
Abstract
Keywords
Introduction
The nose is not only involved in functions such as breathing and smelling but is also crucial for the appearance of the whole face, that is, for facial aesthetics, as it is the centermost feature of the face. Thus, nasal traumas can affect individuals’ quality of life in functional or aesthetic terms. As the nasal bone is the most protruding part of the face, nasal bone fractures (NBFs) are pretty common and even the most common form of maxillofacial fractures. 1 The management, treatment, and etiology of NBFs have been widely studied. The most common causes include interpersonal violence, traffic accidents, sports injuries, and falls. 2
A detailed look at the etiology of NBFs may raise the question of whether there are differences in the psychiatric evaluation of patients based on the cause of trauma. Assessing these patients for the presence of personality disorders, impulsivity, or attention-deficit/hyperactivity disorder (ADHD) may reveal exciting results. For instance, a case of NBF caused by violent incidents may be associated with several psychopathologies that underlie aggressive personality traits.
Impulsivity may be seen in individuals with or without personality disorders and is associated with various psychiatric disorders, such as psychopathy, antisocial behavior, and violence.3,4 ADHD is the most common psychiatric disorder in children, and since it persists into adulthood, it is also a common adult psychiatric disorder. 5 Most researchers have argued that impulsivity is associated with ADHD. 6
This study aimed to assess patients presenting with NBFs not only for nasal trauma but also for personality disorders, impulsivity, and ADHD using psychiatric questionnaires.
Materials and Methods
The study was conducted at a local training and research hospital between April 2022 and October 2022. The study received ethics committee approval from the local university (dated April 06, 2022, no. 50413). The study included a total of 41 patients over the age of 18 years (mean age 26.39 ± 8.19 years), of whom 5 were female and 36 were male, presented to the otorhinolaryngology outpatient clinic or emergency department of Mardin Training and Research Hospital. It was radiologically diagnosed with NBF after acute trauma. After obtaining informed consent from the patients, the researchers proceeded with history-taking, physical examination, and administration of psychiatric questionnaires on the subjects. An ENT physician then treated the patients for NBF.
The CG consisted of 43 volunteers without NBF aged 30 to 40 years (mean age 33.00 ± 3.61 years), of whom 23 were female. Neither the patients nor the volunteers had previously been diagnosed with or treated for psychiatric disorders. After providing informed consent, the subjects in the CG received the same psychiatric questionnaires administered to the study group. The psychiatric questionnaires administered were the Eysenck Personality Questionnaire Revised—Short Form (EPQR-S), Barratt Impulsivity Scale—Short Form (BIS-11-SF), and Turgay’s Adult ADD/ADHD DSM-IV-based Scale. The study assessed patients in 2 groups, the NBF group, and the CG, and sought to reveal differences between them.
Inclusion Criteria
The NBF group included patients over 18 years of age who were presented to the ENT outpatient clinic or emergency department for NBF caused by acute trauma within the last week, who were radiologically diagnosed with nasal fracture, and who volunteered to participate in the study.
The CG included volunteers aged 30 to 40 years with no NBF.
Exclusion Criteria
Patients were excluded from the nasal fracture group if they had a nasal fracture for more than 1 week, had no radiologically-confirmed diagnosis of nasal fracture, were under 18 years of age, or refused to participate in the study.
Both the control and patient groups excluded individuals who had previously been diagnosed with or treated for a psychiatric illness.
Data Collection Instruments—Psychiatric Questionnaires
Barratt Impulsivity Scale—Short Form
Impulsivity is a broad concept that can be associated with numerous psychiatric disorders. Several scales have been developed to assess impulsivity, including BIS-11-SF. 7 The BIS-11-SF is a 15-item impulsivity assessment questionnaire used in many clinical studies for its ease of administration. Its reliability has been compared with its Turkish version. BIS-11-SF is in the form of a four-point Likert scale and divided into 3 subscales: nonplanning (NP), motor impulsivity (MI), and attention impulsivity (AI), all with good reliability. Higher ratings on the scale indicate higher impulsivity. The study, which demonstrates that the internal validity of the Turkish-adapted BIS-11-SF was assessed through a comprehensive factor analysis to ensure consistency with the original test, shows that the Turkish version maintains the scope of the original test. 8 Overall, this adaptation study indicates that the Turkish-translated BIS-11-SF has been validated and has passed a thorough psychometric evaluation.
Turgay’s Adult ADD/ADHD DSM IV-Based Diagnostic Screening and Rating Scale
ADHD is the most common neuropsychiatric disorder in children, and as it persists into adulthood, adult ADHD is also ubiquitous. Adult ADHD has been included in the DSM-IV as a disruptive behavior disorder. 9 The ADD/ADHD scale developed by Şennur et al. 10 based on DSM-IV has been validated for use in the Turkish population and thus used in our study. 10 According to this study, the Turkish version meticulously-addressed linguistic equivalence, aiming to prevent meaning loss during the translation process and demonstrated that it preserved the content of the test. Overall, this adaptation study has ensured the validity and reliability of the Turkish-translated Adult ADHD Scale and has shown that it has undergone a thorough psychometric evaluation. 10 The test is a 5-point Likert scale composed of 3 subscales: attention deficit (ADS, 9 items), hyperactivity impulsivity (HS, 9 items), and ADHD-related characteristics and problems subscale (ADHD-PS, 30 items). In the first 2 parts of the test, the outcome is either “present” or “absent” AD (attention deficit) or H (hyperactivity), while the third part yields a total ADD/ADHD score.
Eysenck Personality Questionnaire Revised—Short Form (EPQR-S)
The Eysenck Personality Questionnaire is a widely-used instrument for assessing personality and originally has well-defined psychometric properties, providing high validity and reliability results and has been tested with a broad cultural sample. 11 The modified short form of the questionnaire used in our study has been previously validated for use in the Turkish population. 12 The Turkish adaptation, on the other hand, was adapted to ensure its validity and reliability within the cultural and linguistic contexts. Overall, the Turkish adaptation of the test has preserved the psychometric properties of the original test, demonstrating its validity and reliability in Turkey and undergoing a detailed psychometric evaluation. This indicates that the test can be effectively used in both academic and clinical contexts. This questionnaire has 24 items and assesses personality under 3 main factors: extraversion, neuroticism, and psychoticism. Each factor comprises 6 items and is answered with YES (1) or NO (0).
Statistical Analysis
The research data were statistically analyzed using the SPSS version 21.0 statistical software (IBM, Armonk, NY, USA) suite for Windows. Numerical variables were presented in mean ± standard deviation and median values, while categorical variables were presented in number and percentage (%). The data were checked for normality of distribution, and the groups that did not fit in the standard distribution were compared using the Mann–Whitney U test. Qualitative variables were compared between groups using the chi-squared (χ2) test. Statistical significance was set at P < .05.
Results
The study’s patients were divided into 2 groups. Out of 84 patients, 41 were in the NBF group, and 43 were in the control group (CG). In the NBF group, 5 were female (12.20%) and 36 were male (87.80%). In the CG, 23 were female (53.49%) and 20 were male (46.51%) (Table 1).
Breakdown of Age and Sex of the Subjects in the Groups.
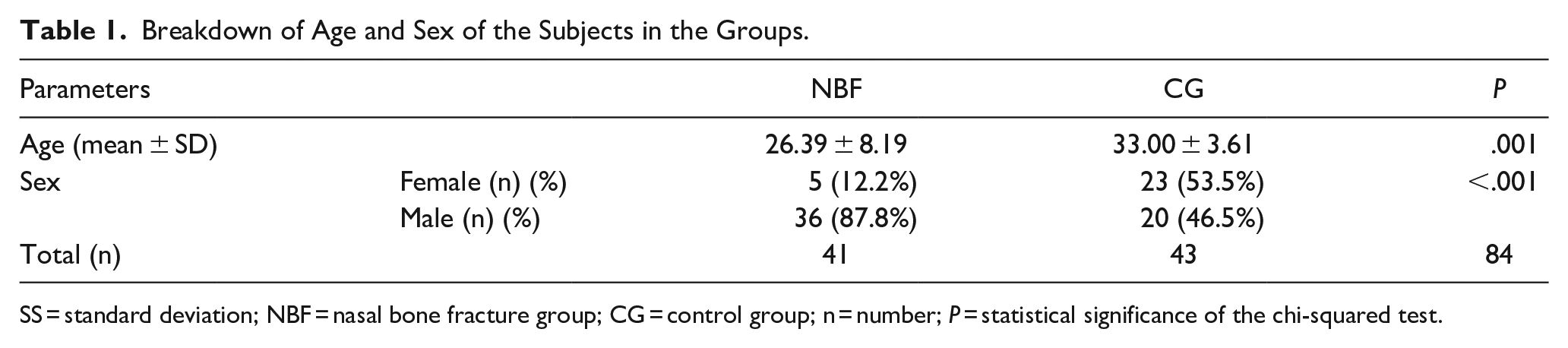
SS = standard deviation; NBF = nasal bone fracture group; CG = control group; n = number; P = statistical significance of the chi-squared test.
The most common cause of NBFs in our study was violence (41.5%), followed by traffic accidents (29.3%), falls (17%), and sports injuries (12.2%).
In the EPQR-S assessment, the NBF group had significantly-higher total scores than the CG (P < .001). In the subscales of the questionnaire, extroversion, psychoticism, and lie subscale scores were higher in the NBF group than in the CG. In the neuroticism scale, however, there was no statistically-significant difference between the NBF group and the CG (Table 2).
Comparison Between the Patients and the Control Group in Terms of Total Scores and Subscale Scores on EPQR-S.
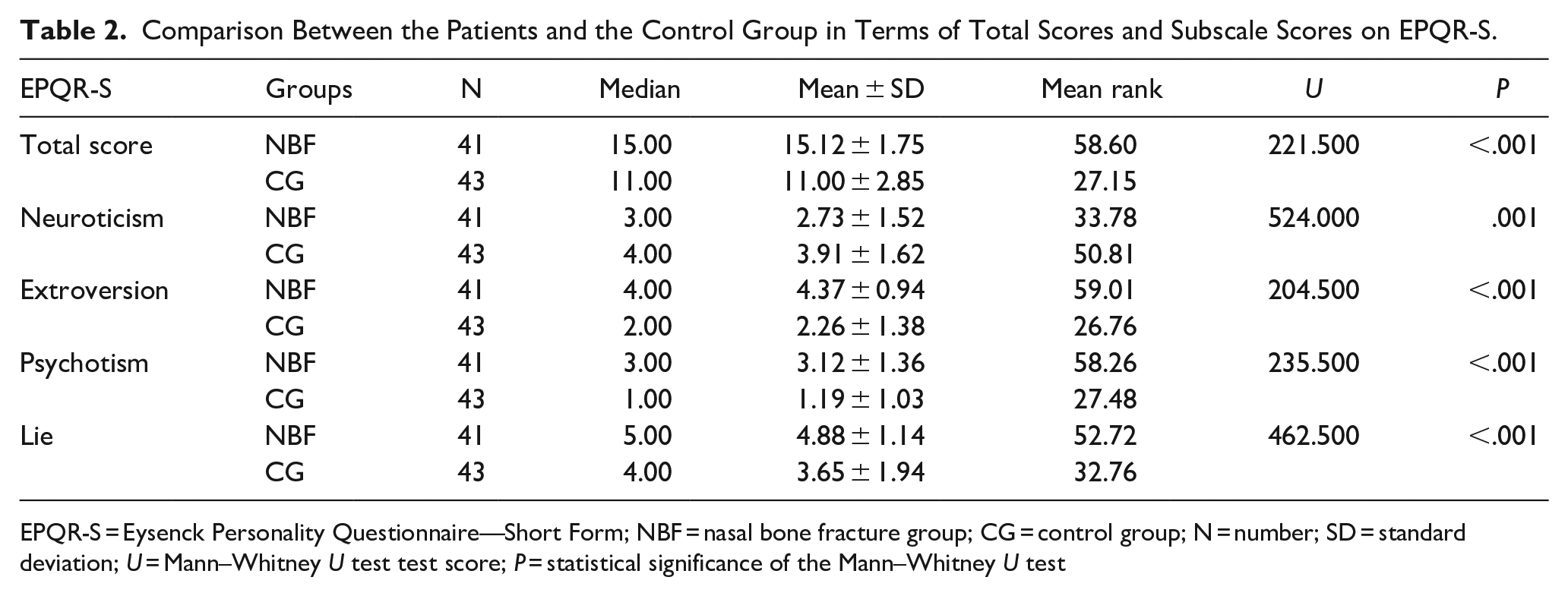
EPQR-S = Eysenck Personality Questionnaire—Short Form; NBF = nasal bone fracture group; CG = control group; N = number; SD = standard deviation; U = Mann–Whitney U test test score; P = statistical significance of the Mann–Whitney U test
In the BIS-11-SF assessment, the NBF group had higher total scores than the CG (P < .001). Comparison by subscales revealed that the NBF group had high scores in all the subscales (Table 3).
Comparison Between the Patients and the Control Group in Terms of BIS-11-SF Total Scores and Subscale Scores.
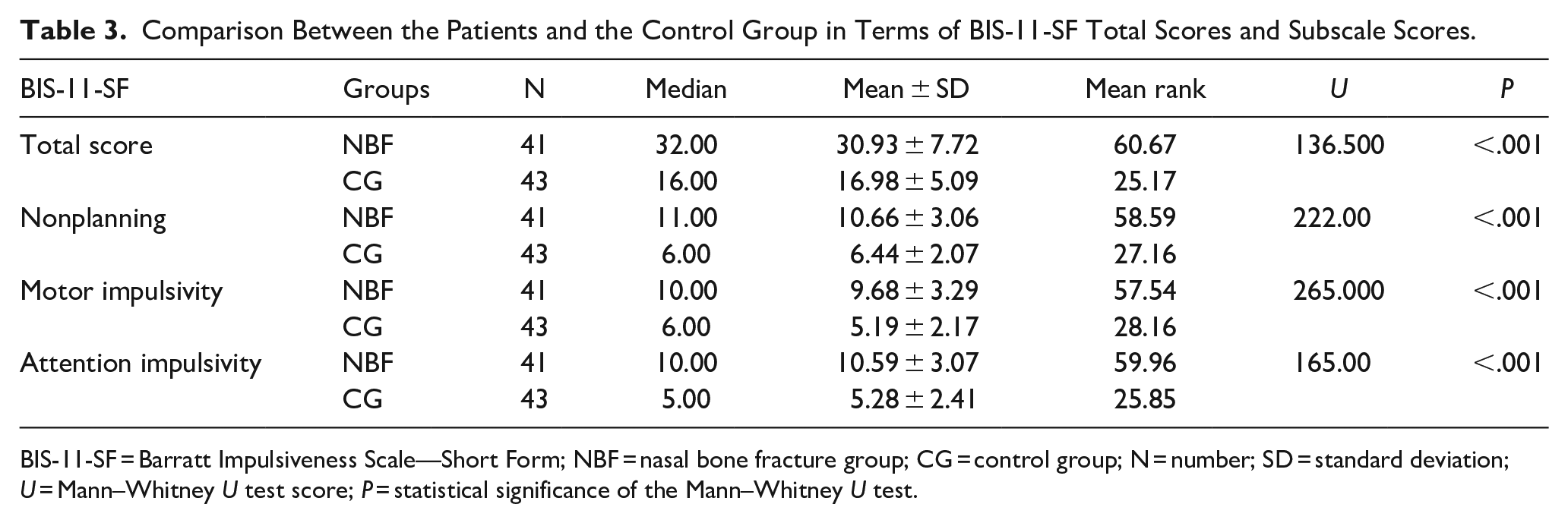
BIS-11-SF = Barratt Impulsiveness Scale—Short Form; NBF = nasal bone fracture group; CG = control group; N = number; SD = standard deviation; U = Mann–Whitney U test score; P = statistical significance of the Mann–Whitney U test.
Assessment using Turgay’s adult ADD/ADHD DSM IV-based diagnostic screening and rating scale revealed no statistically-significant difference between the NBF group and the CG in terms of AD and H (Table 4).
Comparison Between the Patients and the Control Group in Terms of AD and H.
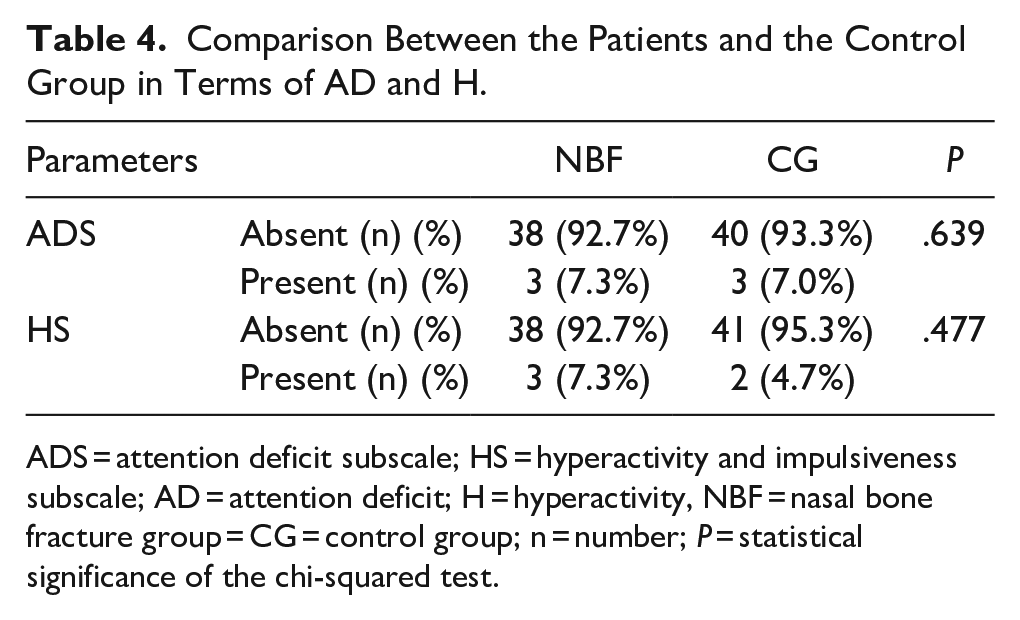
ADS = attention deficit subscale; HS = hyperactivity and impulsiveness subscale; AD = attention deficit; H = hyperactivity, NBF = nasal bone fracture group = CG = control group; n = number; P = statistical significance of the chi-squared test.
In the ADD/ADHD test, the problems subscale (PS) assessment revealed no statistically-significant difference between the NBF and CG (Table 5). In neither group were the total test scores high enough to establish an ADD/ADHD diagnosis.
Comparison Between the Patients and the Control Group in Terms of ADS/ADHD-PS.

ADD/ADHD = attention deficit disorder/attention-deficit/ hyperactivity disorder; PS = problems subscale; NBF = nasal bone fracture group; CG = control group; N = number; SD = standard deviation; U = Mann–Whitney U test value; P = statistical significance of the Mann–Whitney U test.
Discussion
Nasal fractures are a typical ENT emergency and the most common form of maxillofacial fractures. 1 The etiology of NBFs was investigated by Juncar et al. 13 in a 10-year study of 280 patients with NBFs; nasal fractures were primarily seen in young, uneducated males, with the most common cause as interpersonal violence and aggression (43.24%). The second common cause of nasal fractures was traffic accidents, and the third was due to falling. In a review of 26 articles, Hwang et al. 2 reported that the most common cause of NBF in adults was fought (36.3%), followed by traffic accidents (20.8%), sports injuries (15.3%), and falls (13.4%).
The predominance of interpersonal violence in the etiology of NBFs raises the question of whether individuals presenting with NBFs are prone to violence. Hoffman et al. 14 evaluated psychiatric disorders in patients with facial trauma admitted to the emergency department without a previous diagnosis of psychiatric illness and found that a subgroup of facially-injured patients had several personality disorders such as mood disorders, substance or alcohol abuse, schizophrenia; and borderline, antisocial, or narcissistic personality disorders. The researchers concluded that this issue warranted further studies. The researchers underlined that, in their opinion, their study underestimated the true prevalence of mental illness in victims of facial injury. The fact that NBFs are the most common type of maxillofacial fractures and are caused mainly by violence has prompted us to evaluate the patient group psychiatrically.
Our study started with the administration of the EPQR-S on the subjects. This questionnaire assesses personality using 24 items divided into 3 factors: extraversion, neuroticism, and psychoticism. It also includes a lie subscale intended to prevent bias in test administration and to check for internal validity. 12 Extraversion represents sociability and impulsivity, and individuals with high scores in this dimension are defined as being keener to communicate and interact with others. Higher extroversion scores mean increased tendency to exhibit impulsivity, uncontrolled emotions, and irrational behavior. Neuroticism indicates emotional instability and reactiveness, and individuals who score high on this dimension tend to be anxious, depressive, overly emotional, shy and have low self-esteem. The psychoticism dimension highlights personality characteristics such as being distant, cold, aggressive, insensitive, and unable to empathize with others. People with high psychoticism scores are defined as being aggressive, distant, and having an antisocial behavior pattern.11,12 The EPQR-S assessment in our study revealed a statistically-significant difference between the NBF group and the CG in extroversion, psychoticism, lie subscales, and total scores. On the other hand, assessment on the neuroticism subscale revealed no significant difference between the 2 groups. When compared to the normative values on the EPQR-S for the Turkish population, the psychoticism score was found to be higher than the normative mean values. Our study revealed that the NBFs mainly were caused by violence, with also significantly-high psychoticism scores on the personality questionnaire; this supports our hypothesis that aggressive and antisocial personality patterns are likely to be more common in patients presenting with NBFs. Johnson’s study to evaluate aggressive personalities reported that violent individuals are associated with a higher prevalence of antisocial personality disorder, narcissistic personality disorder, borderline personality disorder, and schizoid personality disorder. 15 This study also suggests that early intervention may reduce the repercussions associated with antisocial behavior.
Impulsivity is common in individuals who are prone to violence, and impulsivity and antisocial personality disorder may be associated with one another. The BIS-11-SF, administered to the subjects in our study, is a 15-item, 3-factor self-report scale that measures impulsivity.7,8 It has 3 subscales: NP, MI, and AI. Individuals with MI, in particular, tend to be violent. In a study that included inmates, Chen et al. 16 found that the group with antisocial personality had higher impulsivity and emphasized that detecting MI may contribute to preventing violent incidents.
BIS-11-SF assessment in our study revealed a significant difference between the NBF group and the CG in terms of total and subscale scores. In particular, there was a substantial difference between the 2 groups in MI scores, which supports our hypothesis that patients presenting with NBFs may be prone to violence.
ADHD is associated with an increased incidence of accidental injury due to attention deficit or hyperactivity. Also, 75% of patients with ADHD have been reported to have comorbid psychopathological conditions (such as anxiety disorders, alcohol abuse, antisocial personality disorder, dysthymic disorder, or major depression). 9 Considering both perspectives, we thought that patients presenting with NBFs may have an increased risk of accidental injury or a violent tendency, that is, they may have a high ADHD prevalence. Assessing increased risks in individuals with ADHD may contribute to preventing injuries.16,17 For all these reasons, the subjects in our study were also evaluated using Turgay’s Adult ADD/ADHD DSM IV-based Diagnostic Screening and Rating Scale. This scale is divided into 3 subscales: The first assesses attention deficit (ADS), the second assesses hyperactivity and impulsivity (HS), and the third assesses ADHD-related problems. 9
Prasad et al reported that the risk of fracture is 25% higher in individuals with ADHD than in individuals with other neurobehavioral disorders. 17 This may be due to an increased risk of accidental injury caused by lack of attention or hyperactivity. Our study, however, found no significant difference between the NBF group and the CG in terms of ADS, HS, or PS. We think this may be because our study included fewer patients in whom NBF was caused by falls and sports injuries.
In our study, the age distribution was not homogeneous between the patient and CG.
Altough this is one of the limitations of the study, Johnson 15 explores the persistence of antisocial and psychopathic traits, noting that while the expression of these traits may evolve, they often remain evident throughout life. Antisocial personality disorder and psychopathy, which are closely related to impulsivity and psychotic traits, are frequently diagnosed in younger populations but can continue to influence behavior in later stages of life. 15 Furthermore, Chen et al. 16 highlight that childhood experiences, such as emotional abuse, can exacerbate impulsivity and psychotic traits. This study focuses on male violent inmates with antisocial personality disorder, demonstrating that early-adverse experiences can lead to heightened impulsivity and a tendency toward violent behavior, which may persist into adulthood. 16 Longitudinal studies schow that while the peak of these traits is often during adolescence, they can continue into later adulthood, albeit with some reduction in intensity. This persistence might be attributed to the enduring nature of personality traits and the ongoing influence of life experiences and neurobiological factors.11,16 While impulsivity and psychotic traits may become less pronounced or manifest differently as individuals age, the underlying predispositions can persist, influencing behavior and personality throughout the lifespan.
Research indicates that ASPD and psychopathy are more frequently diagnosed in men explains that men are generally more likely to exhibit aggressive and antisocial behaviors associated with these disorders. 15 Chen et al. 16 examined the relationship between childhood emotional abuse and MI, finding that this impulsivity is more pronounced in male violent offenders. While men are inclined toward physical impulsive actions, women may exhibit impulsivity through less overt behaviors, such as emotional outbursts or risky decision-making. 16 Prasad et al. 17 found that boys with ADHD have a higher risk of injury than their non-ADHD peers. In summary, gender differences play a significant role in disorders such as ASPD, psychopathy, impulsivity, and ADHD. Men are generally more affected by aggressive behaviors and physical impulsivity, which can make them more susceptible to injuries such as nasal fractures. Understanding the relationship between psychological disorders and physical injuries helps clarify how these conditions are related to gender and etiological factors. In our study, however, there is a nonhomogeneous gender distribution between the patient and CGs, and due to this, statistical assessment based on gender differences could not be performed.
Conclusions
This study aimed to assess psychopathological symptoms in patients presenting with NBF. We found that psychoticism patterns and impulsivity were more prevalent in the patient group, whereas ADD/ADHD was not. The results of our study suggest that performing a psychiatric assessment may be the right decision in patients presenting with NBFs caused by violence, whether they are the aggressor or the victim. An early intervention can contribute to reducing problems and repercussions caused by disruptive behaviors of antisocial individuals. In addition to violent incidents, further studies are recommended, which include a large number of patients with fractures caused by traffic accidents, falls, and sports injuries. Such studies can allow for examining patients by cause of trauma and customized psychiatric evaluation based on the presence of psychiatric comorbidities that may have contributed to the pattern of injury. This study is the first to investigate psychiatric comorbidities in patients presenting with NBF and can thus contribute to the literature on this subject.
Limitations of the Study
The presence of a significant age difference between the patient and CGs, the nonhomogeneous distribution of gender in the groups, and the sample size not being sufficiently large may affect the results and constitute the limitations of this study.
Footnotes
Correction (December 2024):
In the published version of the article, an error was noted in the second author’s name “M. Mahir Akbudak” which has been corrected to “Mahir Akbudak”. The article has been updated online to reflect this change and a correction notice has been published to indicate this change. The correction notice is available here: 10.1177/01455613241309462
Authors Contributions
All authors contributed to the conception, design and planning of the study, collection, and/or assembly of data, data analysis, and interpretation, writing, and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The study was approved by the Ethics Committee of Mardin Artuklu University (document date and number: 13/05/2022-53581) and conducted by the principles of the Declaration of Helsinki.
Informed Consent
Consent was obtained from each patient who agreed to participate in the study. Written and verbal information about the survey was given to the participants. The patients were informed they could withdraw from the study at any stage.