
Abstract
Objectives:
Foreign bodies (FBs) in external auditory canal (EAC) can occur at any age but are especially common in children and adolescents. The aims of the study were to evaluate the clinical characteristics of EAC FBs in children and adolescents and to discuss their proper management.
Methods:
A retrospective medical chart review was performed on patients who were treated for EAC FBs in a tertiary referral center from January 2007 to December 2017. We investigated the parameters of age, sex, type of FB, sedation method, complications, and removal strategy.
Results:
Of 284 patients, 176 (62.0%) were male. Peak incidences were noted at the ages of 3 to 6 years and 17 to 18 years. The frequently observed FBs were insects, followed by air-gun pellets, cotton balls, marbles, and earrings. Forty-one (14.4%) EAC FBs were removed with the naked eye, while 243 (85.6%) were removed under microscope in the otolaryngology department. Of these patients, 23 (9.5%) were administered sedatives and 1 (4.1%) needed general anesthesia. During or after the removal procedure, 4 (15.5%) patients had complications of EAC abrasion or laceration (42, 14.8%), and tympanic membrane perforation (2, 0.7%).
Conclusions:
External auditory canal FB showed a distinct characteristic of incidence regarding age, related to removal strategies. Characteristics of FB must be considered for safe removal.
Introduction
Foreign bodies (FBs) in the external auditory canal (EAC) are frequently encountered in pediatric and otolaryngology practice. 1 External auditory canal FBs present with diverse symptoms including unilateral aural discharge, otalgia, ear bleeding, hearing loss, tinnitus, cough, dizziness, and facial palsy, while some EAC FBs are nonsymptomatic and are identified incidentally during routine otoscopic examination. 2,3 The symptoms of EAC FBs are closely related to the characteristics of the foreign materials involved, which can be categorized as organic versus inorganic, animate versus inanimate, metallic versus nonmetallic, hygroscopic versus nonhygroscopic, and so on. 4
Although many FBs can be easily removed, the removal procedure can be a source of substantial morbidity of the external ear and middle ear structures. Physicians can have difficulty removing FBs in the EAC, especially with narrow EACs and limited cooperation on the part of children and adolescents. 5,6 Otolaryngologists can remove EAC FBs using many kinds of instruments, either with the naked eye or under a microscope, and sedatives or general anesthesia are needed in some cases to immobilize children. 5,7 Indeed, struggling during attempted removal can lead to complications such as perforation of the tympanic membrane and abrasion of EAC skin. 8,9
The aim of this study was to evaluate the clinical characteristics of EAC FBs in children and adolescents and to discuss their proper management.
Materials and Methods
A retrospective medical chart review was performed on patients younger than 20 years with EAC FBs, who were managed in the emergency department or otolaryngology/pediatric outpatient department from January 2007 to December 2017. The study population was selected by searching an electronic medical database with the diagnostic code “Foreign body in EAR” (T17, International Classification of Diseases, Tenth Revision) or the procedure codes for EAC FB removal.
Medical data regarding previous medical history, age, sex, initial symptoms, type of FB, management strategy/method, and complications were thoroughly reviewed. This investigation was approved by the local ethics review board and performed in accordance with the Declaration of Helsinki and good clinical practice guidelines
Results
Demographics of the Study Population
A total of 284 patients with EAC FBs were reviewed in the present study. Of these, 176 (62.0%) were male. There were various types of FB: insects (19.7%) were the most frequent, followed by air-gun pellets (17.3%), cotton balls (14.4%), marbles (10.2%), and earrings (4.5%). Forty-one (14.4%) EAC FBs were removed with the naked eye in the emergency department or otolaryngology department, but 243 (85.6%) required a microscope for removal, of which 23 (9.5%) required sedation and 10 (4.1%) needed general anesthesia. Most patients with EAC FBs (84.5%) had no complications, but 44 (15.5%) had complications including EAC abrasions and lacerations (42 cases, 14.8%) and perforation of the tympanic membrane (2 cases, 0.7%). Two hundred and fifty (88.0%) patients initially visited the emergency department; in 39 (13.7%) cases, the FB was successfully removed in the emergency room by a nonotolaryngologist, but 211 (74.3%) patients were referred to otolaryngologists (Table 1).
Demographic and Clinical Characteristics of Patients With EAC Foreign Bodies.
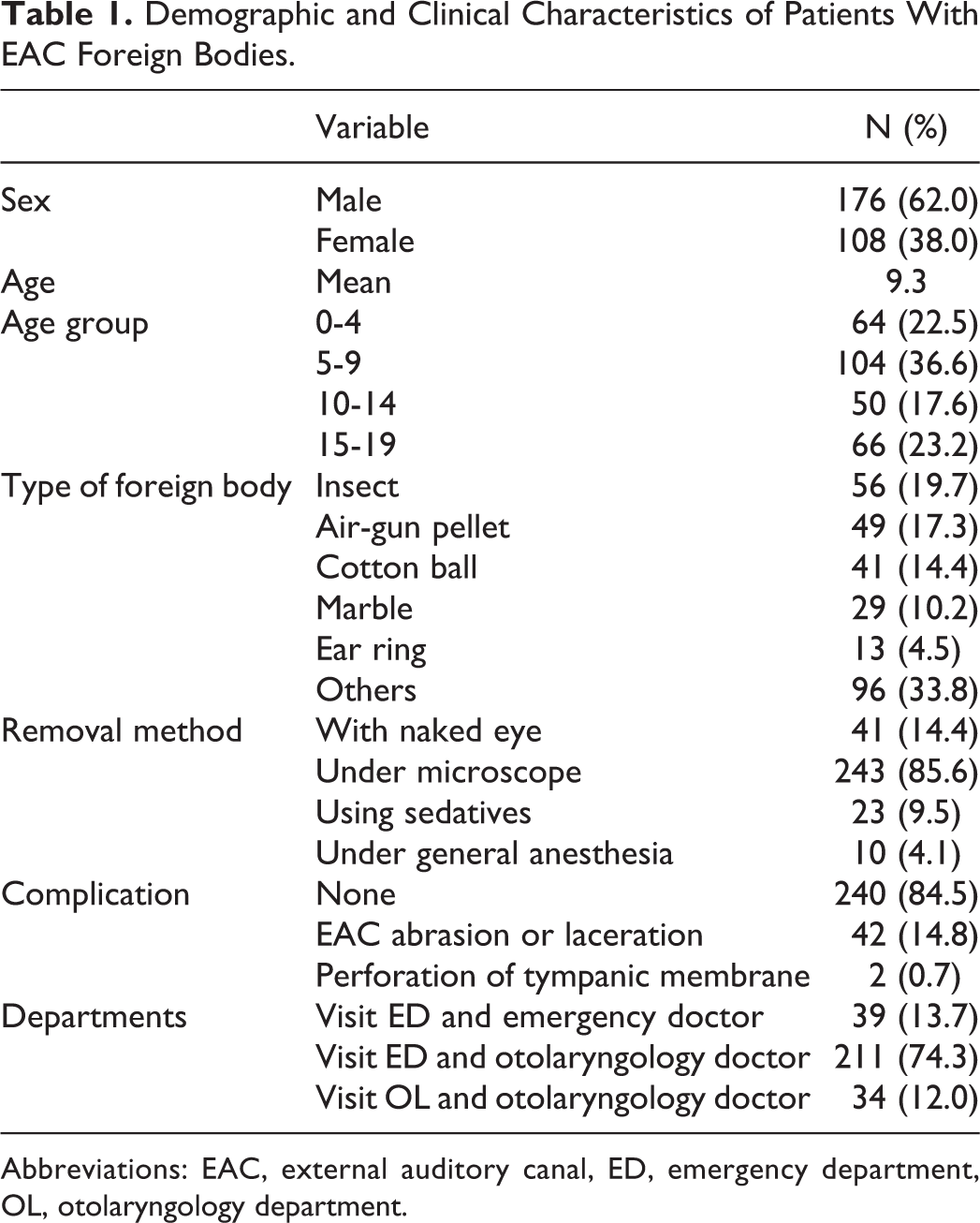
Abbreviations: EAC, external auditory canal, ED, emergency department, OL, otolaryngology department.
Age and Sex Distribution of EAC FBs
External auditory canal FBs were most frequently encountered at ages of 5 to 9 years (36.6%), followed by 15 to 19 (23.2%), 0 to 4 (22.5%), and 10 to 14 (17.6%). There were 2 peak incidences: at ages 3 to 6 and 17 to 18 (Figure 1). The proportion of male patients was higher at most ages, but females predominated among 16- and 17-year-olds (Figure 1).
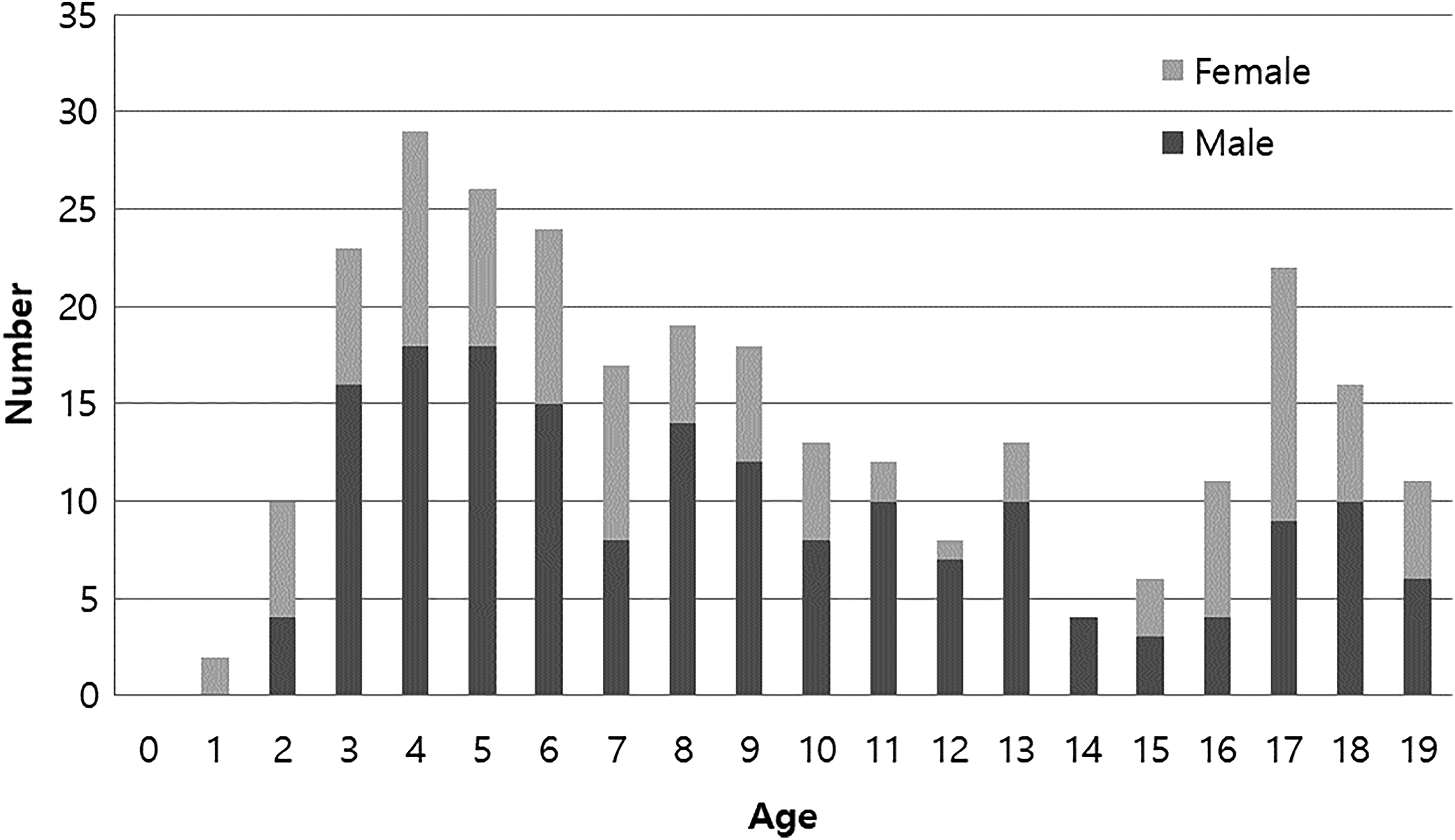
Incidence of external auditory canal foreign body according to age.
Classification of EAC FBs
Various kinds of materials, and insects, were identified as EAC FBs. Among the 15- to 19-year-olds, insects (34.8%), cotton balls (30.3%), and earring parts (15.2%) were more common than air-gun pellets (0.0%) and marbles (6.1%). In contrast, a high proportion of air-gun pellets (23.4%) and marbles (25%) were encountered in 0- to 4-year-olds (Table 2).
Types of Foreign Body by Age-Group.
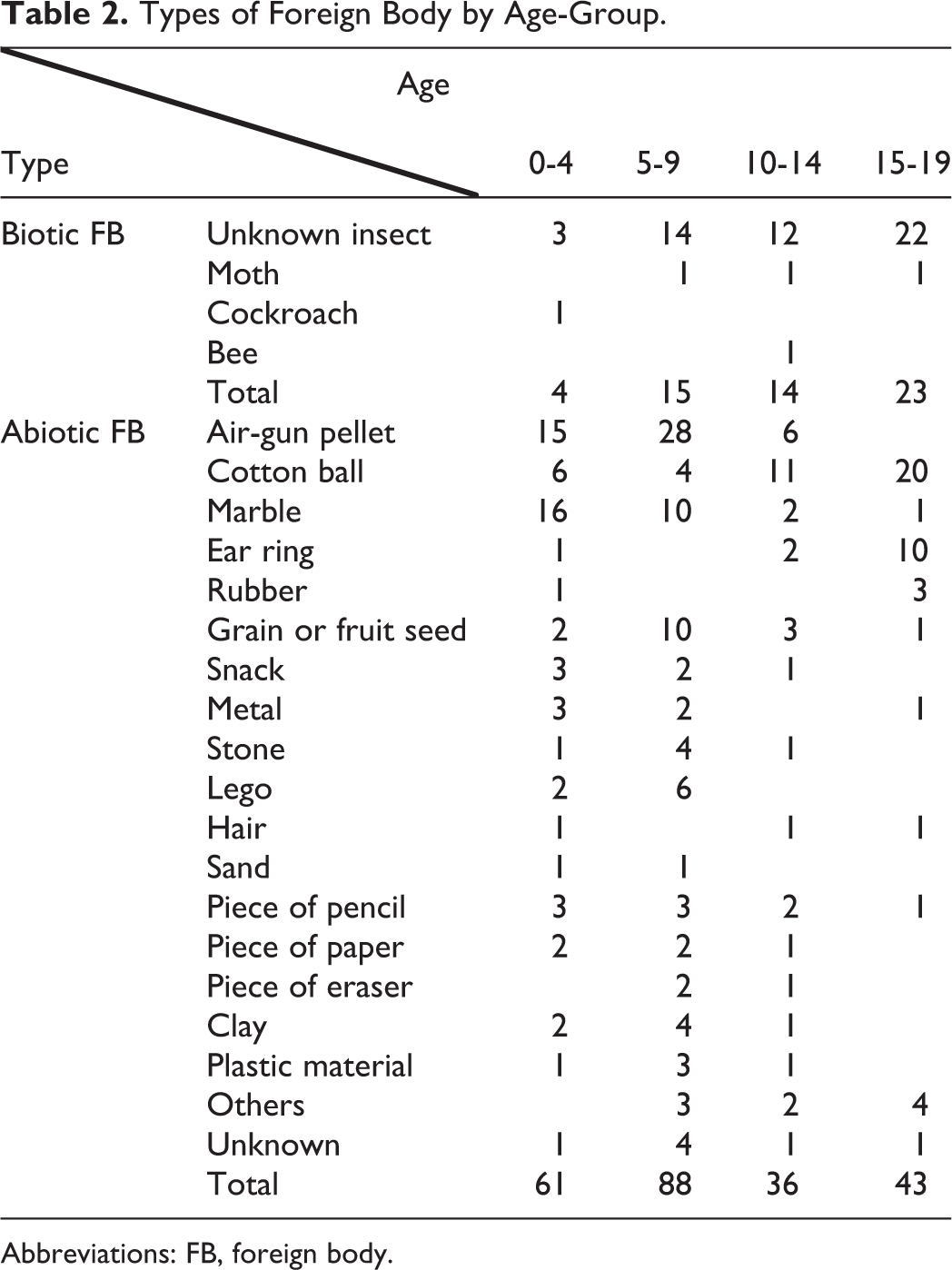
Abbreviations: FB, foreign body.
Management and Complications of EAC FBs
Patients who needed sedatives during the removal procedure ranged between 3 and 13 years of age. And those needing general anesthesia ranged from 5 to 11 years. No infants younger than 3 years, or adolescent older than 13 years, needed sedation (Figure 2).
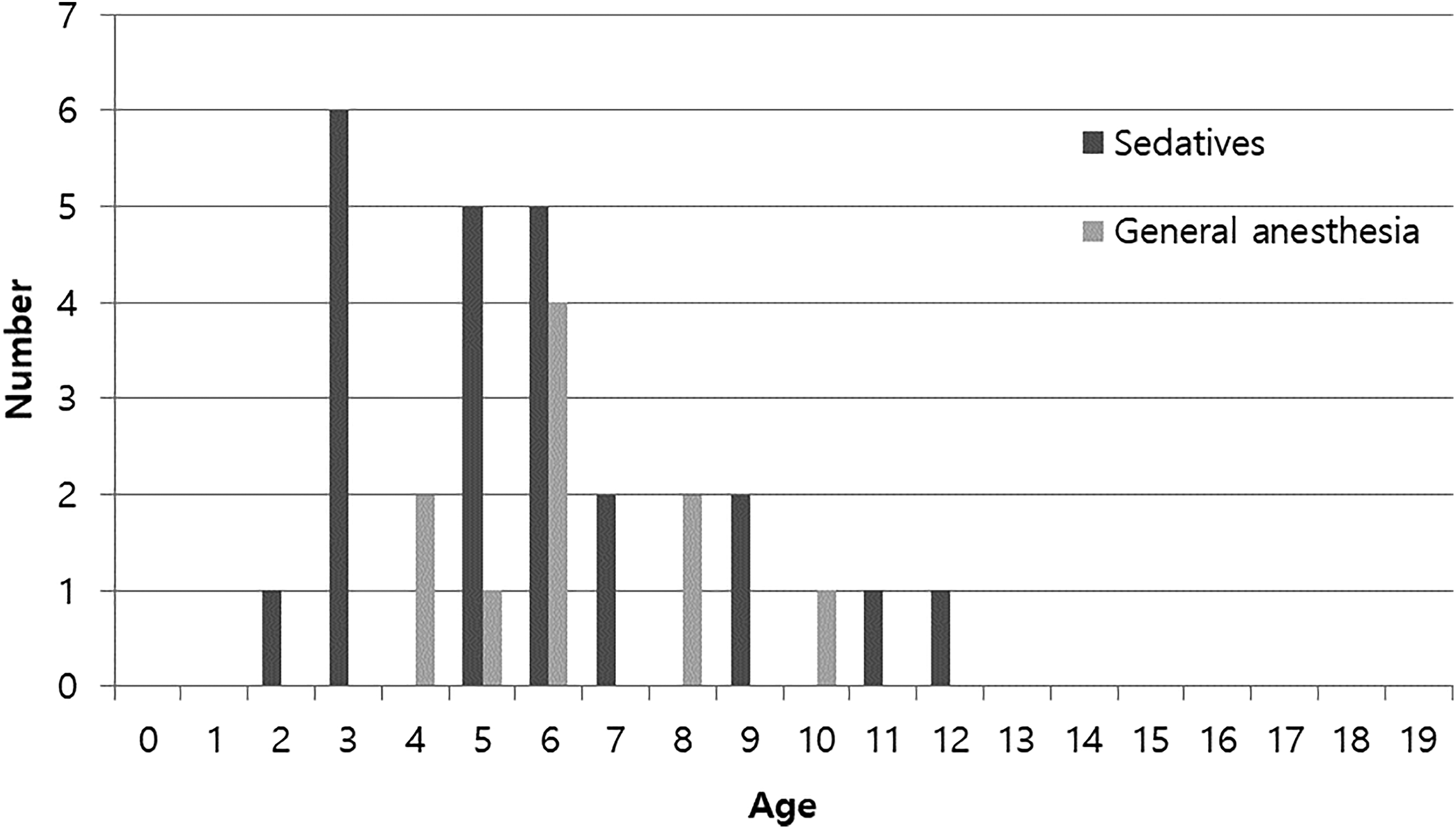
Distribution of patients needing sedation or general anesthesia according to age.
Complications developed in 44 patients after their procedure. External auditory canal abrasions and lacerations were most common among 5- to 9-year-olds (27.9%) followed by 0- to 4-year-olds (15.6%). Complications occurred frequently in cases involving earrings (23.1%). There were 2 instances of tympanic membrane perforation: a 7-year-old girl with an insect FB and a 6-year old girl with a kernel of corn in the EAC (Tables 3 and 4).
Incidence of Complications According to Age-Group.
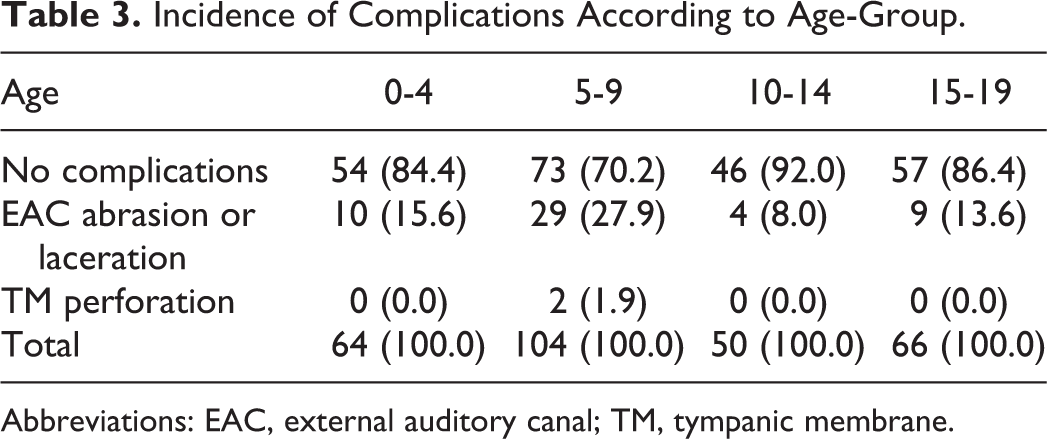
Abbreviations: EAC, external auditory canal; TM, tympanic membrane.
Incidence of Complications According to Foreign Body Type.

Abbreviations: EAC, external auditory canal; TM, tympanic membrane.
Discussion
In this study, we reviewed the clinical characteristics of EAC FBs. The core findings can be summarized as follows: (1) There were 2 peaks of EAC FBs, at ages 3 to 6 years and 17 to 18 years. (2) Complications during FB removal were frequent in the patients with EAC FBs aged 5 to 9 years. (3) The frequency of EAC FBs was higher in male than in female children, but more adolescents were female than male.
Foreign bodies in the EAC are very common and sufferers tend to visit hospital promptly because the effects are really annoying and sometimes painful. 10,11 A previous study showed that 85.9% of all aural FBs occurred in children, and the majority of the latter were aged 5 to 9 years. 7 The authors suggested that EAC FBs are more frequent in younger children because they are curious and careless. The results of the present study were consonant with those of the previous study, but we observed 2 peaks of incidence, at 3 to 6 years and 17 to 18 years. Interestingly, male patients predominated overall, however, in the second peak of incidence the majority were females, as shown in Figure 1. This might result from the fact that earrings and piercings are common in adolescent girls. 12
Our study also showed that the types of FB varied according to the age of patients, as have others. 12,13 Children younger than 10 years tend to have FBs related to toys such as air-gun pellets and marbles. 14 With age, the proportion of toys decreased while cotton balls, insects, and earring materials increased. 14 The increase of cotton balls may result from more frequent “self-picking” and the increase in insects from the fact that adolescents are more often involved in outdoor activities and have wider EAC diameters than younger children.
It is usually not difficult to remove FBs under a microscope, especially in adults. In younger children or adolescents, however, one must be more careful because they find it difficult to stay still. 15 Especially when the FB is sharp or impacted, one needs to think about the appropriate removal method and instrument to minimize complications. 6,16,17 In the present study, complications during FB removal were most frequent in 5- to 9-year-olds, who are less cooperative than other age-groups. Moreover, younger patients received sedation or general anesthesia more frequently. In the present study, sedatives were used step by step according to the sedation protocol of the children. Chloral hydrate was used firstly, and ketamine or midazolam were used when chloral hydrate did not effect. If none of these sedatives worked, EAC FBs were removed under general anesthesia.
Regarding injuries during FB removal, earrings were the most frequent cause, and cotton balls were less often the cause, suggesting that the characteristics of FB’s affect the complication rate. In this regard, animate FBs tend to cause complications more frequently than inanimate ones. 14,18 However, in the present study, insects did not cause many complications. Complication rates depend on many factors including patient age, nature of FB, the instrument used, and the skill of the practitioner. However, the most important factors influencing the complication rate seem to be the patient’s age and the degree of cooperation. 2,19
Various instruments can be used to remove aural FBs, including alligator forceps, cerumen loops, right-angle ball hooks, and so on. After making sure that the tympanic membrane is intact, aural irrigation can be useful for removing friable FBs like insects and tissue paper. However, batteries or hygroscopic objects should never be irrigated; aural irrigation can expand the volume of hygroscopic objects such as vegetables, beans, or other food materials, and cause them to be impacted in the EAC, making them more difficult to remove. 5,17
In this study, 14.4% of EAC FBs were removed without microscope. Cotton balls or FBs not stuck in the EAC could be easily removed with otoscope and Bayonet forceps. However, cases of FBs near tympanic membrane or presence of secondary inflammation have to recommend consulting an otolaryngologist. Previous reports have recommended prompt referral to an otolaryngologist to minimize complications. One study reported a complication rate of 15.7% when the procedure was performed by otolaryngologists, compared with 68.1% for nonotolaryngologists. 19 Another study suggested that multiple attempts by nonspecialists can reduce patient cooperation and make subsequent procedures more difficult. 5 In the current study, the incompleteness of the medical records made it difficult to check whether complications involved nonotolaryngologists or otolaryngologists. But there is no doubt that early referral to otolaryngologists can reduce complications considerably. 1
Interestingly, a recent analysis of health insurance claims showed that patients with attention deficit hyperactivity disorder (ADHD) were at high risk of insertion FBs in the nose and ears. 20 The authors recommended that ADHD should be considered in children with EAC FBs, and that comorbidities should be thoroughly reviewed. 20 In addition, it is known that children from low-income families are more likely to present with EAC FBs. 20
The limitations of this study were its retrospective nature, which may have decreased the power of the evidence. Also, the complication rate we observed in this study could have been overestimated or underestimated because it was unclear whether the complications arose due to the characteristics (sharp or insect) of the FBs or to struggling during removal. Despite these limitations, the present study reveals important epidemiological characteristics and outcomes of EAC FBs in a single institution.
Conclusion
Various materials and insects were identified among EAC FBs. Choosing the removal method appropriate to the patient’s age and type of FB is essential to minimize complications. 21 Moreover, in children and adolescents who behave uncooperatively, we should not hesitate to administer sedatives or put them under general anesthesia. 8,22
Footnotes
Authors’ Note
This article was presented in International Congress of OR-HNS 2019 organized by Korean Society of Otorhinolaryngology—Head and Neck Surgery. The authors hold rights to publish the full manuscript. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education(NRF-2017R1D1A1B03033051).