused by the FBs or the removal procedures could not be determined. Besides, there was limited documentation in the medical charts regarding the numbers of previous removal attempts, who performed those procedures, and the duration of the impaction. Although a longer duration of impaction has been reported to be a risk factor for developing complications,4,12 this conclusion is not supported by several other studies.6,13,27 Another limitation was that some patients were lost to follow-up after FB removal, which might make it difficult to determine the late complication rates.
Conclusion
The peak age range for patients with EAC FBs was 0 to 9 years. In the <10 years age group, beads were the most common type of FB, while in the ≥10 years group, insects were the most common. Most EAC FBs could be removed directly and safely in the ENT emergency unit without major complications. However, 10.1% of patients required operative removal in the OR. Complications occurred in 8.8% of patients, with EAC laceration being the most frequent complication (4.4%). Age <10 years was the most significant risk factor for complications following EAC FB removal, with this group showing a higher risk of EAC laceration. To minimize complications after a failed removal under direct vision, sedation or endoscopic/microscopic removal under GA should be considered for this age group. Further studies are warranted to determine the efficacy and safety of this clinical practice for EAC FBs in younger patients.
Footnotes
Acknowledgements
None.
Data Availability
The relevant data of this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was granted by the Institutional Review Board of Chang Gung Medical Foundation (IRB No. 202400884B0).
Informed Consent
Since this was a retrospective study, written informed consent was not obtained.