
Abstract
Introduction and Background
Currently, cochlear implantation is the standard intervention for hearing restoration in patients with hearing loss. A cochlear implant is an important intervention to improve hearing in individuals with profound congenital or pediatric hearing loss. According to published reports, cochlear implant surgery has been considered a safe treatment associated with an approximately 1.6% complication rate. 1 Widely reported major complications include cerebrospinal fluid (CSF) leakage, facial nerve damage, skin necrosis, device failure (requiring explantation), postoperative meningitis, and hemorrhage.2,3 These complications have been reported to occur more frequently in patients with congenital anomalies such as incomplete partition deformity, joint cavity, and large vestibular aqueduct syndrome. 4 The occurrence of complications presents a significant challenge to surgeons and may affect postoperative patient outcomes.
CSF leakage refers to the intraoperative leakage of the CSF from the cochleostomy site. The leakage is caused by abnormal communication between the perilymph in the cochlea and CSF. The gentle flow of the fluid during cochlear implant surgery is called “oozing.” However, a profuse and rapid fluid flow during cochleostomy is called a “gusher.” 5 Prior to the development of cochlear implantation, the complication was referred to as “perilymphatic gusher” and occurred during stapedectomy. In cases of CSF gusher, the fluid flowing out of the inner ear is not the perilymph, but the CSF. 6 Miyamoto et al 7 reported the first case of CSF gusher during cochlear implantation in a patient with Mondini deformity in the inner ear. CSF gusher is a common complication developed during cochlear implant surgery. 8
Literature reports have shown that bony deformities in the fundus of the internal acoustic canal, such as common cavity defect, enlarged vestibular aqueduct, and Mondini dysplasia, are associated with an increased incidence of CSF gusher.8,9 According to previous reports, the incidence rate of CSF gusher ranges between 1% to 5%, 3 but the presence of inner-ear malformation (IEM) potentially increases the incidence rate up to 40%. 10 Patients who develop CSF gushers during cochlear implantation may have an increased risk of meningitis, incomplete electrode insertion, fewer active electrodes, poor receptive vocabulary acquisition, and poor speech perception.11,12 Therefore, it is crucial to identify risk factors associated with CSF gushers during cochleostomy and develop intense management strategies.
The objective of this systematic review and meta-analysis was to evaluate the incidence of CSF gusher, risk factors that predispose patients to CSF gusher, and outcomes in patients during cochlear implant surgery.
Materials and Methods
Study Design
This systematic review and meta-analysis were guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework (Supplemental Material). 13
Information Sources and Search Strategy
A comprehensive literature search was conducted on PubMed and Google Scholar to discover relevant studies using the Boolean logics “AND” and “OR” with keywords such as “Cerebrospinal fluid gusher” AND “cochlear implantation” OR “cochleostomy.” The search was limited to reports published in the English Language from 2003 to 2023. The reference lists of the full-text articles were manually screened to identify any potentially relevant articles that were missed by the initial search strategy.
Eligibility Criteria
Population-Intervention-Comparators-Outcomes-Study (PICOS) eligibility model 14 was used to assess the eligibility of full-text articles, as shown in Table 1 below.
Eligibility Criteria Based on PICOS.
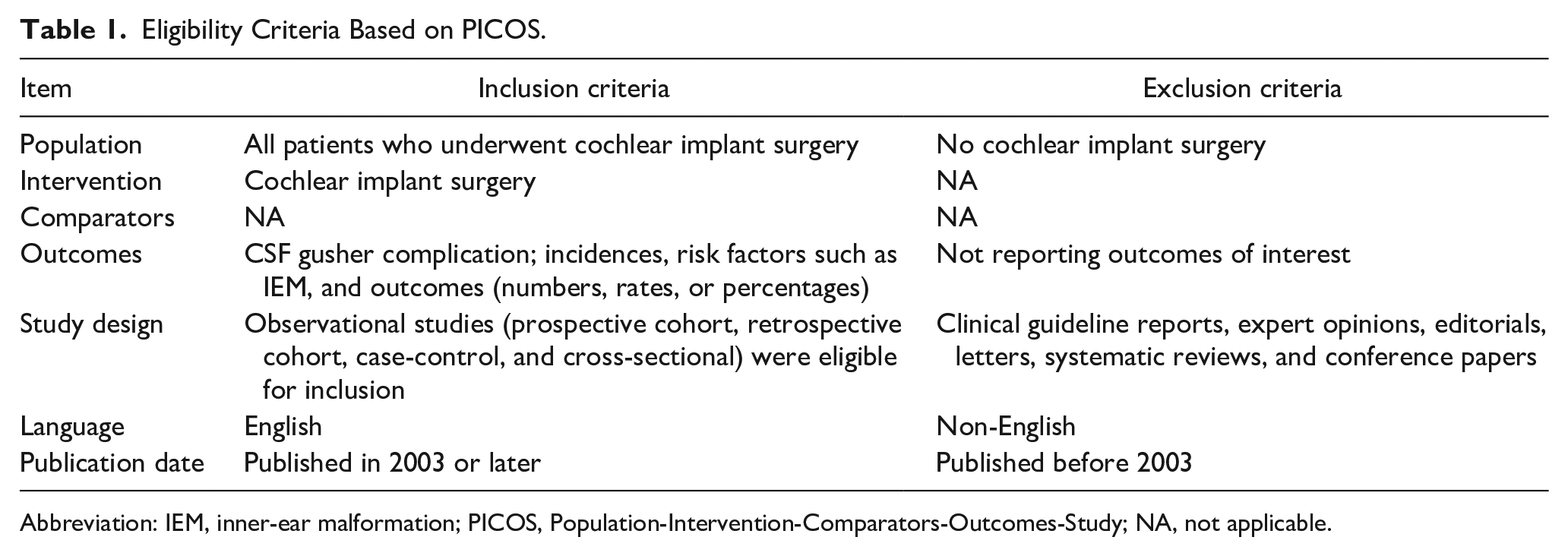
Abbreviation: IEM, inner-ear malformation; PICOS, Population-Intervention-Comparators-Outcomes-Study; NA, not applicable.
Study Selection and Data Extraction
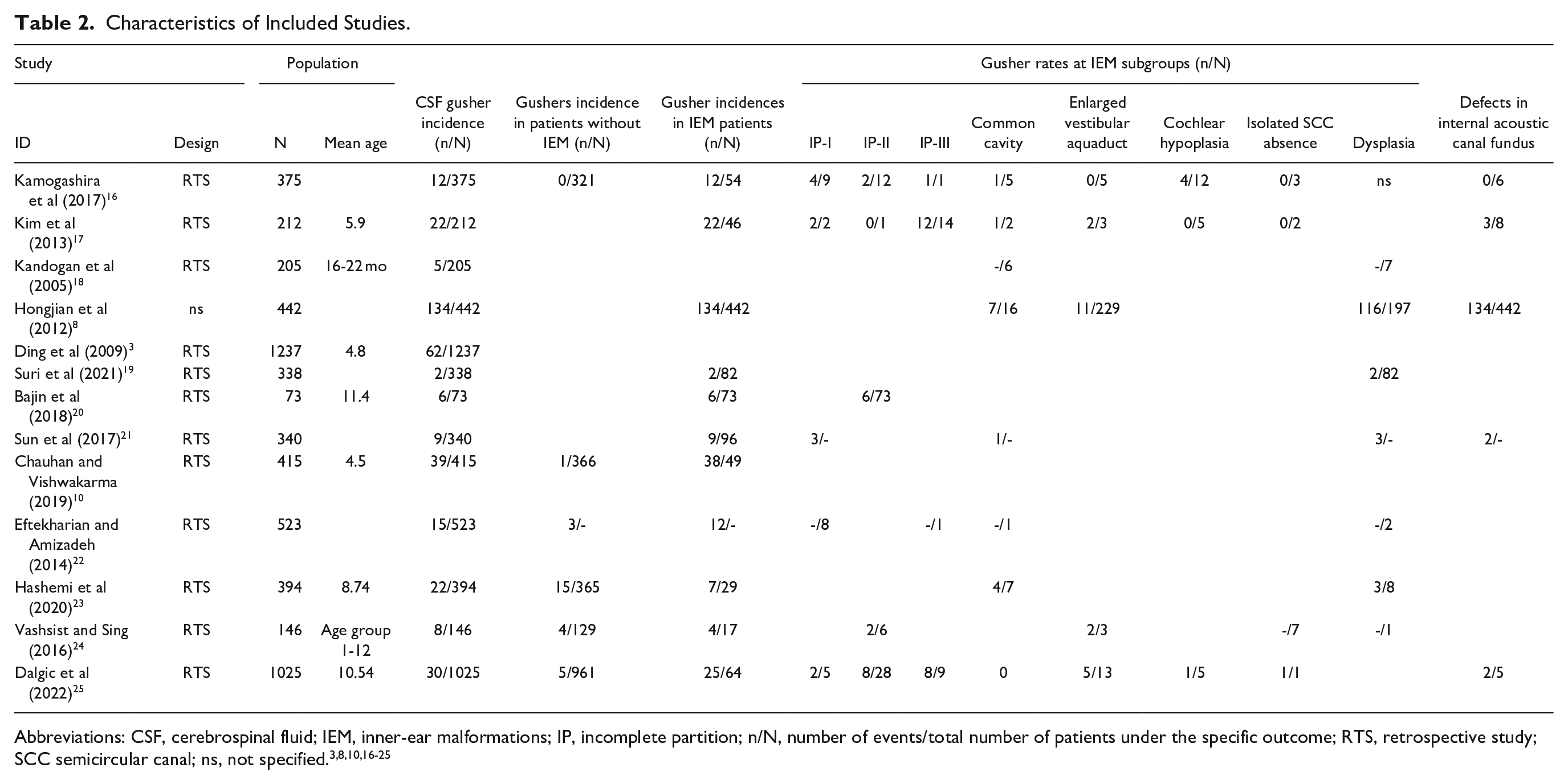
Relevant studies used in the review and analysis were identified using the predefined PICOS inclusion. Relevant data was extracted and filled into a table, including study ID, design, population characteristics (number, age), CSF gusher incidences, and associated risk factors, majorly IEM (Table 2).
Characteristics of Included Studies.
Risk of Bias Assessment
The Newcastle-Ottawa Scale (NOS) was used to assess the risk of bias in all the retrospective studies used in this systematic review and meta-analysis. This was important to identify any potential risk of bias in participant selection, comparability, or outcomes reporting.
Statistical Analysis
The review manager software (RevMan version 5.4) and rBiostatistics 15 were used to perform the meta-analysis. The odds ratios (ORs) and proportions were generated with a 95% confidence interval (95% CI), and the forest plots were used to analyze the pooled effect of the statistical data from included studies. The I2 statistic was used to determine the heterogeneity between studies. I2 < 50% indicated no significant heterogeneity among the studies, 50% ≤ I2 < 75% showed moderate heterogeneity, while I2 ≥ 75% meant a high considerable heterogeneity.
Results and Findings
Search Results
The database searches identified a total of 975 studies (908 from Google Scholar and 67 from PubMed), of which 153 duplicate articles were excluded. Additionally, 724 studies were removed after the title and abstract screening. Ninety-eight studies were set for full-text retrieval, but 53 full texts were not retrieved. The full texts of 45 successfully retrieved publications were assessed for eligibility using the predefined PICOS inclusion criteria. Of these 45 articles, 32 did not meet the eligibility criteria outlined and were excluded. The remaining 13 pertinent articles were included in this systematic review and meta-analysis. The PRISMA-guided study selection process is shown in Figure 1 below, while Table 2 shows the fundamental characteristics of the studies used and key data extracted for this analysis.3,8,10,16-25
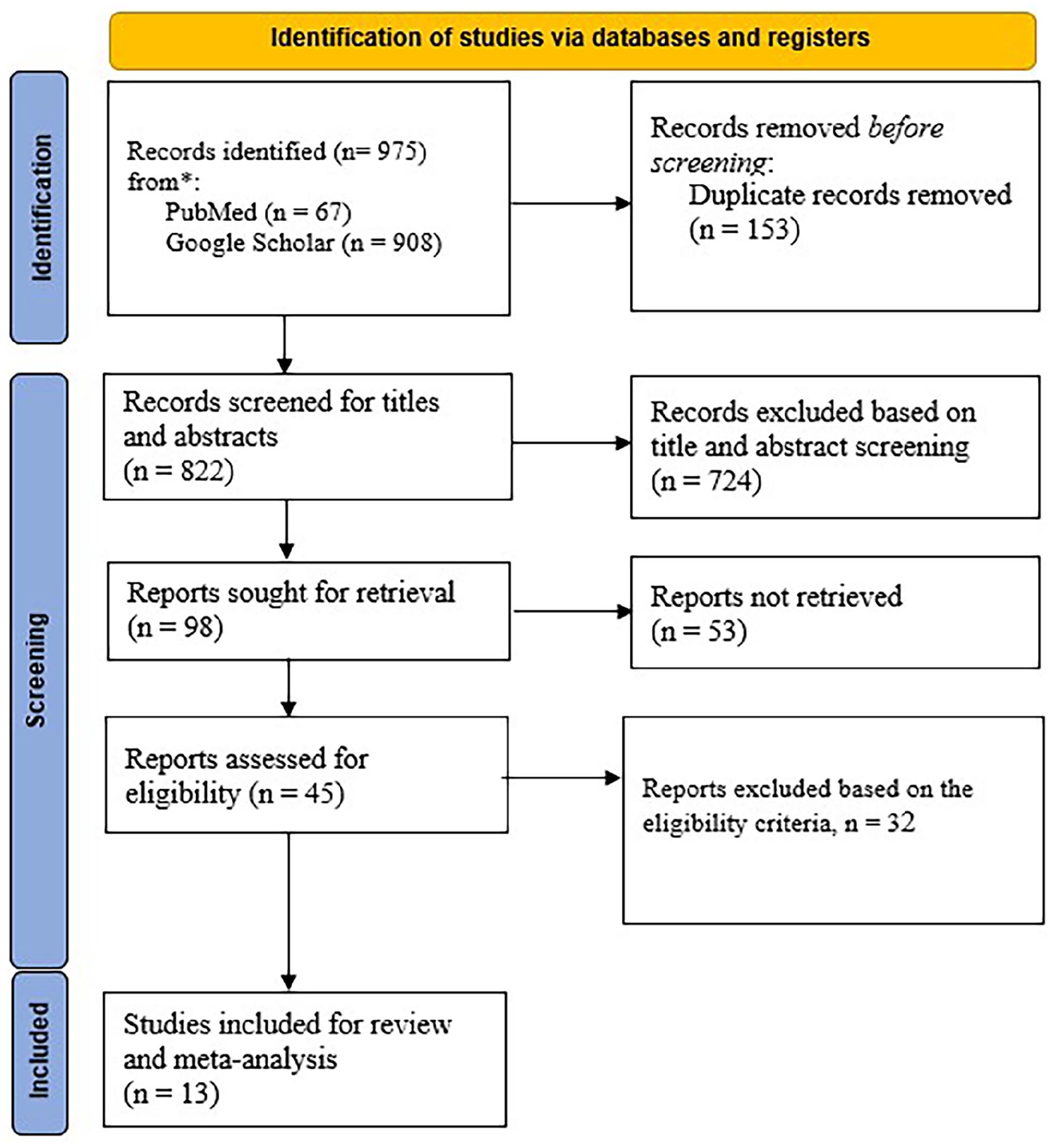
PRISMA-guided study selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quality Assessment
The quality assessment of the retrospective studies was performed according to the NOS to assess bias in the selection of patients, comparability, and outcomes (Figure 2). Scores were given, and the overall scores were judged to determine the study quality. Studies with a score <4 were low quality, 5 to 6 moderate qualities, while 7 to 9 were high quality.
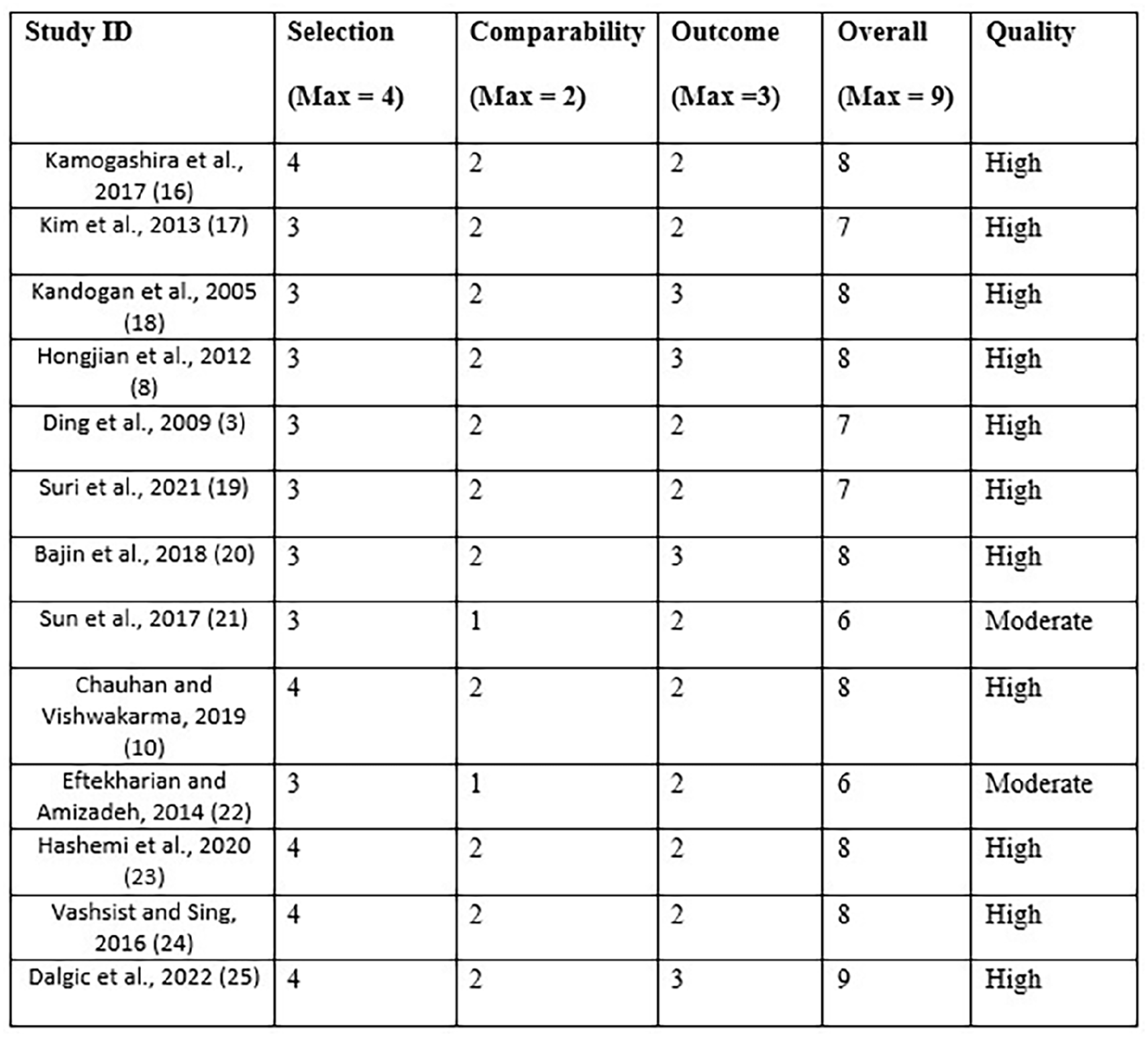
Quality appraisal of the included studies using NOS. NOS, Newcastle-Ottawa Scale.
Meta-Analysis Results
Incidence Rate of CSF Gushers
The pooled analysis of the sources reviewed found the incidence rate of CSF gushers among the general population to be 5% (95% CI: 3%-9%), considering the random effect model, using the statistical data from 13 studies analyzed in this article. Figure 3 below shows the forest plot of the incidence rate of CSF gushers reported across the studies. However, the heterogeneity among the studies was significant (I2 = 97%, P < .01).
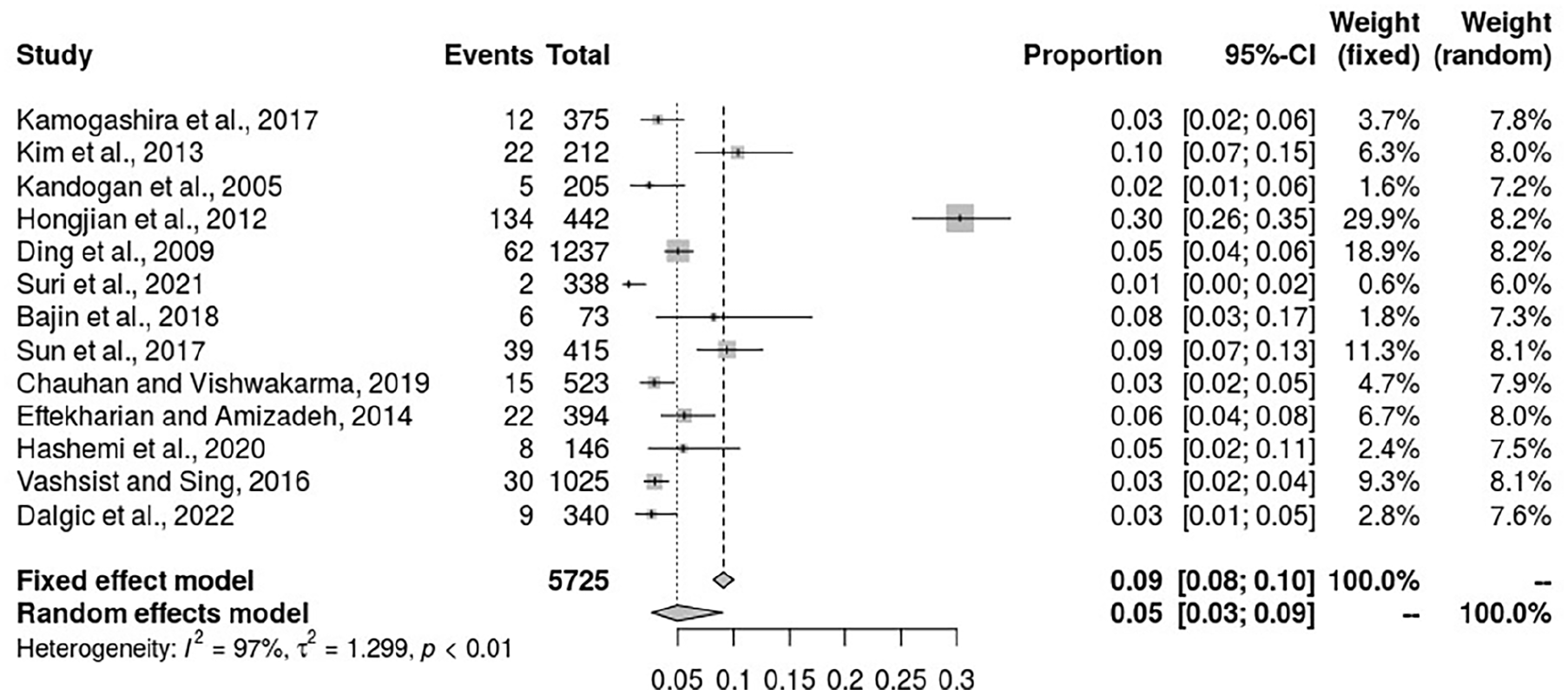
Forest plot for the incidence rate of CSF gushers reported across 13 studies. CSF, cerebrospinal fluid.
Comparison of the Incidences of CSF Gushers Between Patients With IEM Versus Patients Without IEM
IEM has been reported as a risk factor for developing CSF gushers during cochlear surgery. Consequently, a meta-analysis was conducted using data from 5 studies. The result of this analysis found a significantly higher incidence rate of CSF gushers among patients with IEM (40.37%; 86/213) during cochlear surgery compared to patients without IEM (1.17%; 25/2142), with a significant heterogeneity found among the studies OR = 63.01 (95% CI: 9.85-403.11, P < .00001, I2 = 88%). A total of 86 cases of CSF gusher were reported out of the 213 patients with IEM (40.38%) compared to only 25 patients out of 2142 (1.17%) without IEM. This implies a significant association between the incidence of CSF gushers and IEM for patients receiving cochlear implants (see Figure 4).
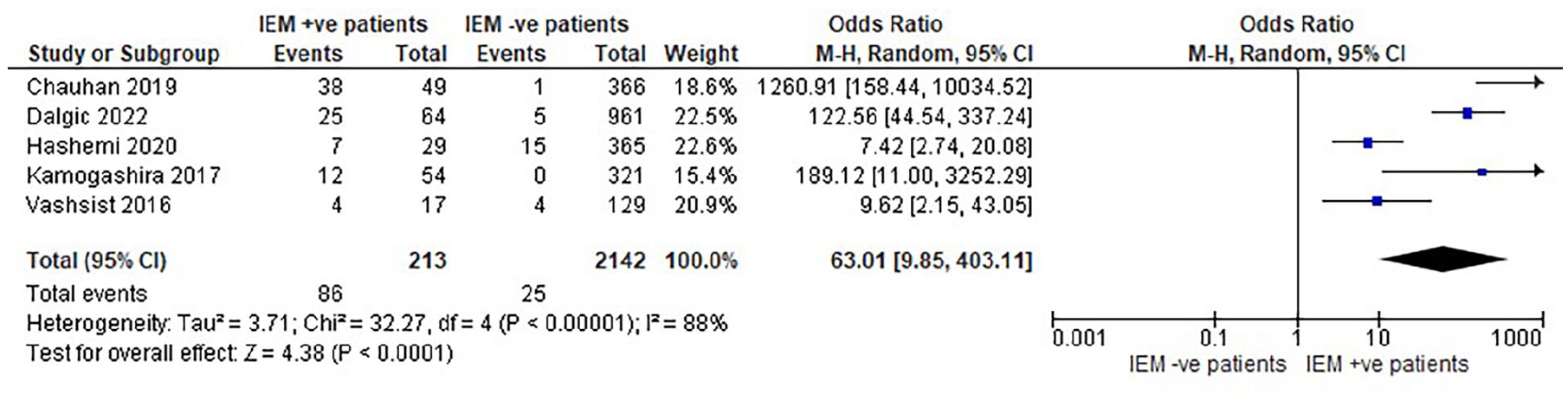
Forest plot showing the comparison of CSF gusher incidences between patients with IEM and those without IEM. CSF, cerebrospinal fluid; IEM, inner-ear malformation.
Comparison of Incidence of CSF Gushers Between Patients with IEM Versus the Entire Population
Further, a meta-analysis was performed using 8 studies to compare the incidence of CSF gushers among patients with IEM with that of the entire population included in these studies. The results showed a significantly higher incidence of CSF gushers in patients with IEM who received cochlear implants than the group of patients without IEM who underwent the same operative procedure, with a significant heterogeneity existing across studies, OR = 9.35 (95% CI: 5.15-16.97, P = 0.001, I2 = 77%). This further affirms the association between the existence of IEM and the increased risk of developing CSF gushers during operative procedures in cochlear implants (Figure 5).
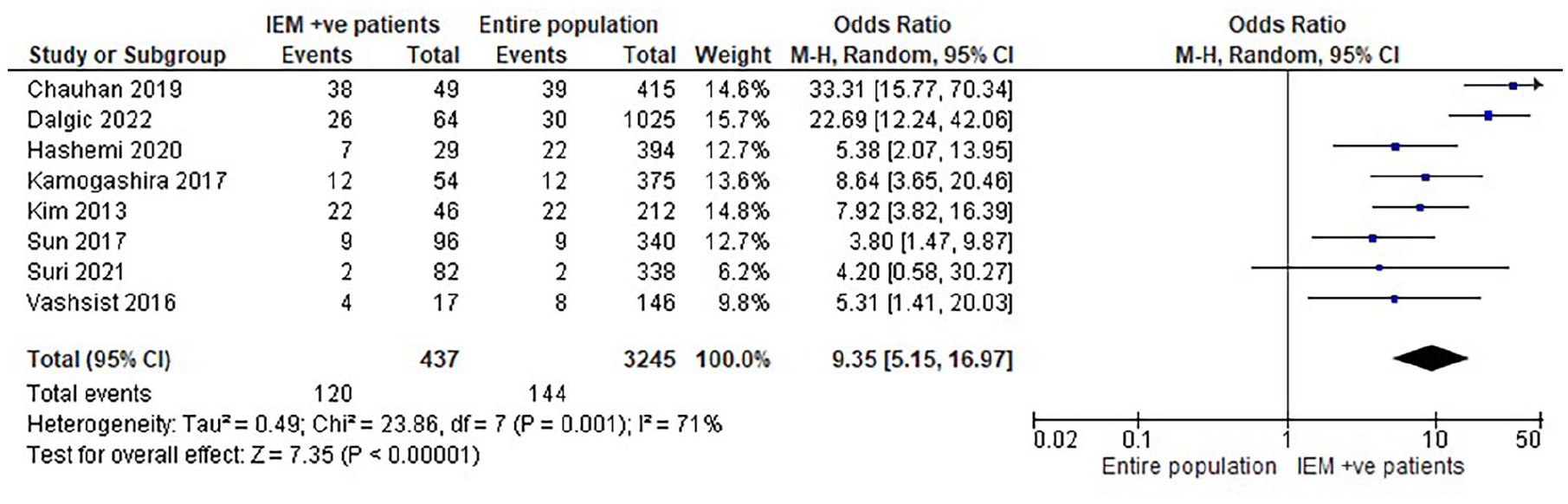
Forest plot of the comparison between the incidence rate of CSF gushers between patients with IEM and the entire population of patients receiving cochlear implants. CSF, cerebrospinal fluid; IEM, inner-ear malformation.
Association of IP-I with Risk of CSF Gushers in Patients During Cochlear Implant Operation
The incidence of CSF gushers in patients with IP-I receiving cochlea implants was 48% (95% CI: 25%-71%, I2 = 0%) (Figure 6). This rate is significantly high, considering that the overall prevalence of CSF among all patients undergoing cochlea implantation was determined to be 5% (Figure 3). Therefore, patients with IP I could be at increased odds of experiencing CSF gusher during cochlear implantation compared to patients with normal internal ears.
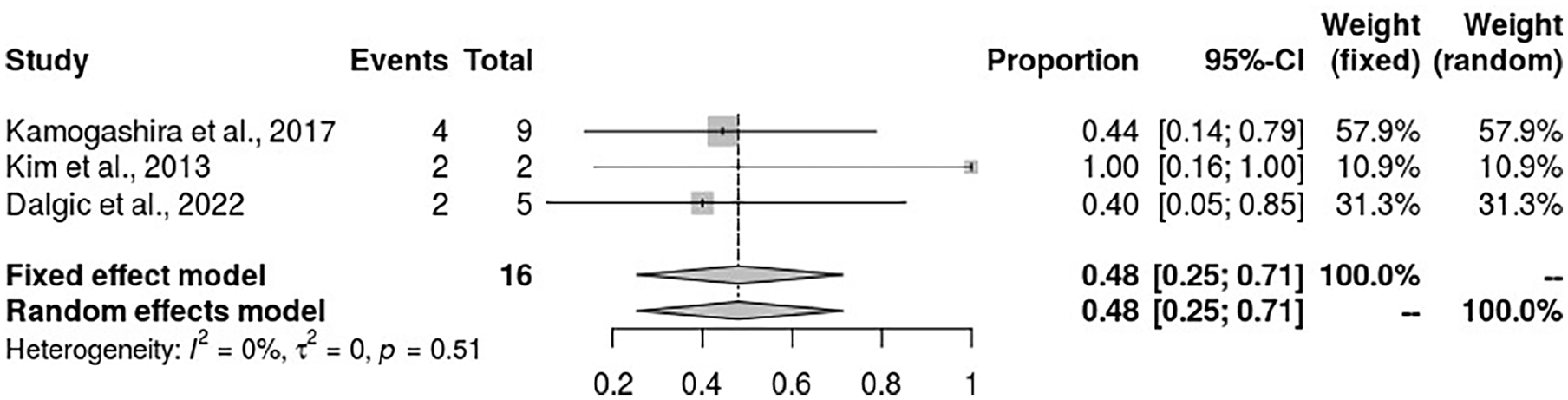
Forest plot showing the incidence rate of CSF gushers among patients with IP I during cochlear implant surgery. CSF, cerebrospinal fluid; IP, incomplete partition.
Association Between CSF Gushers and IP-II in Patients During Cochlear Implant
The incidence rate of CSF gushers in patients with IP-II receiving cochlear implants was 19% (95% CI: 9%-34%) (considering the random effect model) from the pooled analysis of 5 studies that reported the statistical data. The heterogeneity between the studies was insignificant (I2 = 46%) (Figure 7).
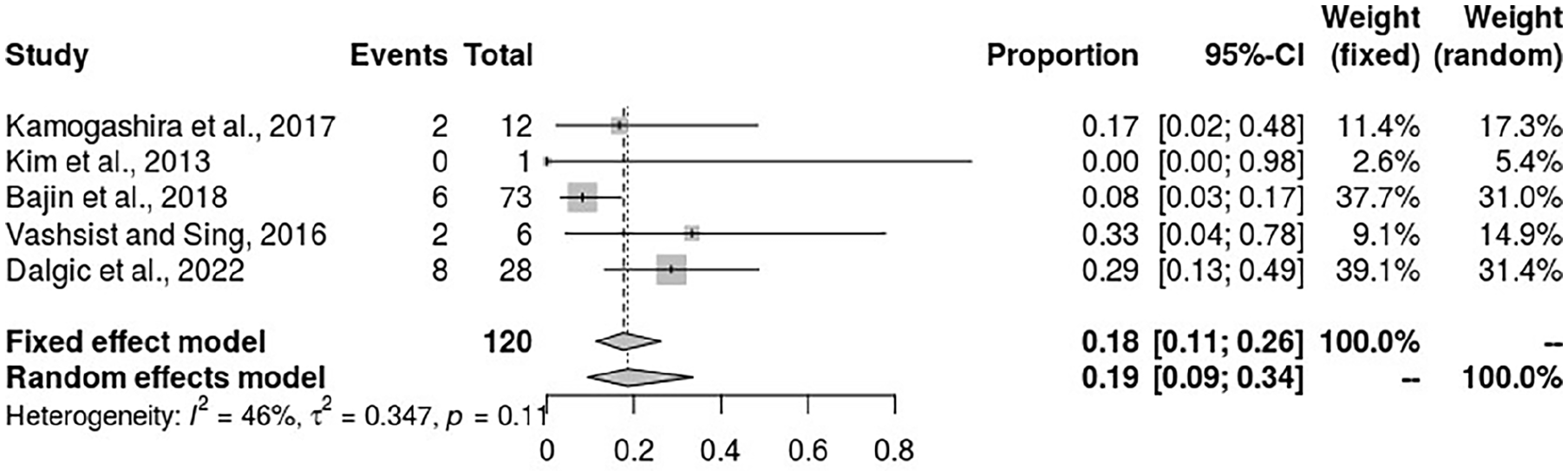
Forest plot showing the incidence of CSF gushers in patients with IP-II during cochlear implant. CSF, cerebrospinal fluid; IP, incomplete partition.
IP-III
Patients with IP-III were found to have the highest risk of experiencing CSF gushers during cochlear implant than all other IEM groupings. The meta-analysis results found an incidence rate of 86% (95% CI: 66%-95%), with no heterogeneity among the studies (I2 = 0%) (Figure 8). This finding shows that IP-III poses the highest risk for the occurrence of CSF gushers in patients during cochlear surgery.
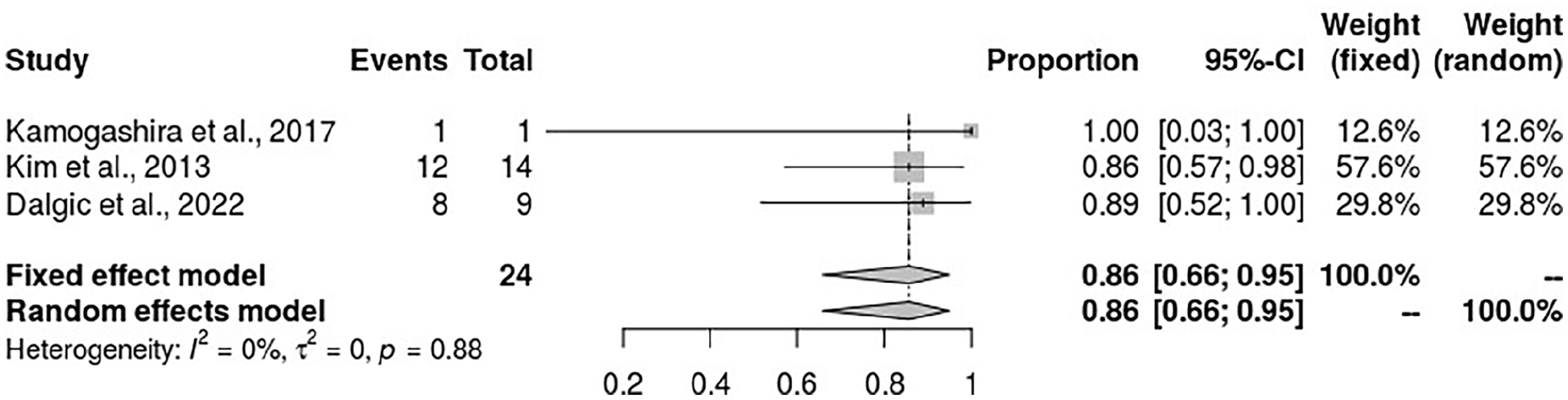
The forest plot for the incidence of CSF gushers in patients with IP-III receiving cochlear implants. CSF, cerebrospinal fluid; IP, incomplete partition.
Common Cavity and Incidence of CSF Gushers
The incidence of CSF gushers among patients with common cavities was also meta-analyzed to determine the influence of this anomaly and its association with the occurrence of CSF gushers. CSF gushers occurred in 40% of patients with common cavities (95% CI 22%-61%). There was no heterogeneity across the studies analyzed (I2 = 0%) (see Figure 9).
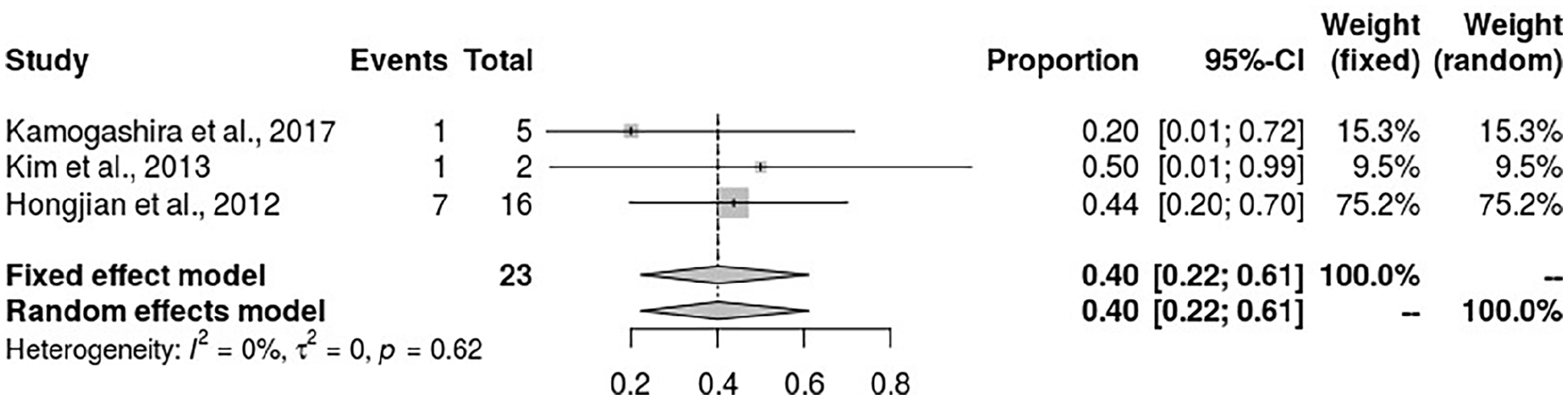
The forest plot for the association of common cavity and incidence of CSF gushers. CSF, cerebrospinal fluid.
Cochlear Hypoplasia and CSF Gushers
Cochlear hypoplasia also increases the odds of CSF gusher occurrence in patients receiving cochlear implants. The pooled analysis found an incidence rate of 26% (95% CI 12%-49%) (see Figure 10). This result suggests a significant risk of CSF gushers in patients with cochlear hypoplasia.
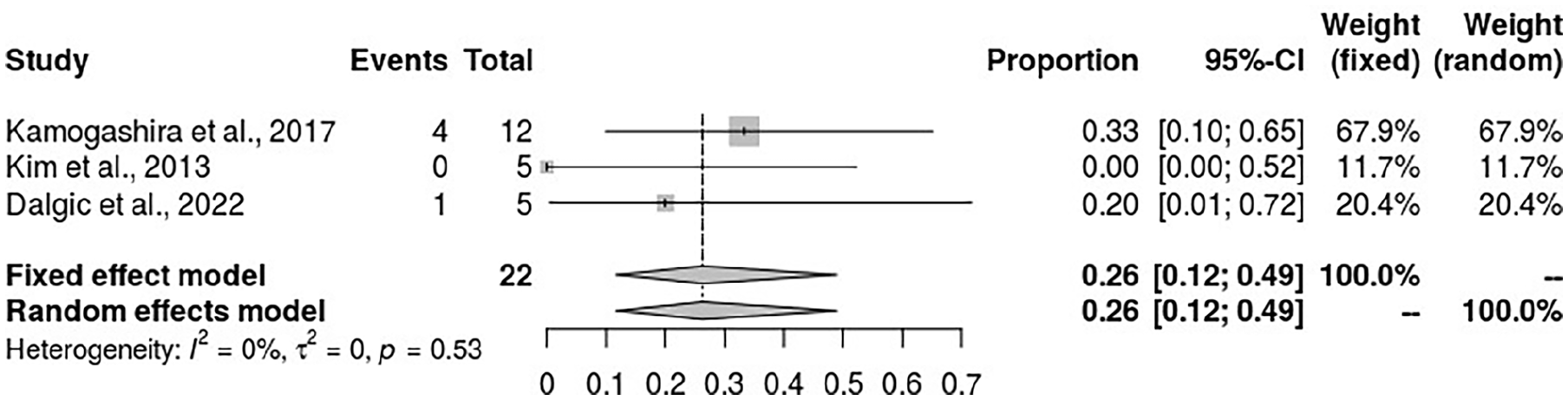
Forest plot for the association between incidences of CSF gushers and common cavity in patients undergoing cochlear implant. CSF, cerebrospinal fluid.
Enlarged Vestibular Acquadact and Incidences of CSF Gushers
Enlarged vestibular aqueduct was also associated with an increased risk of CSF gushers in patients receiving cochlear implants. The results from the meta-analysis of 5 articles revealed an incidence rate of 27% (95% CI: 6%-68%). However, the heterogeneity among the studies was highly significant (I2 = 85%) (see Figure 11).
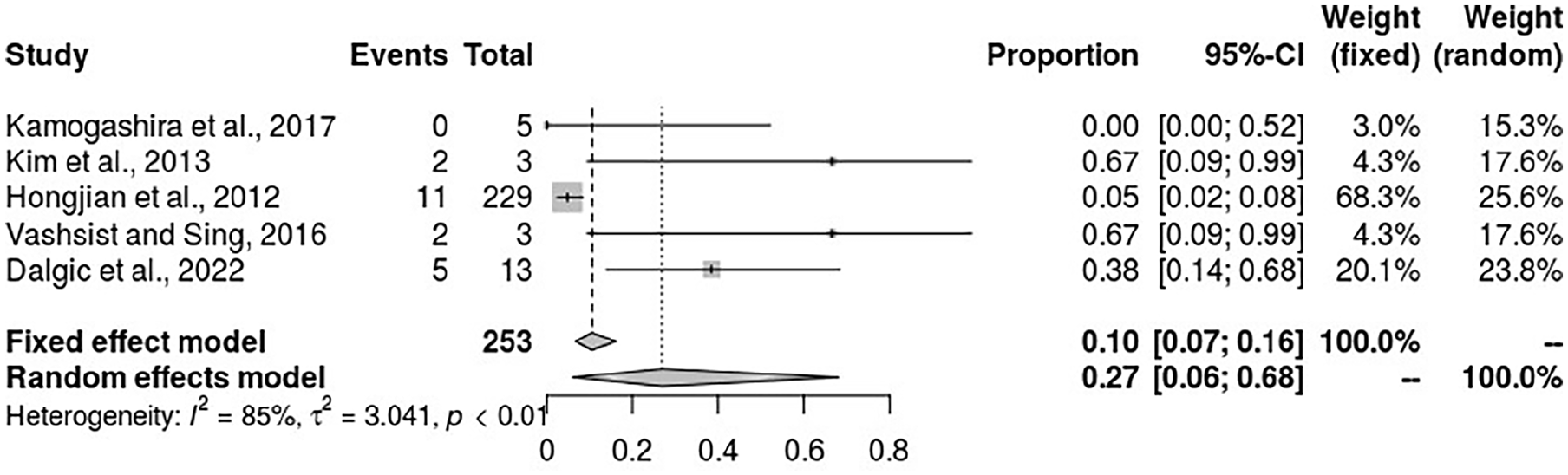
Forest plot for the association of enlarged vestibular aqueduct and incidence of CSF gushers. CSF, cerebrospinal fluid.
Defects in the Internal Acoustic Canal Fundus and CSF Gushers
Considering the random effect model, the incidence rate of CSF gushers in patients with defects in the internal acoustic canal fundus was found to be 73% (95% CI: 10%-98%), which is significantly higher than in the entire population, following the pooled analysis of 4 studies whose heterogeneity was significantly high, I2 = 85% (Figure 12).
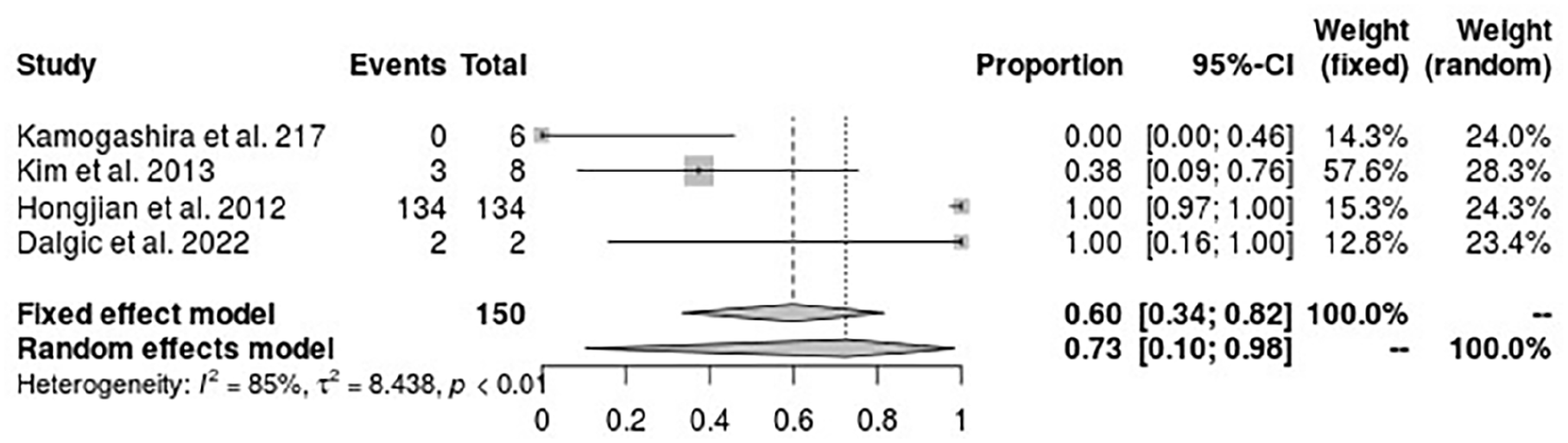
Forest plot for the incidence of CSF gushers in patients with defects in the internal acoustic canal fundus during cochlear implant. CSF, cerebrospinal fluid.
Discussion
The objective of this study was to evaluate the incidence of CSF gusher in patients during cochlea implantation and identify the risk factors that can predict the occurrence of CSF gusher as well as patient outcomes. The analysis was based on 13 studies that reported a total of 5725 patients who underwent cochlear implantation. According to the results of this meta-analysis, the incidence rate of CSF gusher was 5% (Figure 3). Further investigation revealed that the incidence rate of CSF gusher was much higher in patients who had IEM. According to the analysis data from 5 articles used in this study, CSF gusher incidence was significantly higher in cases with IEM OR = 63.01 (95% CI: 9.85-403.11, P < .00001, I2 = 88%) (Figure 4). Additionally, the incidence rate of CSF gusher was much higher in patients with IEM compared to the prevalence of CSF gusher in the general population of patients who received cochlea implants OR = 9.35 (95% CI: 5.15-16.97, P = 001, I2 = 77%) (Figure 5).
IEM has been identified as a predisposing factor for the development of CSF gusher. 24 The findings of this study have confirmed that IEM may increase the risk of CSF gushers. IEM categorizations include incomplete partition (3 types: IP-I, IP-II, and IP-III), cochlear hypoplasia, and common cavity malformations. In this study, the incidence rate of CSF gusher in patients with IEM was 27.46% (120/437), which was much higher than the incidence rate in patients without IEM 4.44% (144/3245) (Figure 5). Previous reports have suggested that gusher occurred in patients with deformities in the fundus of the internal acoustic canal or basal turn of the cochlear.26-28 This study found an incidence rate of 73% in patients with defects in the internal acoustic fundus (Figure 12).
Previous reports have indicated that the prevalence of CSF gusher was approximately 37% to 45.9% in patients with IP-I, 8% to 15% in those with IP-II, 100% in cases of IP-III, 23% to 27% in common cavity defects, 27% in cochlear hypoplasia, and 0% to 11% in cases with enlarged vestibular aqueduct.20,24,29-31 In the current study, the incidence of CSF gusher was found to be 48% in IP-I, 19% in IP-II, 86% in IP-III, 40% in the common cavity, 26% in cochlear hypoplasia, and 27% in patients with enlarged vestibula aqueduct (Figures 6-11). A similar trend was observed in the review by Sennaroglu et al, 4 who found that the incidence of CSF gusher was 40% in IP-I, 15% in IP-2, and 100% in IP-III. However, they did not report any cases of CSF gusher in patients with common cavity defects or enlarger vestibular aqueduct. Among the IEM group, there was a significantly higher incidence of CSF gusher in IP-III cases. Farhood et al previously performed a meta-analysis and found an incidence rate of CSF gusher of 45.9% in IP-I cases. The present study has found a 48% incidence rate of gusher in the IP-I group. 29 In this study, the incidence of gusher in patients with common cavity malformations was 40%. It is imagined that individuals with common cavity defects should be at a high risk of experiencing gusher due to common internal acoustic canal lateral wall anomalies. However, some studies,4,25,32 including a meta-analysis by Shi et al, 32 have reported lower rates of CSF gushers in patients with common cavity malformations.
In the context of the current findings concerning risk factors associated with CSF gushers, structural anomalies in the inner ear should alarm the surgeons to ensure precise preoperative scanning or imaging before cochlear implantations. Kamogashira et al suggested that computed tomography (CT) scans should provide malformation reports, including the absence of modiolus, large base of cochlea modiolar, and large vestibular aqueduct, which should be used to predict the potential risk of CSF gusher occurrence. 16
CSF gushers were managed successfully using various techniques across studies. For example, Eftekharian and Amizadeh 22 described the use of muscle blocks together with multiple small muscle pieces, while Vashist and Singh 24 managed all 9 cases of CSF gusher that occurred by packing 3 pieces of thin periosteum, which were packed around the electrode using a needle to form a complete seal. It has been reported that the occurrence of gushes may significantly diminish the residual hearing in patients.33,34 However, in this study, no statistical analysis was performed to investigate the postoperative outcomes of patients who develop CSF gushers during cochlear implant surgery due to insufficient statistical data to aid such investigation.
Study Limitations
This study has some limitations. First, available studies on CSF gushers in patients receiving cochlear implants are mostly retrospective in nature, which is justifiable since gathering such clinical data typically requires studies that are observational in nature. The retrospective nature of the studies used, and the small sample size present a risk of publication bias that may influence the findings. Moreover, the retrospective nature of the included studies means that results were recorded at a specified time during follow-up. Therefore, attrition or losing participants to follow-up would limit the accuracy and interpretation of the long-term results of retrospective studies. Another notable limitation is the small number of studies used in the analysis due to the limited number of published studies and the inconsistencies in the type of outcomes reported among the articles that provided numerical data employed in the statistical analysis. However, despite the small number of studies used in the analysis, the included studies give important insights into the incidence and risk factors of CSF gushers among specific patient populations who receive cochlear implants. Additionally, the heterogeneity of the studies has a limitation on further analysis and the implications of the study results. Also, some factors (such as onset or diagnosis age of deafness, residual hearing, preimplantation amplification, and age of implantation) that could have a bearing on the results have not been accounted for during the analysis.
Conclusion
CSF gusher occurred in 5% of patients during cochlear implantation. However, the prevalence of CSF gusher was considerably higher in patients with IEM, including IP, common cavity, and cochlea hypoplasia. Therefore, this study suggests accurate preoperative imaging and precise reporting of scanning results for patients with inner ear malformations to inform the necessary management and enhance better patient outcomes.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241292195 – Supplemental material for Retrospective Analysis of Cerebrospinal Gushers in Cochlear Implant Surgery: Incidence, Risk Factors, and Outcomes—A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-ear-10.1177_01455613241292195 for Retrospective Analysis of Cerebrospinal Gushers in Cochlear Implant Surgery: Incidence, Risk Factors, and Outcomes—A Systematic Review and Meta-analysis by Mohammed Hazazi, Eman Almashharawi, Saleh Alamry, Meshael M. Alkusayer, Alwaleed Altimyat and Yazeed Alsalamah in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Consideration
Our institution does not require ethical approval for conducting a meta-analysis, which is based on already published literature.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.