
Abstract
Introduction
Nasal deformities have a large spectrum, from minor esthetic concerns to major deformities with severe esthetic and breathing problems in combination.1-4 Due to their complex deformity, Crooked noses present significant challenges for rhinoplasty surgeons. The upper third, the bony vault, is the most difficult part of the crooked noses. 4 Correcting a crooked nose is to reset the angle formed by the nasion–rhinion line at the midline to zero. 4 In crooked noses, the lengths of the right and left nasal bones differ, typically with the nasal bone on the side of the deviation being shorter (Figure 1A and B). Traditional correction methods have focused on osteotomies but have not extensively addressed the equalization of bone length due to the lack of appropriate instruments. 4 Advances in technology have led to the development of powered instruments, including piezoelectric devices (PDs), powered microsaws (PMSs), and otological drills (OD). 5 This study aims to correct crooked noses using a novel technique involving OD and ostectomy to shorten the longer nasal bone, thus equalizing the length of both nasal bones and resetting the nasion–rhinion line at the midline for optimal esthetic results.
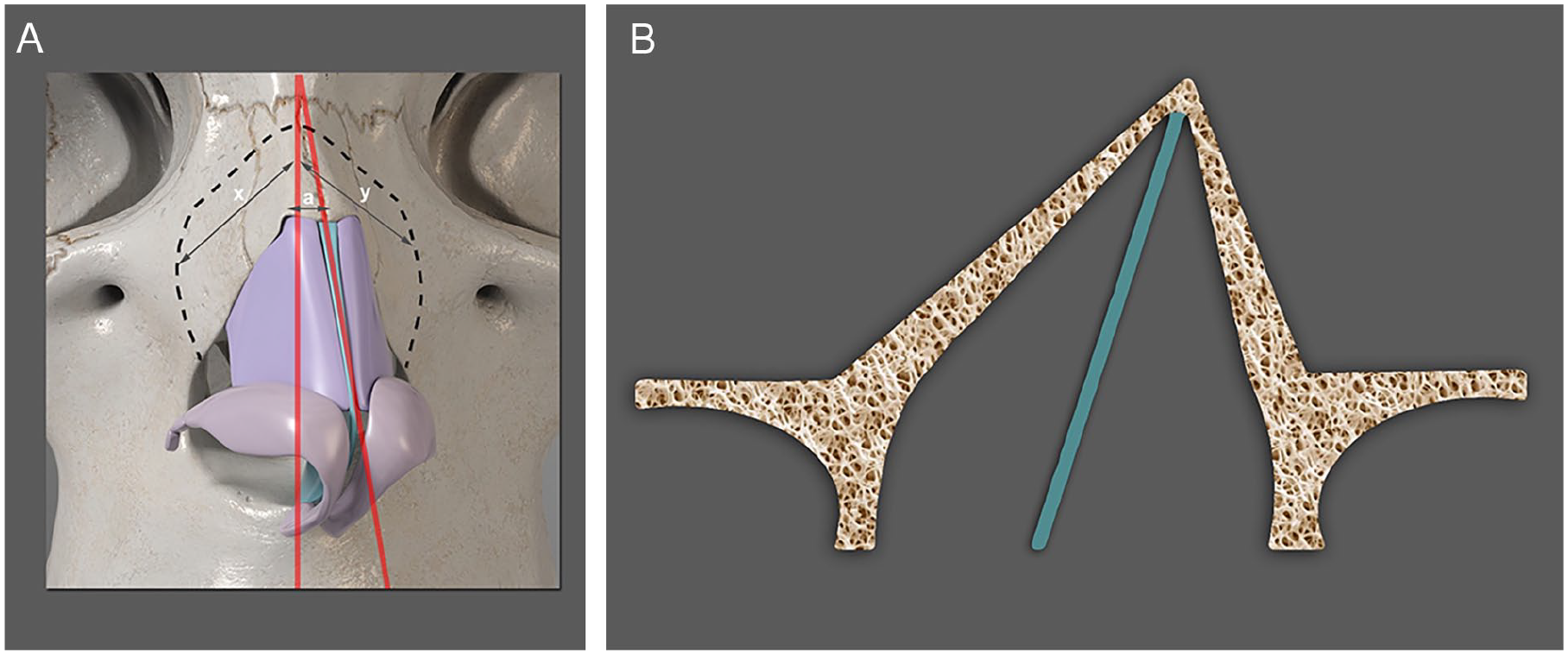
(A) Basal view that illustrates the anatomical structure of the nose with a deviation to the left. The red lines represent the intended midline and the existing midline. The differences in length on both sides are indicated by x and y. (B) Basal view diagram illustrating a crooked nose with deviation from the left axis.
Materials and Methods
This study strictly followed the principles outlined in the Declaration of Helsinki. Ethical approval was obtained for the study (Health Sciences University Tepecik Research and Training Hospital Date: June 6, 2023 Decision Number: 2023/05-16).
Under general anesthesia, 4 ml of infiltration anesthesia (20 mg/ml lidocaine hydrochloride + 0.0125 mg/ml epinephrine) was administered. A Goodman’s incision was made, and the skin flap was elevated to the nasion. An extended skin elevation was performed on both sides to a 0.5 cm lateral point to the ascending process of the maxillary bone. A sharp dissection was carried out between the lower lateral cartilages’ medial crus to reach the septum’s caudal end. Mucoperichondrial elevation was performed on both sides of the septum. A low strip of cartilage was removed from the septal cartilage to free it from the base, and the deviated parts of the septum were excised. The caudal septum was separated from the nasal spine. In cases requiring removal of the dorsal hump, a 3-mm diamond drill operating at 15,000 rpm was used to splinter the bony dorsum.
The distance between the nasofacial groove and the midline of the nasal dorsum on both sides was measured with a ruler. Lateral and transverse ostectomies were performed on both sides with OD. The drill size for the lateral ostectomy on the opposite side of the curvature was determined by adding 1 mm to the estimated difference, formulated as follows: (x − y) + 1. The drill’s size for transverse osteotomy was determined by measuring the distance between an imaginary line from the nasion to the lip philtrum and the actual line from the nasion to the rhinion named as in the figure. We used 1 mm drills for both transverse and lateral ostectomies on the side of the deviation, taking great care to preserve the inner nasal mucosa.
Root osteotomy was performed percutaneously in the nasion area, with a 2-mm osteotome acting as a hinge (Figure 2A and B). The nasal dorsum was reduced by approximately 1 mm with this maneuver. Manual force was applied from the deviated side, causing en bloc movement of the nasal bony vault toward the midline. As a result of the reduction in dorsum projection of 1 mm and medialization of the nasal bony vault, a scab was performed using a 3-mm diamond tip to prevent step formation in the frontal process of the nose on the deviated side (Figure 3A and B). Subsequently, appropriate cartilage grafts, flap techniques, and sutures were applied to the middle and lower thirds of the nasal dorsum. The septum cartilage at the caudal end was resutured to the spine with 5/0 Prolene in a figure of 8. For double checking, the length of both nasal bones was measured and the nasion–rhinion line was reset at the midline for optimal esthetic results. Transeptal sutures (4/0 Vicryl sutures) and 18 Gage cannulas were placed bilaterally under the skin on the transverse ostectomy line to ensure drainage. Finally, internal nasal packing and external molds were applied.
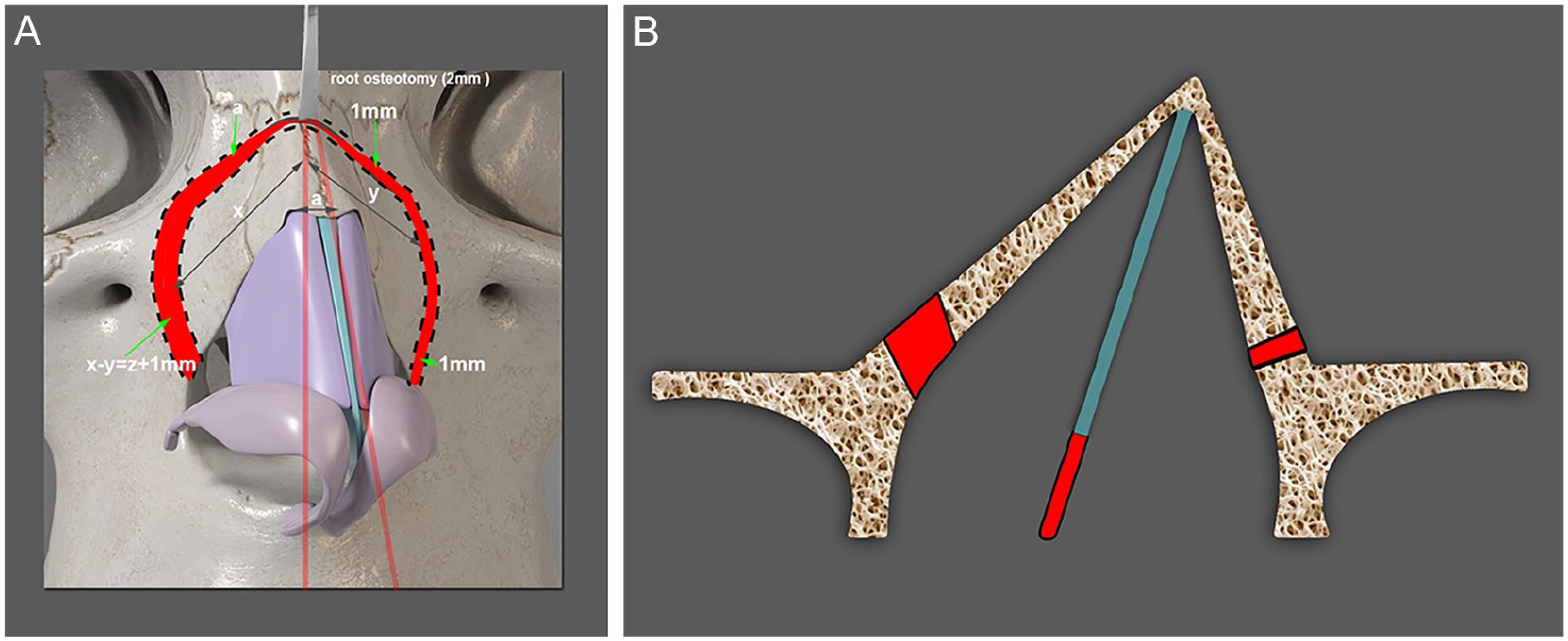
(A) Frontal view illustrating the anatomical structure of the nose with the distance between the nasofacial groove and the midline of the nasal dorsum on the right side represented as (x), the distance from the nasofacial groove to the midline of the nasal dorsum on the left side represented as (y) and the distance between an imaginary line from the nasion to the lip philtrum and the actual line from the nasion to the rhinion (a). Areas of ostectomies are marked in red and delineated by dotted lines. Root osteotomy in the nasion using a 2-mm percutaneous osteotome. (B) Basal view that illustrates the anatomical structure of the nose with the ostectomy areas marked in red on the long and short sides of the nasal pyramid. The blue line represents the septum. The red line in the septum indicates the excision of the low-strip septal cartilage.
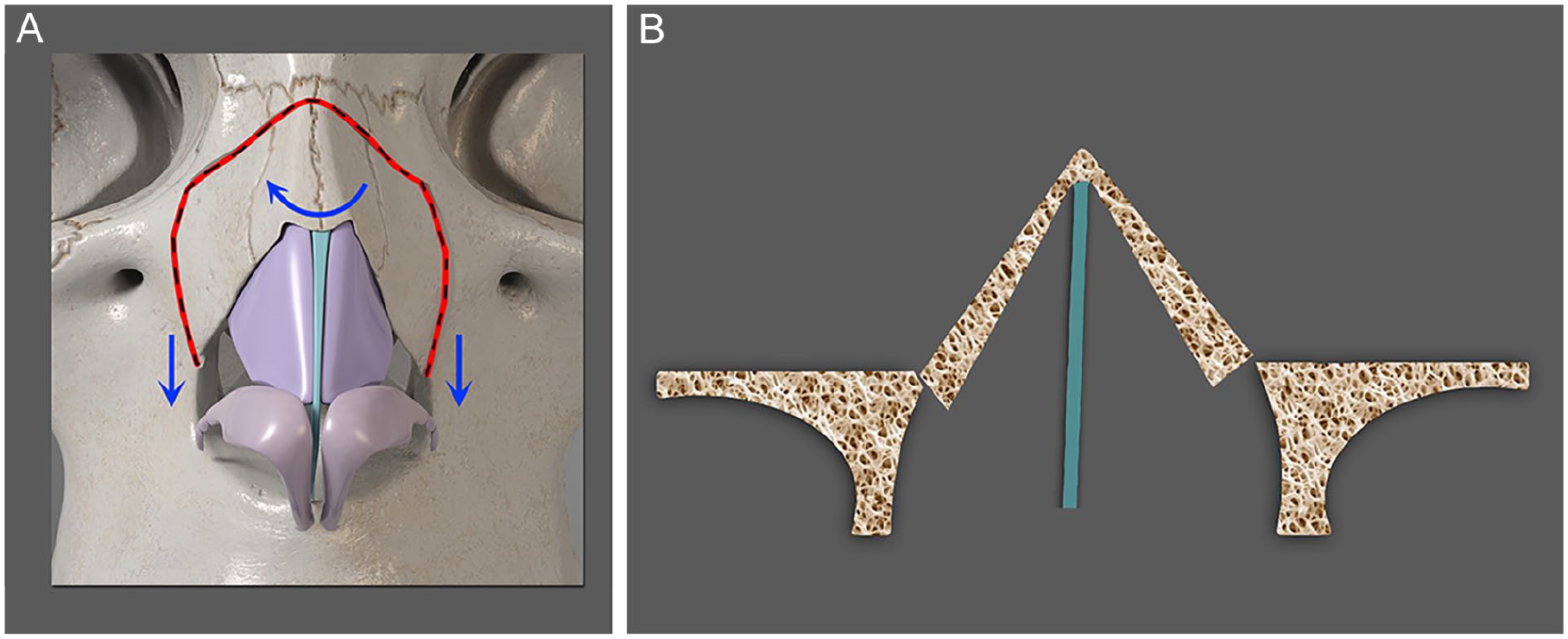
(A) Manual force applied from the deviated side, as indicated by the curved arrow pointing from left to right, results in en bloc movement of the nasal bony vault to the midline. The downward arrows indicate the nasal pyramid is reduced by 1 mm and the ostectomy lines come into contact. (B) Basal view diagram illustrating the straightened nasal structure after correction.
Postoperative Care
The application of ice and the keeping of the head elevated at 30 degrees were recommended, and antibiotics were prescribed for 1 week. The cannulas were removed on the second day. The inner nasal packing and outer mold were removed on day 7. After removing these components, a new external mold was applied to the nose for an additional week. Follow-up examinations were performed 3, 6, and 12 months after the procedure to assess long-term results and ensure successful treatment.
Results
In total, 48 primary cases of crooked noses were operated on. During the 12-month postoperative physical examination, 2 physicians and a resident were present, and the visual analog score was performed by consensus. Two of the 3 physicians’ positive opinions were accepted as satisfactory. In 47 cases, the goal was reached, and the nose was accepted as straightened (Figures 4 and 5). In 1 case, a consensus marked it slightly deviating from the external axis that remained crooked after surgery, but the patient did not request revision surgery.

Frontal view at a patient’s preoperative and 13-month postoperative view.

Frontal view of a patient at 12-month preoperative and postoperative view.
Discussion
Crooked noses are classified into I, S, C, and reverse C shapes.6,7 To better understand the anatomy of a crooked nose, it is divided into upper, middle, and lower thirds. Various modified grafts, suturing techniques, scoring systems, and flap techniques have been used to reconstruct the middle and lower thirds, composed of cartilage.8-11 The upper third, known as the bony vault, is the most challenging part of the crooked noses we focus on. The lengths of the right and left nasal bones in crooked noses differ. Typically, in the upper third, the nasal bone is shorter on the side of the deviation, whereas on the opposite side, the nasal bone is longer. 12
Although double osteotomies, asymmetric lateral osteotomies, and unilateral lateral osteotomies have been used to correct the deviation in the upper third, none of these are standard solutions, prompting the search for new and different methods.6,7 Using a different approach, asymmetric hump resection has been used to equalize the lengths of the nasal bones by taking more from the side of the long nasal bone and less from the side of the short one. This technique has reported successful results. 13
Similarly, a wedge ostectomy is performed between double-lateral osteotomy lines by removing bone to shorten the long nasal bone. 14 Although it is reported to be more effective in correcting crooked noses, the difficulty of determining the amount of bone to be excised and the complexity of the technique have limited its use. 14 The introduction of powered instruments such as PD, PMS, and OD has become popular in rhinoplasty surgery in the last decade. The most important advantage of motorized tools is to perform ostectomy, allowing smooth cuts along desired lines, and achieving the desired amount of bone resection. They result in less swelling and bruising compared to conventional osteotomy. These tools are fast and effective in resecting and shortening the nasal bone, thereby equalizing the length of the nasal bones. PD and PMS are preferred by surgeons who use closed techniques due to their compatibility with conditions characterized by limited visibility; furthermore, they produce less heat and cause less tissue trauma. However, nasal bone cutting and excision, defined as OD-free ostectomy, are much more effective and efficient than others. 9 ODs are readily available and are already present in most ear, nose, and throat clinics.
OD ostectomy is performed with an open extended rhinoplasty approach. The extended open approach has the advantage of freeing the soft tissue envelope, ligaments, and skin, allowing for more effective midline alignment of the nose. 6
A deviation of 5 degrees from the midline may not be noticeable to the eye. Surgeons do not typically want to complete crooked nose surgery without achieving midline alignment. Therefore, the angle formed by the nasion–rhinion line at the midline is mostly reset to zero in the early postoperative period. However, a slight recurrence of this deviation can be observed in the late postoperative period. Two reasons for failing to correct a crooked nose are incomplete osteotomies and resistance between bones in the osteotomy lines. Our goal was to overcome these problems by performing lateral and transverse ostectomies.
Our technique can be used in cases with minimal or no hump, that is when the dorsal hump does not need to be addressed. It is still applicable to cases with a slight hump up to 4 mm and is also compatible with the let-down dorsal preservation technique.9,12
However, it has limitations and cannot be applied in cases with high humps or high radixes, as it relies on maintaining the integrity of the nasal bony vault. Another disadvantage is the steep learning curve; specific techniques and skills are required to use the drill safely in a limited space. Using a protective tip and operating the drill at 15,000 rpm prevent overheating and uncontrolled drill damage to surrounding tissues. To minimize thermal burns, abundant irrigation is necessary during the procedure. ODs operate at higher speeds and temperatures than powered instruments of PDs and PMSs. The use of an OD can also lead to more bruising, swelling, and soft tissue damage due to the need for an open extended rhinoplasty approach. 10
Conclusion
This novel technique involves ostectomies, which means precise bone cutting and excision to equalize nasal bone lengths and create an equilateral triangle in the midline. Therefore, by using ODs, this technique is highly effective in correcting crooked noses. It can be used in cases with minimal or no hump when the dorsal hump does not need to be addressed. With this feature, it aligns with the currently popular dorsal preservation technique. This technique minimizes the resistance between bones, resulting in satisfactory and lasting outcomes. In the future, with the development of different tips compatible with other powered instruments, this technique could also be applied in closed rhinoplasty. Large case series and long-term results regarding preoperative and postoperative deviation angle calculations from the midline are needed to validate this approach further.
Footnotes
Consent to Participate
Written informed consent was obtained from the participants.
Consent for Publication
Consent was obtained from all participants involved in the study for publication.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors contributed at every stage of the manuscript. The authors declared that they had no potential conflicts of interest regarding this article’s research, authorship, and publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. This research was carried out without financial support.
Ethical Considerations
This study complied with the principles outlined in the Declaration of Helsinki. Ethical approval was obtained for the study (Health Sciences University Tepecik Research and Training Hospital Date: 06/06/2023 Decision Number: 2023/05-16).