
Abstract
Rhinoplasty remains one of the most commonly performed aesthetic surgical procedure that demands a meticulous intraoperative precision as well as maximum precaution and control. Nasal osteotomy is a key component to shape the bony vault in aesthetic rhinoplasty, but it is also the so versatile, dangerous, and difficult to learn. The present study aims to evaluate the usefulness of our locator instrument for beginners which is called transilluminating osteotome. The use of transilluminating osteotome instead of guided lateral nasal osteotome is a reliable instrument since it facilitates the localization of osteotome and osteotomy line beneath the soft tissue with a limited damage to the surrounding soft tissues.
Level of Evidence: III
Introduction
The lateral nasal osteotomy is an important step in rhinoplasty to improve the appearance of the nose. This step relates also to various complications such as hemorrhage, edema, ecchymosis, and excessive narrowing that would cause nasal obstruction and asymmetric appearance of the nasal wall. Basically, 2 techniques have been used to achieve a controllable and reliable osteotomy, whose techniques have been analyzed by various studies. 1 The external (percutaneous) perforated technique ensures excellent stability and control and reduces hemorrhage, edema, and soft tissue injury, whereas the internal (endonasal) continuous technique is associated with soft tissue displacement, and, therefore, this technique may increase hemorrhage, edema, and ecchymosis. 1,2 To achieve a planned osteotomy line, the osteotome selection for endonasal osteotomy is important. Osteotome itself must provide the surgeon with a clear sign to localize blunt edge of osteotome during osteotomy, especially for beginners. This is why guarded osteotomes were designed with the guard attached lateral to the nasal bone. Sometimes, the surgeon might not sense the guide of osteotome because of edema or thick skin and therefore large guard can cause soft- tissue trauma. Lighting system can help the surgeon to localize the blunt edge of osteotome easily, and the light can be seen beneath the skin even in the presence of edema or thick skin. 3 -5 Thus, we believe that the illumination system should be helpful to improve teaching for beginners in rhinology.
Materials and Methods
The study protocol has been approved by Medical Faculty, and Hospital Ethics Committee (07/09/2017-72.07.07), and all procedures followed are in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975 as revised in 2008. Informed consent was obtained from all patients in order to be included in the study. Additional informed consent was obtained from all patients whose identifying information is included in this article. Exclusion criteria were as follows: immunodeficiency or any sign of infection at the time of surgery, previous history of all kind of nasal surgery, and nasal polyp or chronic sinusitis. Twenty-five consecutive rhinoplasty patients were included in the study. Lateral osteotomy sides were randomized in all patients so that each patient received transilluminating osteotomy (4-mm unguarded osteotome with lighting system) on one side and conventional osteotomy (a straight 4-mm guarded osteotome) on the other side. Nine patients required additional medial osteotomy. All surgeries were performed by the same experienced surgeon (T.E.). A straight, unguarded osteotome with a blade width of 4 mm was the main part of our transilluminating osteotome. The other part of transilluminating osteotome constitutes a flexible tube of BD Angiocath (Becton, Dickinson, Franklin Lakes, New Jersey), flexible tube of disposable infusion set, 3 M Steri-strips (3M, Maplewood, Minnesot) skin closure application, and Storz light transmission Probe (496 V; Karl-Storz, Tuttlingen, Germany; Figure 1). Light transmission probe is designed for diaphanoscopic localization of the nasolacrimal ducts and fistulae with a diameter of distal tip 0.5 mm for use with fiberoptic light cable by storz (Karl-Storz). We placed the light transmission probe into the flexible tube of disposable infusion set and Angiocath (BD, Franklin Lakes, NJ) to protect the light transmission probe from blood and soft tissue of the nose. Then, the light transmission probe was fastened to lateral part of 4-mm osteotome with 3M Steri-strips skin closure bands. After attaching the light transmission probe to the fiberoptic cable, the transilluminating osteotome is ready for use (Figure 1).
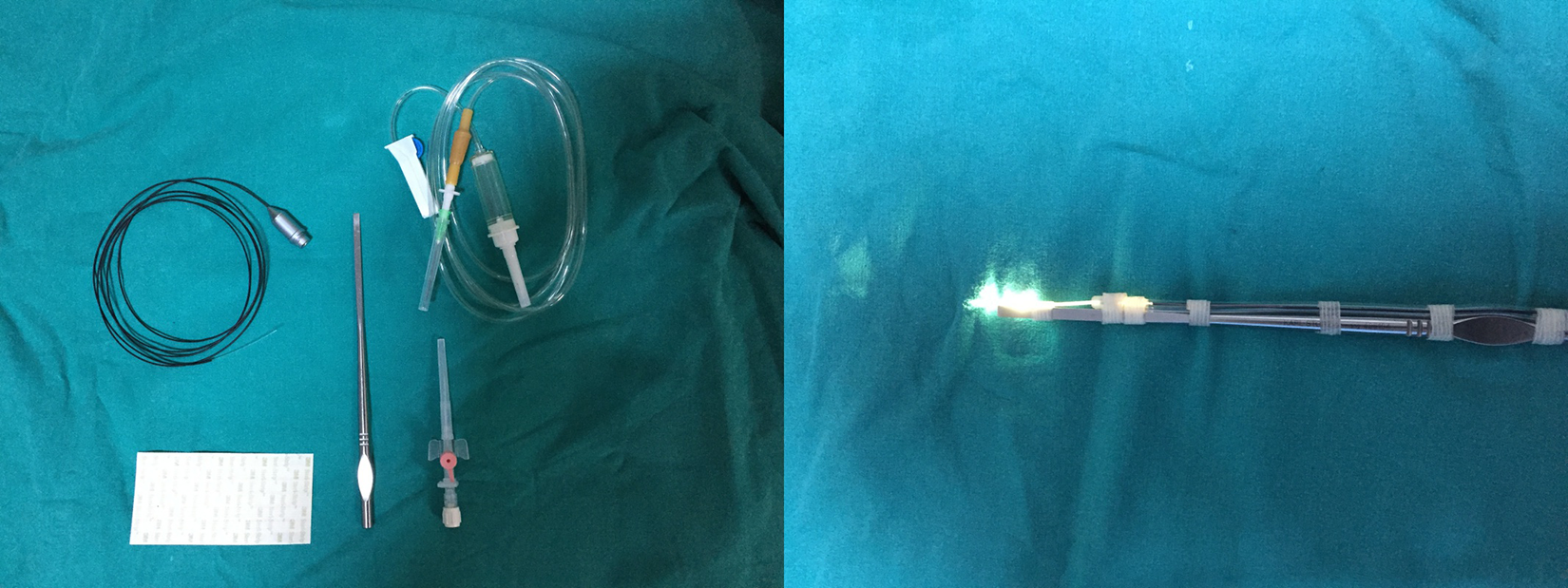
Photo shows transilluminating osteotome with light transmission probe.
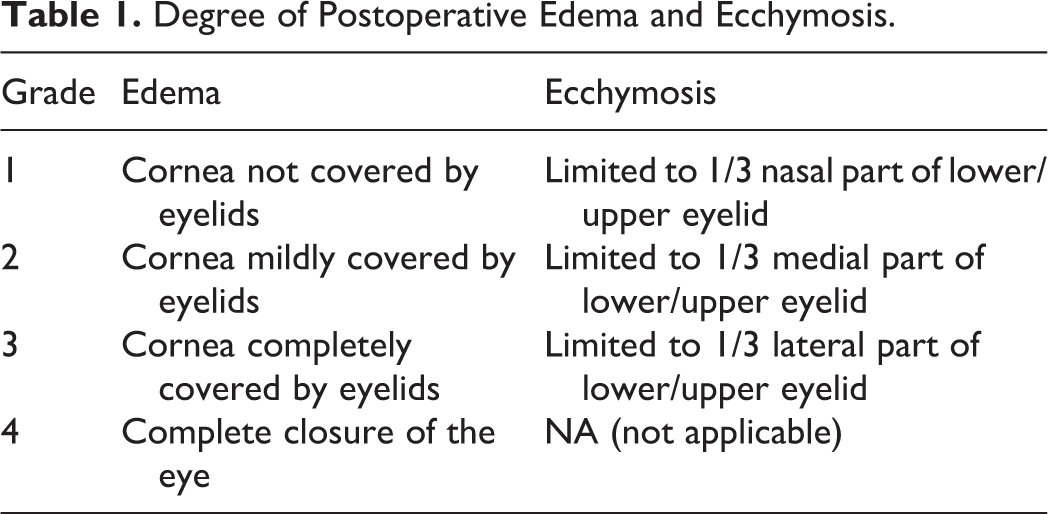
In order to perform lateral osteotomies, the entry sides and pathways were injected 1 to 2 cm3 of %1 lidocaine with 1/100 000 epinephrine along the lateral and medial aspects of the lateral nasal wall. After making a small incision base on priform aperture, a subperiosteal tunnel was created on the lateral nasal bone along the path of the osteotomy line. The transilluminating ostetome is seated on the bone 3 mm above the base of the priform aperture. Low-to-low and low-to-high osteotomies were performed according to the deformity of status. A gentle tap–tap technique is applied gradually to advance the transilluminating ostetome. The osteotome approaches the level of the inner canthus the result of which being the visibility the spot light that could be also followed easily beneath the soft tissue. It is advisable to briefly decrease the external lights in the operating room. No harmful effect could be seen on the lighting system, which might have been based on hitting the osteotome with hammer. The osteotomy was terminated at the level of the medial canthus (Supplemental Video). In the same session on the opposite side, the surgeon used straight 4-mm guarded osteotome. We used ice packing and head elevation for all patients in recreation room postoperatively for the first 4 hours. In order to define the degree of postoperative ecchymosis and edema, we used grading method (Table 1). 6 We evaluated postoperative edema and ecchymosis day 2 for both side of nose using postoperative photographs (Figure 2). The analysis of postoperative photographs was performed blindly. Mucosal tears were inspected on day 2 using 0° rigid endoscope by 2 different investigators objectively.
Degree of Postoperative Edema and Ecchymosis.

Photos show a patient preoperatively (A) and 2 days (B) and 7 days (C) postoperatively.
Statistical Analysis
Data were performed using Statistical Package for the Social Sciences version 13.0 software for Windows (SPSS Inc, Chicago, Illinois). All values were calculated as mean ± standard deviation. Statistical analysis was performed in a blinded manner. Independent samples t test was used for statistical analysis for independent groups; χ2 and Mann-Whitney U test were used for equality of variances. The P value of <.05 was accepted as statistically significant.
Results
All these 50 osteotomies were done between October 2017 and June 2018 ranging in age from 21 to 43 years with an average age of 27 years. Fourteen patients were male and 11 were female. All patients underwent an open rhinoplasty. Direct inspection with 0° endoscope revealed the presence of an intranasal tear in 4 (16%) of the 25 sides applied by straight 4-mm guarded osteotome. Mucosal tears were evident in 3 (12%) of the 25 nasal sides that applied a 4-mm unguarded transilluminating osteotome (Figure 3). There was no statistical difference between the 2 groups regarding the number of mucosal tears (P > .05). A 4-mm guarded osteotome and 4-mm unguarded transilluminating osteotome groups were compared regarding the severity of edema and ecchymosis in the second postoperative day (Figure 4). A decrease was observed in the severity of edema and ecchymosis of the lower and upper eyelid in the transilluminating osteotome group, this decrease was statistically significant in Mann Whitney U test (P values <.05). These data reveal that this practical instrument, which was prepared in operating room, decreases ecchymosis and edema and does not increase the mucosal injury. We did not see any postoperative bleeding and infection in the site of osteotomies.
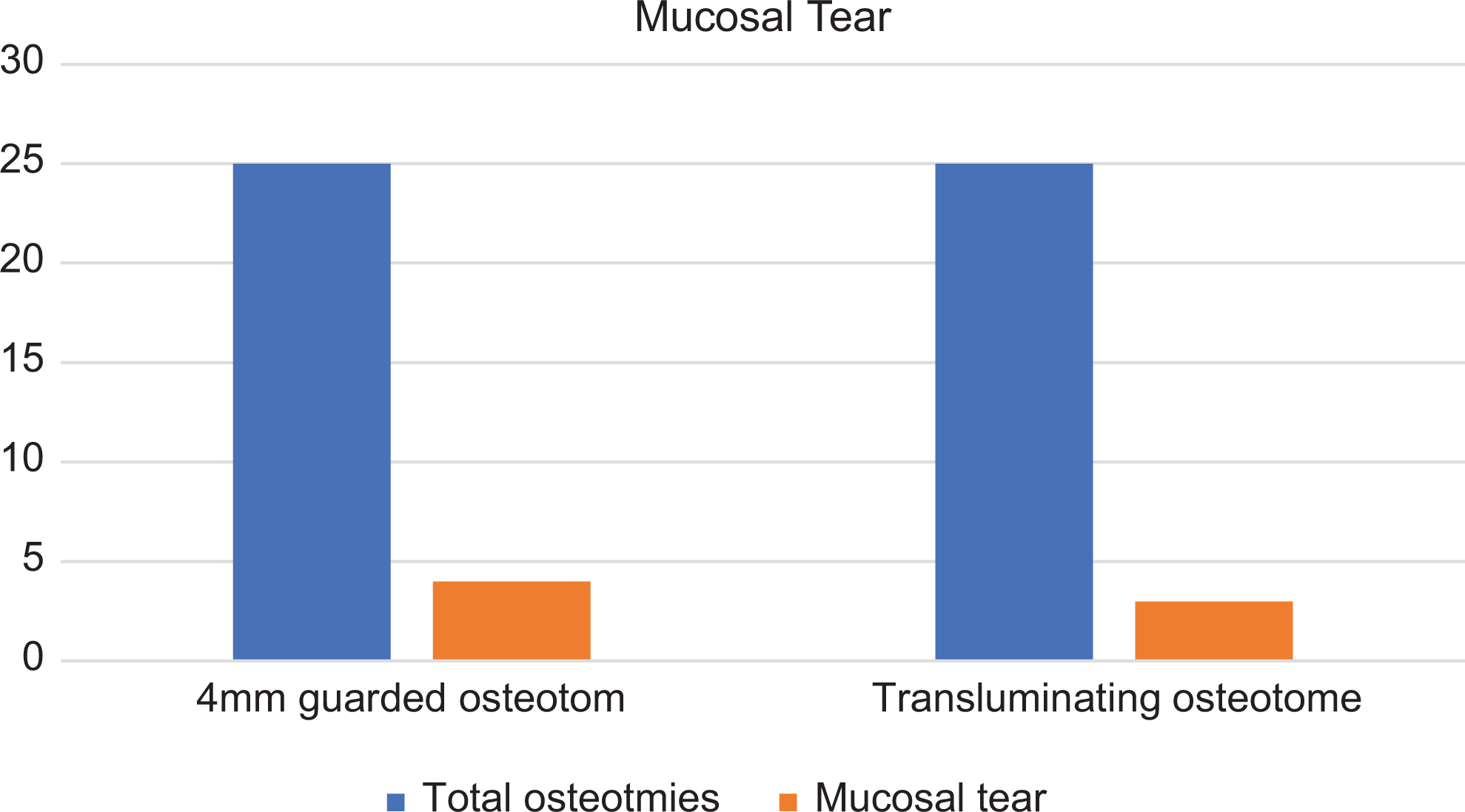
The mucosal tear rates of transilluminating and guided osteotomas.
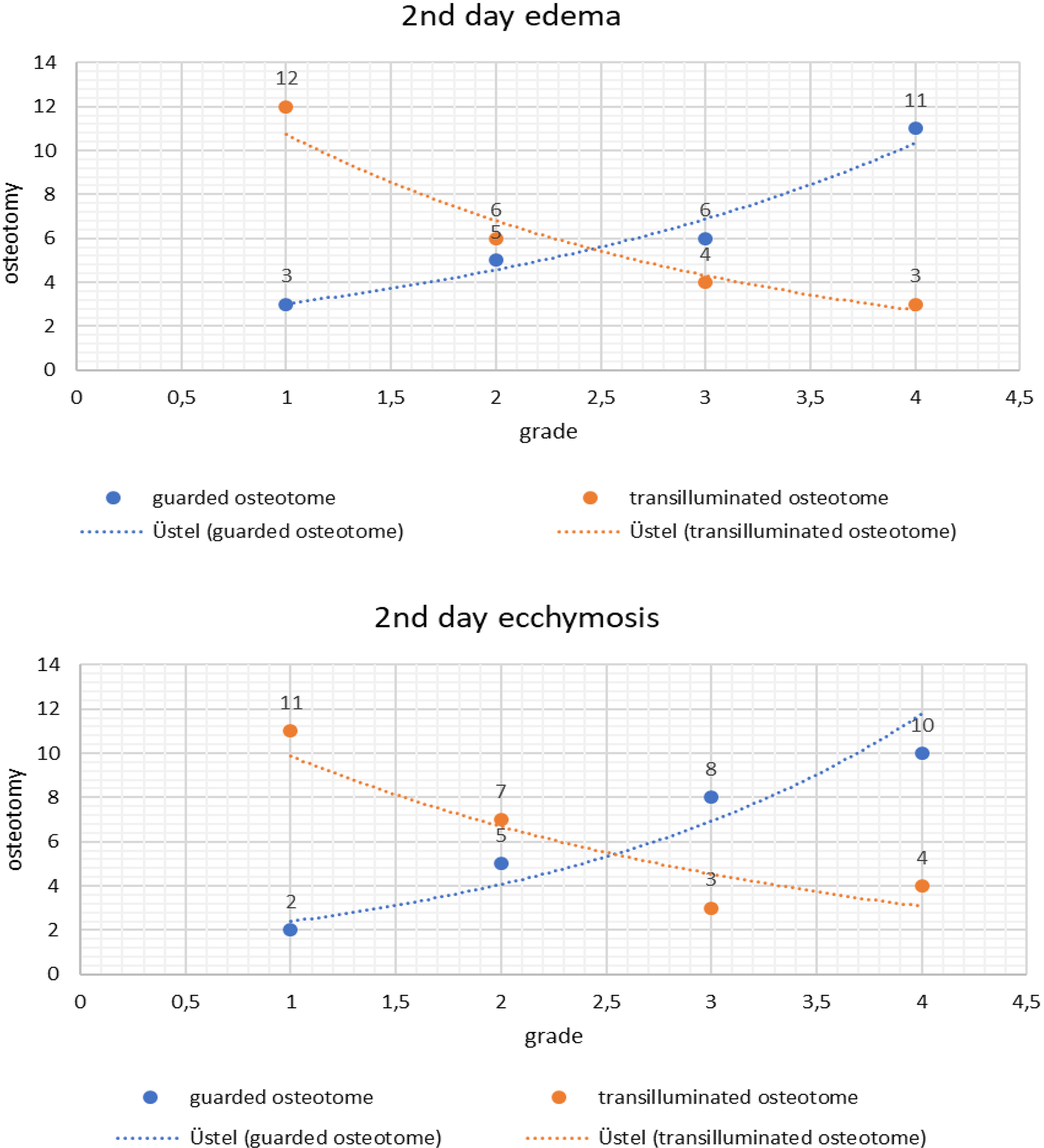
The 2nd day edema and ecchymosis of transilluminating and guided osteotomas.
Discussion
The appropriate choice of surgical technique and the use of correct instrument are important to obtain significant results in rhinoplasty. Various studies have been done to improve the lateral nasal osteotomy and minimize the soft-tissue injuries.
Rohrich et al evaluate intranasal tears using endoscope in cadaver specimens. They compared the percutaneous perforation technique to the internal continuous technique. Rohric et al deduced that the percutaneous perforation technique performs more controlled bony fracture with less intranasal trauma. 3
Helal et al measured nasal airway by computing minimal cross-sectional area using acoustic rhinometry and computed tomography in the pre- and postoperative setting to compare internal continuous and external perforating lateral osteotomy on the internal nasal valve. They observed a measurable decrease in the nasal airway after lateral osteotomy in all patients. Eventually, they found no statistically significant difference between the internal continuous osteotomy and the external perforating osteotomy. 7
Becker et al analyzed important anatomic information for rhinoplasty operations when choosing the size of a guarded osteotome. The authors compared the results from a standard, straight, 4-mm low-profile guarded osteotome with 3-mm and 2.5-mm models. They emphasized that the occurrence rate of intranasal mucosal tears were only of 4% after the 2.5-mm model was employed, whereas 95% of patients experienced intranasal tears with 4-mm low-profile guarded osteotomy. 2 In our study, we used osteotomes of 4 mm on both sides to compare guarded and nonguarded transilluminating osteotome and the results were not statistically significant in terms of mucosal tears. When the illuminating system can be applied to a smaller extent osteotome, it is possible to reduce the occurrence rate of intranasal mucosal tears, such as in the work of Becker et al. It means that rhinologists in training will be able to work with smaller osteotomes.
Ghazipour et al compare postoperative complications of the 2 methods; buccal approach osteotomy and intranasal lateral osteotomy. They found buccal sulcus technique to cause meaningful decrease in the incidence of upper and lower eyelid edema and upper eyelid ecchymosis. 6 In this study, for the first time, we compared 2 different instruments for internal lateral osteotomy regarding edema and ecchymosis. Repositioning the nasal dorsum and narrowing the nasal base can be frightening for beginners. The surgeon rightly desires the sharp instrument in his hand to be under his control and to go where it goes. This is among reasons why researchers have tried various techniques and approaches. We found that transilluminating osteotome is an excellent alternative to traditional lateral osteotomes to correct asymmetric lateral nasal wall contour. The transilluminating osteotome can be easily monitored by the surgeon under the tissue, as it does not increase the severity of ecchymosis and edema. Also, by our method, the light system can be applied to osteotomes in all sizes and thus allow inexperienced surgeons to work with smaller osteotomes.
Gryskiewicz et al have compared the perforating methods to the continuous technique for the same patient with prospective, randomized, and partially blinded study. Gryskiewicz et al confirm the clinical impression that perforating lateral osteotomies with a 2-mm straight osteotome reduce postoperative ecchymosis and edema in rhinoplasty patients compared to continuous osteotomy. 4
Using measurements from preoperative and postoperative photographs, we found that this easy prepared instrument is effective in breaking lateral nasal wall in all 25 study patients.
Byrne et al pointed out that the inside-out lateral osteotomy is an effective technique for lateral repositioning of the bony lateral sidewall of the nose. It is reproducible and accurate and appears to provide greater preservation of the periosteal support of the bony segments than a continuous osteotomy. 8
Zoumalan et al compared the perforation technique to the traditional continuous osteotomy using dorsal width as a surgical end point. Both techniques were found to be effective in reducing dorsal width and there was no statistical difference between the 2 techniques. 9
Continuous method, which is usually performed via an intranasal approach using a smaller osteotome 3 mm width, reduces the mucosal tear. 2 Other options to continuous osteotomies proposed by perforating techniques revealed to have less ecchymosis, less soft tissue trauma while offering same outcomes. 10 Of course, the surgeon must follow the same osteotome line in order to eliminate irregular fracture pattern. Unfortunately, it is difficult to handle small osteotome and follow the same osteotomy line, especially in less experienced hands. 5 Transilluminating osteotome which author design and use meets the surgeon attempt to localize osteotome and follow the osteotomy line easily. According to our opinion, medical engineering will develop this practical tool and it will be put into routine use by surgeons.
Conclusion
The use of transilluminating osteotome instead of guided lateral nasal osteotomy is a reliable technique; it facilitates to localize osteotome and osteotomy line beneath the soft tissue with a limited damage to the surrounding soft tissues. This technique was invented by an experienced surgeon (T.E.) who assists residents during their first attempt to rhinoplasty. We believe that this illuminating system may reduce the failure rate especially in the first stage for the surgeons in training. Experienced surgeons may also benefit when palpation of the osteotome becomes too difficult because of edema. Moreover, authors hope this tool to develop hand in hand with the development of technology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.