
Abstract
Objective:
To understand the anatomical and dimensional variations of the human inner ear using 3-dimensional (3D) segmentation within the Middle East population.
Design:
Retrospective study.
Setting:
King Abdullah Ear Specialist Center (KAESC) Riyadh, Saudi Arabia.
Participant:
Forty computed tomography (CT) images of patients with sensorineural hearing loss who underwent cochlear implant (CI) were taken for analysis.
Main outcome Measures:
Three-dimensional images showing the anatomical variations of the inner ear including various pathological conditions, cochlear parameters including basal turn diameter (“A” value), “B” value which is perpendicular to “A” value, cochlear height, length, and width of the internal auditory canal (IAC), intercochlear spacing, and electrode angular insertion depth (AID).
Results:
Out of 40 CT image data sets, 12 had normal inner-ear anatomy (NA), 4 with enlarged vestibular aqueduct syndrome (EVAS), 8 with only 2 turns of the cochlea (2TL), 7 with incomplete partition (IP) type II, 5 with cochlear hypoplasia, 1 with common cavity, and 3 with abnormal IAC. Taking the NA, EVAS, 2TL, and the IP type II cases altogether, age of the patient had no correlation with the “A” value; however, the “A” value had a linear correlation with the “B” value. The age of the patient had an increasing logarithmic correlation with the IAC length and the intercochlear spacing. The “A” value did not have any meaningful correlation with the cochlear height. Three data sets showed asymmetric inner-ear malformation types on either side of the ears. All these 40 cases were implanted with various CI electrode array variants and the corresponding postoperative plain film X-ray images showing the electrode AID are given separately in figures.
Conclusions:
Three-dimensional segmentation of the inner ear from the temporal bone CT is a valuable clinical and training tool for surgeons and radiologists especially in difficult cases which will certainly help to understand the overall anatomical and dimensional variations.
Introduction
Incidence rate of inner-ear malformation is reported to be around 20%, 1 and in country like China, the incidence rate goes as high as 30% as per report by Sun et al in 2015. 2 Reports by Sennaroglu et al, 3 Weber et al, 4 Isaiah et al, 5 Masuda et al, 6 Ramos et al, 7 Grover et al, 8 Aldhafeeri et al, 1 Quirk et al, 9 and Smeds et al 10 are the scientific proof that inner-ear malformation is a universal occurrence. Inner-ear malformation within cochlear implantation (CI) is a topic of importance when comes to surgeons who lack experience handling difficult cases. The main challenge is the mental compilation of a series of 2-dimensional image slices into a corresponding 3-dimensional (3D) anatomical structure in understanding the inner-ear anatomical variations.
The surgical complications with the inner-ear malformation types include endolymphatic oozing of perilymph and cerebrospinal fluid gusher if the vestibular aqueduct (VA) is enlarged 11 and the internal auditory canal (IAC) is wide open. 12 Electrode entering the IAC in inner-ear malformation types like common cavity (CC) 13 and incomplete partition (IP) type III 10 has been clinically reported. Electrode entering the vestibule in cases of IP with dilated vestibule 14 is also reported. In respect to all these aspects, a 3D image of the complete inner ear could help the surgeons and radiologists in getting a clear understanding on the anatomical malformations thereby minimizing the surgical complications. Three-dimensional segmentation of the inner ear as proposed by Dhanasingh et al 15 in understanding the overall anatomical variations is a valuable teaching tool especially for the surgeons who lack experience handling difficult cases.
In this study, we aim to identify the anatomical variations of the inner ear in general using the method of 3D segmentation from the computed tomography (CT) scans of patients within Saudi Arabia. From the 3D images of the inner ear, various dimensional analyses were performed to see if there is any mathematical relation between the various dimensions of the inner ear. We also investigated the postoperative X-ray images of the corresponding patients retrospectively to understand how the implanted electrode fits into these anatomical variations.
Materials and Methods
Forty temporal bones preoperative CT scans of patients with sensorineural hearing loss who were implanted with CI made available retrospectively from King Abdullah Ear Specialist Center Riyadh, Saudi Arabia. The age of the patients ranged from a minimum of 5 months to a maximum of 90 months. The 3D segmentation of the inner ear was performed using the freeware 3D slicer (https://www.slicer.org/). The CT images were loaded in the 3D slicer followed by the capturing of the inner ear from each slice by setting a tight gray-scale threshold. The details of the 3D segmentation process are given in detail elsewhere. 15 From the CT image, slices viewed in both oblique coronal and axial plane and the corresponding 3D images of the inner ear, the below given dimensions were measured by the first 2 authors together in agreement (Figure 1) using the ruler function in 3D slicer. The graphical plots and analyses were performed using Micro Soft Excel.
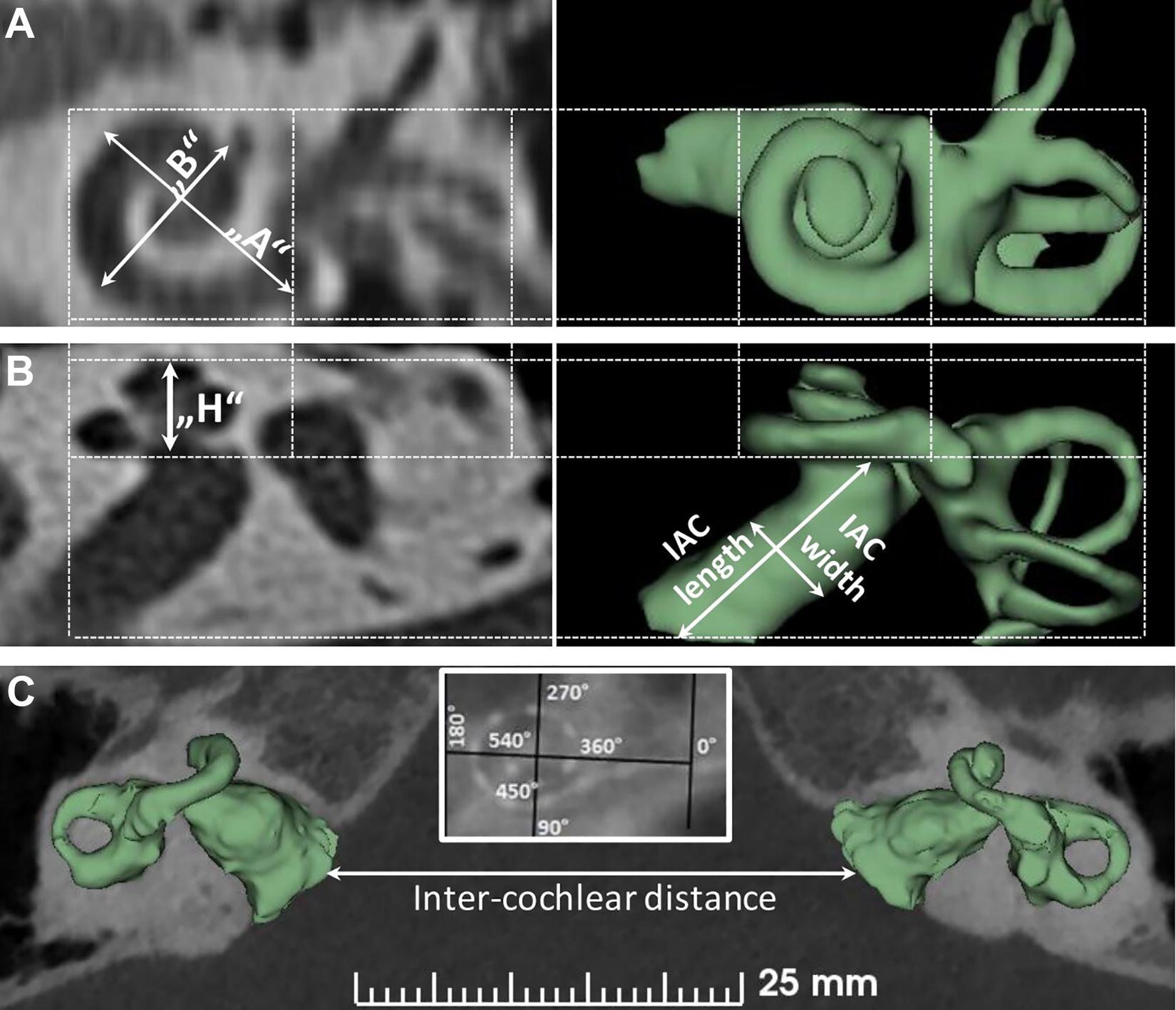
A, Inner ear visualized in the oblique coronal plane showing the “A” and “B” value. B, Inner ear visualized in the axial plane showing the cochlear height (H), length, and width of the IAC. C, Intercochlear distance measured from the tip to tip of the IAC between the ears in the axial plane. IAC indicates internal auditory canal.
“A” value/diameter of the basal turn: In the oblique coronal plane (Figure 1A, line starting from the middle of the round window (RW) membrane passing through the central modiolus to the other end of basal turn.
“B” value/width of the basal turn: In the oblique coronal plane (Figure 1A), line perpendicular to the “A” value again passing through the central modiolus.
Cochlear height: In the axial plane (Figure 1B), line measuring from the floor of the basal turn to the roof of the apex.
Length of the IAC: In the axial plane (Figure 1B), line measuring from the center of the fundus (top end) to the center of the bottom end of the IAC.
Width of the IAC: In the axial plane (Figure 1B), line measuring perpendicular to the IAC length along its center.
Intercochlear distance: In the axial plane (Figure 1C) with the cochlea seen through the mid-modiolus, line connecting the bottom end of the IAC from both the ears.
The electrode angular insertion depth (AID): Using postoperative X-ray image in the oblique coronal plane (Figure 1C-inside picture), 0° starting at the RW entrance. A line connecting the RW entrance passing through the central modiolus and reaching the opposite end makes the 180° similar to the “A” value measurement. Line perpendicular to the “A” value line would correspond to 90° and 270° as shown in Figure 1 (inside picture). Following these 2 lines, every quadrant would correspond to every 90°angular depth.
Results
Three-dimensional segmentation process of the complete inner ear from the clinical CT images took roughly 10 minutes depending on the number of image slices available. The resulting images provided the complete view of the inner ear in 3D in various planes.
Cochlear Parameters
From the 40 CT data sets, we identified 12 data sets with normal inner ear anatomy (NA) with a clear separation of a cochlear and vestibular part, 3 distinct semicircular canals, thin VA, and the IAC making a clear connection with the base of the cochlea. Four data sets with enlarged vestibular aqueduct syndrome (EVAS) were identified, which have the cochlear and the vestibular portion similar to the NA type in terms of the dimensions but the VA in the enlarged condition, as shown in Figure 2. In the EVAS condition, the VA in the axial plane is measured >1 mm. Due to the enlarged VA, it could pose the surgical complication of endolymphatic oozing when the cochlea is opened for electrode array placement. Eight data sets with only 2 turns of the cochlea (2TL) were identified. The 2TL looks similar to the NA type in terms of the “A” and the “B” values, but the cochlear lumen is only available for the basal and the middle turn of the cochlea. Seven data sets with IP type II were identified. Incomplete partition type II is also called as Mondini’s deformity that has the basal turn of the cochlea normally developed close to 1 full turn with the remaining portion of the cochlea in the form of a cyst. The “A” value is measured slightly shorter than the NA type cochlea. In most of the IP type II cases, VA is enlarged and this is clearly shown in Figure 2. Five data sets with cochlear hypoplasia (CH) were identified that represented the underdeveloped/not full formed cochleae with the “A” value usually shorter than the NA type cochlea. One data set with CC was identified that represents the combined cochlear and the vestibular portion into a single cavity. One of the surgical complications with the CC type malformation is the electrode entering the IAC and therefore an intraoperative imaging in controlling the proper placement of the electrode is advisable. Three data sets with abnormal IAC were identified.
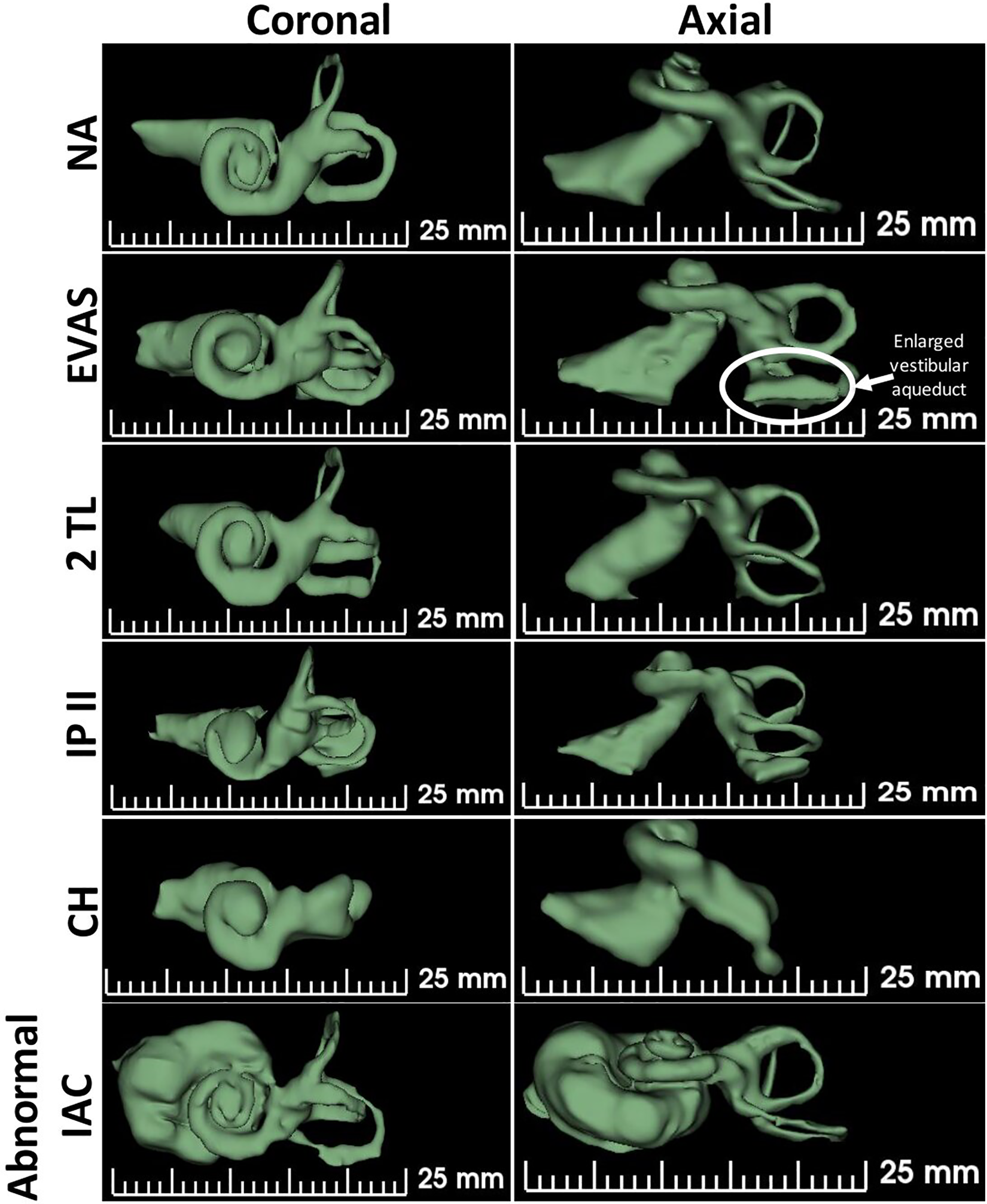
Inner ear with various anatomical types shown in 3 dimension in both coronal and axial plane.
Figure 2 shows sample images of the inner ear from each anatomical (pathological) type. Table 1 provides all the measurements of the inner ear made in this study. The measurements were made from both the ears, along with the patient’s age and the electrode array length implanted. Table 1 also shows the AID covered by the implanted electrode array. It is important to note that for the NA, EVAS, and 2TL anatomical types, in majority of the cases, either a 24 or a 28-mm long electrode has been implanted and as a result, the electrode array has gone as deep as 720° (Table 1, S. No: 22) at the most and 540° in majority of the cases. This shows that in these anatomical types, the cochlea is accessible for electrode array placement beyond the basal turn of the cochlea. For the cases S. No: 30 and S. No: 32 which are IP type II and CH, respectively, a 28-mm long electrode array has been implanted and that offered an AID of 700° and 540°, respectively. In none of the cases given in Table 1, the electrode array has not implanted shallower than the 360°.
Summary of All the Measurements of the Inner Ear With Different Anatomies.
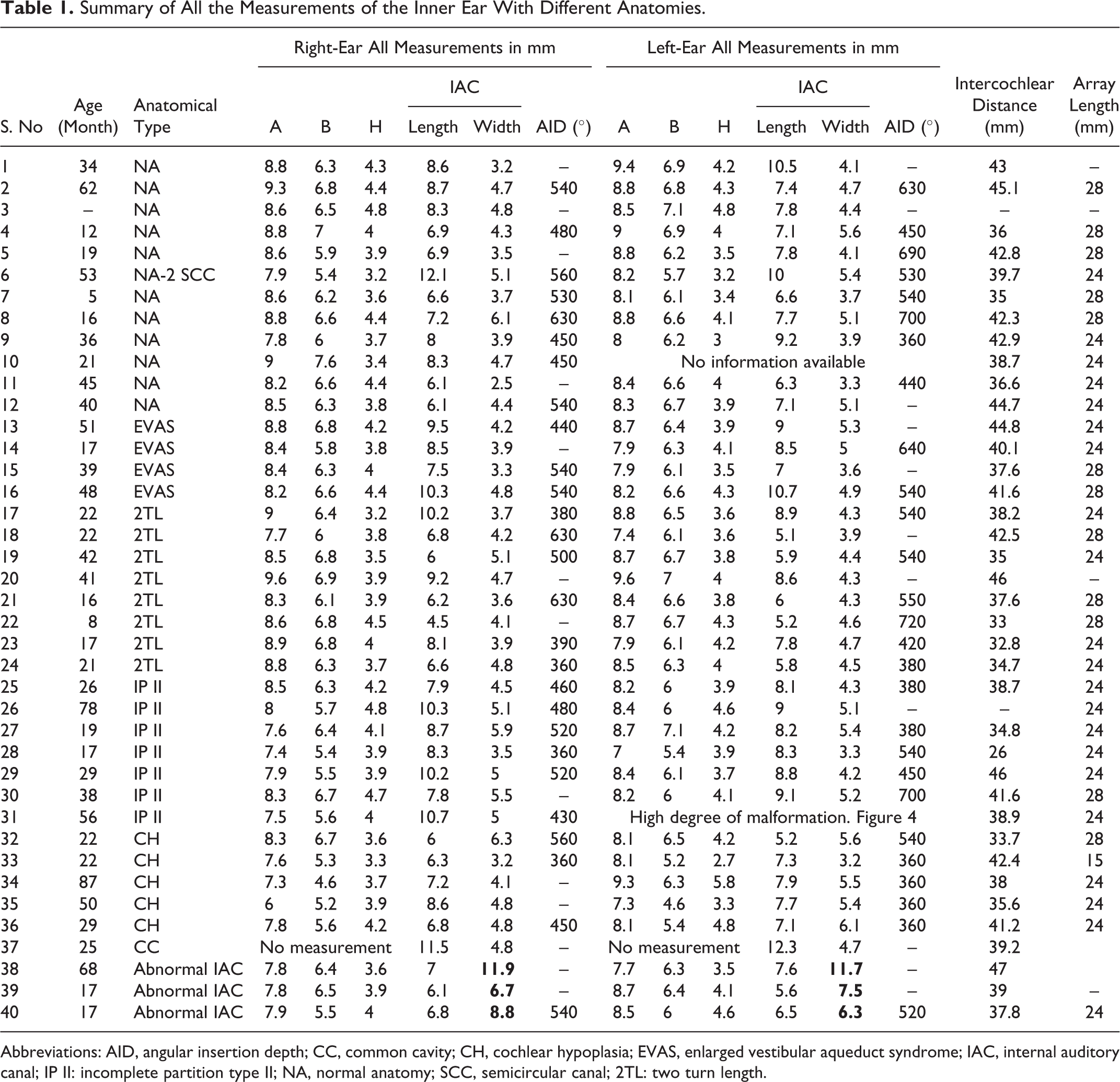
Abbreviations: AID, angular insertion depth; CC, common cavity; CH, cochlear hypoplasia; EVAS, enlarged vestibular aqueduct syndrome; IAC, internal auditory canal; IP II: incomplete partition type II; NA, normal anatomy; SCC, semicircular canal; 2TL: two turn length.
Age of the patients taken for the analysis in this study varied from 5 to 90 months. The “A” value ranged from a minimum of 6 mm to a maximum of 9.6 mm considering all the anatomical types. Age had no mathematical relation to the diameter of the basal turn “A” value measured across the malformation type and also between the right- and the left-side ear (Figure 3A). The “A” value and the “B” value had a positive linear correlation irrespective of the anatomical variation types with a very good regression value of more than 0.5 for the right ear and 0.45 for the left ear (Figure 3B). Cochlear height had no clear mathematical relation to the “A” value even though left-side ear showed a weak positive linear correlation (R 2 = 0.16) with the cochlear height (Figure 3C). Dimensions of the IAC were interesting to look at as the age of the patient had a positive logarithmic correlation (R 2 = 0.28) with the length of IAC for both sides of the ear (Figure 3D). Intercochlear distance had a positive logarithmic correlation (R 2 = 0.23) with the age of the patient (Figure 3E).
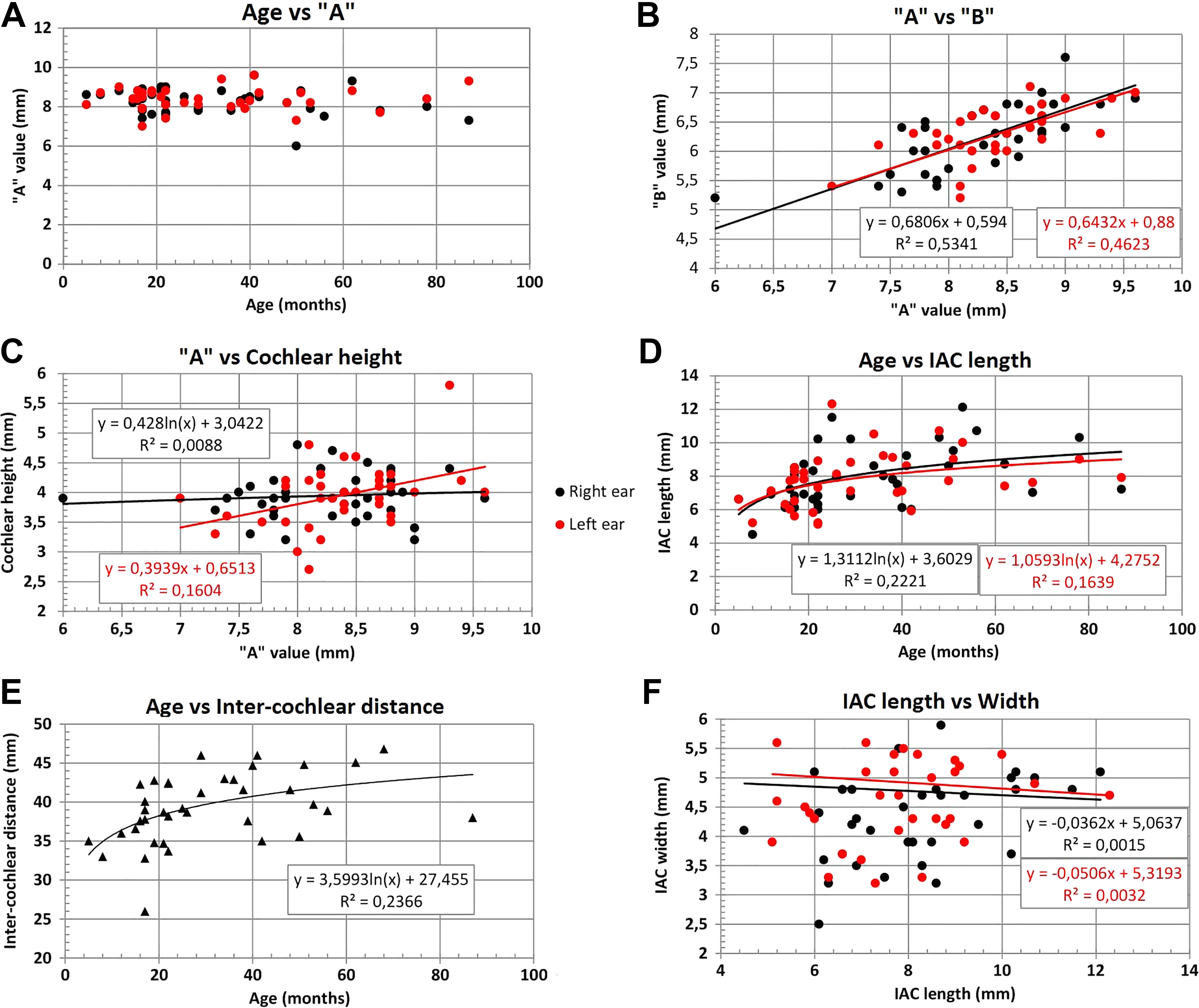
Six different x-y plots showing the mathematical relationships between different inner-ear dimensions. Age has no mathematical relation with the cochlear size measured by the “A” value (A). While cochlear diameter “A” and cochlear width “B” had a positive linear relation (B), there was no meaningful mathematical relationship seen between “A” and cochlear height (C). Age had a logarithmic relation with the length of IAC (D) and intercochlear distance (E). Length and width of IAC in the axial plane did not show any meaningful mathematical relation (F). IAC indicates internal auditory canal.
The length and the width of the IAC in the axial view had no meaningful mathematical correlation between them (Figure 3F). The AID of the electrode inserted did not show any mathematical relationship with the size of the cochlea. Within the normal cochlear anatomy, EVAS, and IP type II groups, the AID varied between 360° and 700°. With the 2TL group, the AID varied from a minimum of 360° to a maximum of 720°. For the CH group, the electrode AID showed a minimum of 360° to a maximum of 560°.
Observation on the Extreme Anatomical Variations
Figure 4 showing cases 31, 34, and 37 with different inner-ear malformation anatomies on either side of the ears. Case 31 showed IP type II on the right ear and almost cochlear aplasia on the left side. Case 34 had severe CH on the right side compared to the left side. As a result, CI electrode was only able to be placed on the left side, a 24-mm long array covering an AID of 360°. Case 37 is the most severe of all the cases as it showed cochlear aplasia on the right side and CC on the left side.
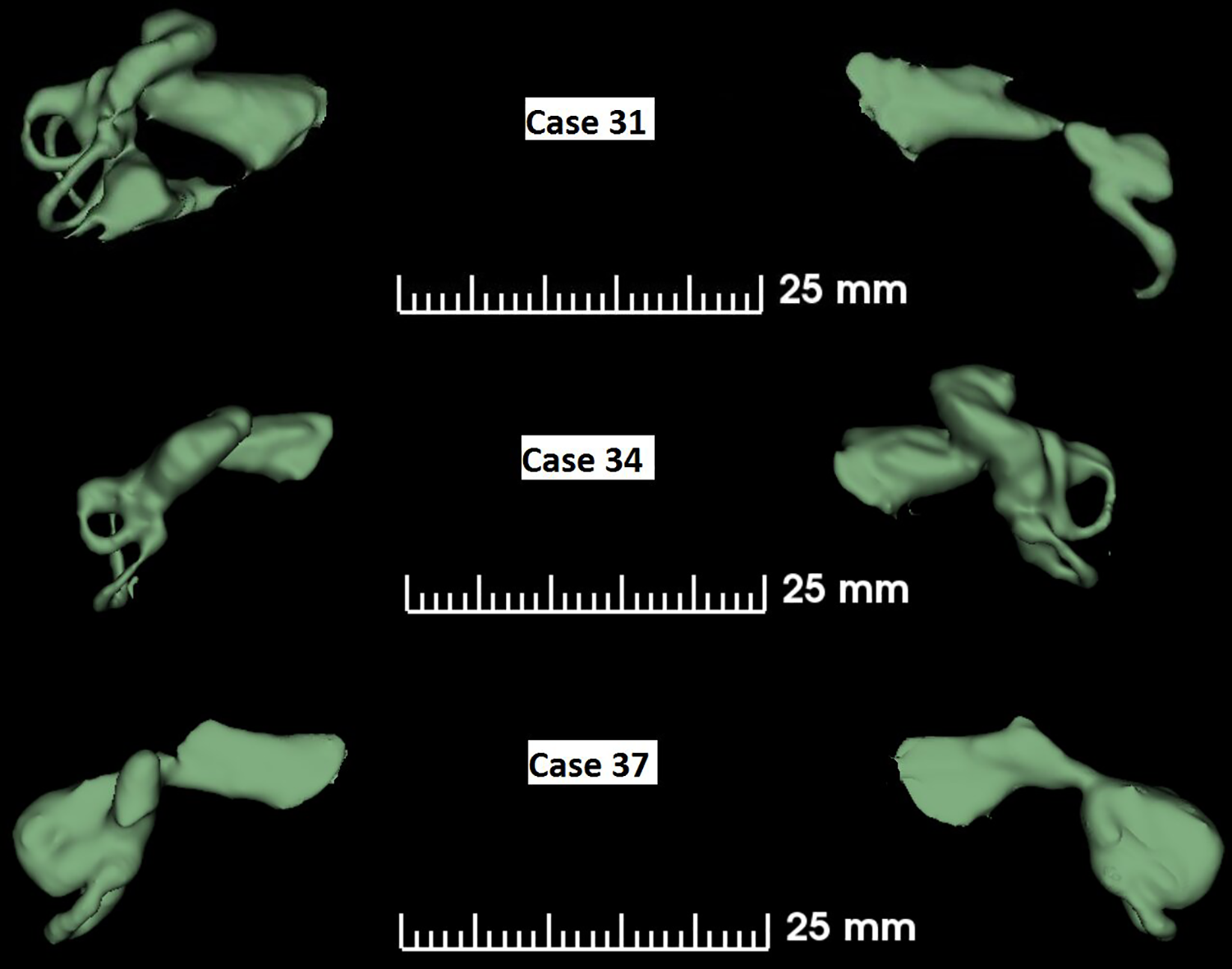
Three cases showing dissimilar inner-ear malformation types on either side of the ears.
Figure 5 captured 9 cases that had extreme anatomical differences in comparison to the normal anatomy inner ear. Case 6 showed a pretty normal anatomy cochlea but the vestibular portion lacked posterior semicircular canal on both sides as given in Figure 4. Both the ears implanted with a 28-mm long electrode array were shown to be fully placed inside the cochlea making an AID of more than 450°. Case 32 had CH-type malformation on both the sides and was implanted with a 28-mm long electrode that gave an AID of 560° and 540°, respectively, on the right and the left ears. Case 33 is another CH-type showing malformation in both the cochlear and the vestibular part. Both the ears had the electrode covering 360° AID, although the right side is implanted only partially with basal 4 channels placed extracochlear. Case 34 showed severe CH on the right side that would preclude CI as the cochlear portion is only developed half of the basal turn.
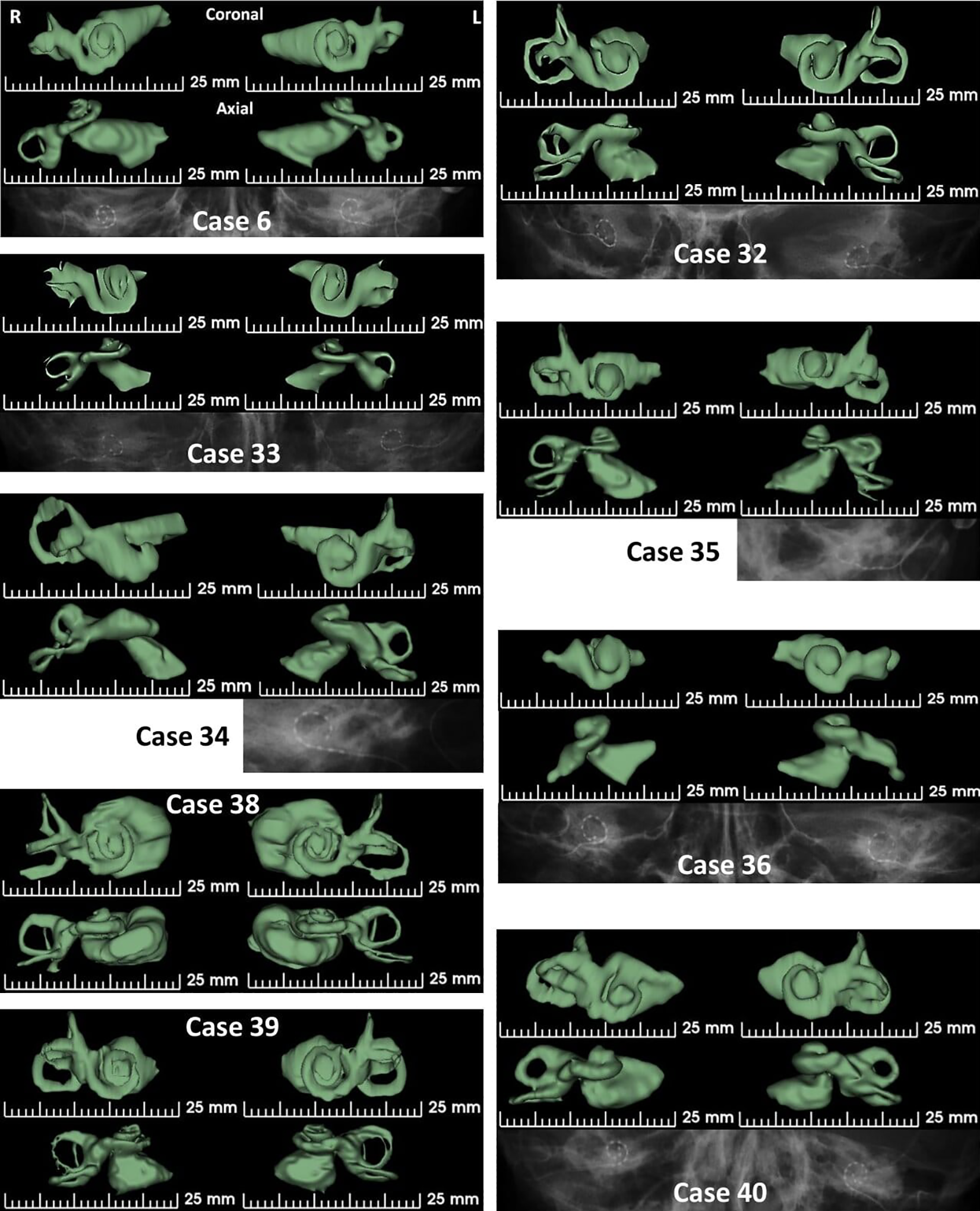
Case 6 showing the absence of the horizontal semicircular canal. Cases 32 to 36 has various degree of cochlear hypoplasia. Cases 38 to 40 shows much enlarged IAC in its width.
The left side, however, is developed to 1 full turn that allowed the electrode to cover an AID of 360°. Case 35 was again another severe CH-type malformation as the lumen of the basal turn of the cochlea is narrowing immediate to the cochlear entrance. Left ear showed partial insertion of the CI electrode covering an AID of 360° with basal 3 channels extracochlear. Case 36 was yet another CH-type malformation with the cochlear portion only developed for 360° of AID and the vestibular portion shows only the horizontal semicircular canal. The CI electrode provided a cochlear coverage of 360°. Cases 38, 39, and 40 show much enlarged IAC compared to any of the cases shown in this study. The width of IAC, in particular, is much enlarged (values bold in Table 1) in these 3 cases in comparison to all other cases taken in this study.
Discussions
Dhanasingh et al 15 recently showed the method of 3D segmentation in easy understanding of all the inner-ear malformation types. As more and more young surgeons are getting eligible to perform CI surgery, simple assistive tools like 3D segmentation could be handy. This current study applying 3D segmentation adds additional value especially in understanding the anatomical variations of the inner ear including the IAC which was not reported in the literature in detail.
This is yet another study confirming that cochlea reaches its full size at birth as the cochlear size measured by the “A” value did not have any mathematical relation with the age of the patient. The cochlear parameters “A” value and “B” value showed a positive linear relationship even for the cases with inner-ear malformation types which was never reported before. The interesting fact here is that even in cases with inner-ear malformation, there is a proportional growth between both “A” and “B” values of the basal turn. The cochlear height “H,” however, did not show any mathematical relation with the “A” value of the cochlea which is different to the earlier report of Liu et al 16 in which they showed shorter cochlear height for the CH group compared to IP type II and normal cochlear anatomy group. The length of the IAC seems to grow logarithmically with the age of the patient which is another novel finding in this study. The intercochlear distance as measured from end-to-end of the IAC in the axial plane showed a positive logarithmic growth with age of the patient. This finding is similar to the earlier report by Mori et al in 2011 17 confirming that the overall growth in the skull size has a positive linear effect on the intercochlear distance. Although we did not measure the mastoid thickness in this study, looking at the intercochlear distance growing logarithmically with age, it can be assumed that the mastoid thickness will also grow logarithmically. This could have an effect on the excess electrode lead over time which is looped in the mastoid cavity.
In our study, we identified 3 cases (38-40) that showed ginormous IAC especially in its width as measured in the axial plane, which was not reported so far in the CI field. Since all these cases taken for the analysis in this study did have meaningful benefit from the CI, the distinct effect of ginormous IAC on postoperative CI hearing is not clear. The electrode AID coverage showed that even in the cases of CH, if the cochlea is available for 1 full turn, then it is possible to place the electrode for at least 360°. Not to forget that if the degree of malformation is too severe as seen in case 35, it might be challenging to push the electrode fully inside the cochlea.
This study had the limitation of smaller sample size of only 40 CT data sets that included very few numbers within each malformation types. The IAC showed a great variation in its dimensions and the future work could use the 3D segmentation of the inner ear and study the effect of IAC volume to the hearing performance of CI patients. This was never studied before and any research in that direction could shed light to the importance of size of IAC in predicting hearing with CI.
Conclusion
To best of our knowledge, this was the first study coming from the Middle-East region investigating the diagnostic value of 3D segmentation of the inner ear in the malformation types and as well in understanding the general anatomical variations of the inner ear. Young surgeons who are coming into the CI field with little or no experience handling the inner-ear malformation cases could benefit from this 3D segmentation method. Knowing the inner-ear dimensions and how it varies with the various malformation types could be valuable information before going for the CI surgery. Three-dimensional segmentation of the inner ear should become a routine in the preoperative CT scan analysis in all the difficult anatomical cases.
Footnotes
Acknowledgements
Authors thank Yassin Samad, PhD for his overall support during this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Anandhan Dhanasingh is employed by MED-EL as the Head of CI Electrodes Research which is purely a scientific role and this study did not contain any marketing message.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.