
Abstract
Introduction
Chronic rhinosinusitis (CRS) is a chronic inflammatory disease that affects the mucous membranes of the nasal cavity and sinuses. 1 Its prevalence is approximately 5% to 12% of the world population, and it can significantly affect the quality of life and impose a global economic burden.2-4 The economic burden of the disease in the United States in 2011 was estimated to be between $60.2 billion and $64.5 billion. Some patients develop anxiety/depression after treatment. 5 Therefore, the prevention and treatment of CRS is extremely important. Gastroesophageal reflux disease (GERD) is a common comorbidity in patients with CRS, and previous epidemiologic studies have observed a potential correlation between the two, with GERD as a possible cause of CRS.6,7 However, traditional observational studies are subject to reverse causality effects and potential confounders and cannot be used for causal inferences, and high-quality evidence for a causal association is lacking. This is because observational studies cannot remove the effects of factors such as asthma and obesity in patients with CRS, and these factors are also associated with GERD, thus interfering with the study of the correlation between GERD and CRS.
Mendelian randomization (MR) is a research method that explores the causal relationship between traits, using genetic variants strongly associated with exposure as instrumental variables (IVs).8-10 IVs are randomly assigned at the time of human conception and are not subject to potential confounders. Therefore, MR studies avoid the effects of bias and reverse causality, which are difficult to eliminate in observational studies, and are reliable for causal inferences. 11
Our previous MR study explored and confirmed the potential risk factors for CRS. 12 However, we did not explore the causal role and potential for mediation between CRS and GERD. Therefore, we conducted this MR analysis to explore and measure the causal relationship between GERD and CRS. At the same time, we conducted multivariate MR, as well as 2-step MR analyses, to ensure the robustness of this causal association and the potential mediating effects.
Methods
Study Design
Figure 1 presents an overview of the general design of this MR study. This study was conducted according to the 3 main assumptions of MR research. 13 It followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines using Mendelian randomization. 14
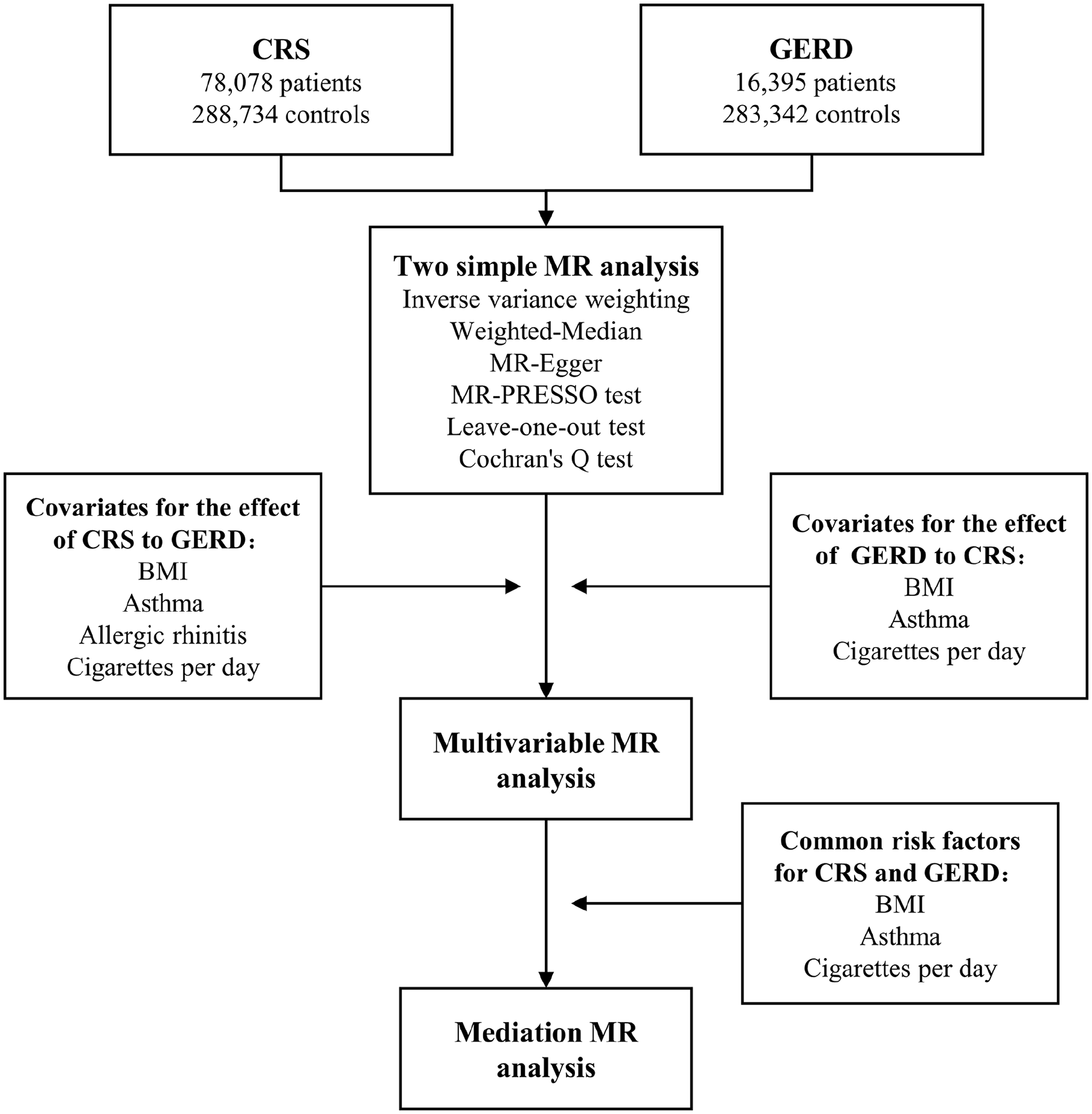
Overview of the general design of our Mendelian randomization study. GERD, gastroesophageal reflux disease; CRS, chronic rhinosinusitis; MR, Mendelian randomization; BMI, body mass index.
First, the causal relationship between GERD and CRS was explored using 2-sample MR analysis. Next, risk factors associated with the dependent variable (outcome) were screened and included as covariates in the multivariate MR analyses to enhance the robustness of the causal relationships. Finally, based on the results of the multivariate MR analyses, 2-step MR analysis was used to explore the potential mediating roles of these risk factors.
The data for this study were obtained from publicly available genome-wide association studies (GWASs). The original GWASs were approved by the relevant authorities; therefore, the need for informed consent and ethical approval was waived for this study.
Selection of IV for CRS and GERD
We obtained data on GERD from the GWAS study conducted at the Berghof Institute for Medical Research. 15 This GWAS study population was primarily derived from the UK Biobank (www.ukbiobank.ac.uk) and Qskin study cohorts, 16 which included 78,707 patients with GERD and 288,734 controls. For CRS, data were extracted from the FinnGen (www.finngen.fi/en), including 16,395 cases and 283,342 controls based on the codes of the International Classification of Diseases, Tenth Edition (ICD-10).
For the exploration of the causal effect of GERD on CRS, the genome-wide significance threshold was defined as P < 5 × 10−8. For the causal of CRS on GERD, the genome-wide significance threshold was defined, as permitted by the MR analysis, as P < 5 × 10−6 because the single-nucleotide polymorphism (SNP) in CRS were less likely to reach the genome-wide significance level of P < 5 × 10−8. SNP with linkage disequilibrium (R2 < .001) and palindromic sequences were excluded. In addition, the MR-PRESSO test was used to identify and exclude aberrant SNP affecting horizontal pleiotropy to ensure the reliability of the selected IV.
GWAS Summary Data on Risk Factors of CRS and GERD
Our previous MR study identified allergic rhinitis (AR), asthma, cigarettes per day, and body mass index (BMI) as risk factors for CRS. 12 In addition, MR studies have confirmed the causal relationship between smoking, BMI, and asthma on GERD.17-19 Thus, AR, asthma, cigarettes per day, and BMI were used as covariates in exploring the causal effect of GERD on CRS. Smoking, BMI, and asthma were used as covariates in exploring the causal effect of CRS on GERD in the multivariate MR analysis. In addition, 3 risk factors common to both, which were smoking, BMI, and asthma, were used to explore the mediating effect of the causal association.
Data for cigarettes per day were obtained from the GWAS & Sequencing Consortium of Alcohol and Nicotine Use, with a total of 337,334 participants. 20 The data for BMI came from the within family GWAS consortium, which included 99,998 participants. The data for Asthma were obtained from the Trans-National Asthma Genetic Consortium, which included 23,948 asthma cases and 118,538 controls. 21 The data for AR were obtained from the Kaiser Permanente Research Program on Genes and included 56,637 participants. 22 Details of the data sources can be found in Supplemental Table S1. We reviewed the acquired GWAS data to ensure that there was no overlap of the participants in each of the above GWAS studies.
2-Sample MR Analysis
We first used 2-sample MR analysis to investigate the causal relationship between GERD and CRS. We used the random effects model of the inverse variance weighting (IVW) approach as our primary research method to reduce the effect of SNP heterogeneity and obtain robust causal estimates. 23 Multiple sensitivity analysis methods, including the weighted median method, MR-Egger method, and Leave-one-out test, were used to ensure the robustness of the results.24,25 We used Cochran’s Q test to assess the heterogeneity of the SNP, and the MR egger intercept method was used to assess their horizontal pleiotropy.26,27 Scatterplots were used to demonstrate the causal relationship between exposure and outcome, and funnel plots were used to assess the heterogeneity of the IV.
In the bidirectional 2-sample MR analysis exploring the causal relationship between GERD and CRS, P < .025 (.05/2) denoted a significant association with a Bonferroni correction for multiple testing, while P-values between .025 and .05 denoted a potential association.
Multivariable MR Analysis and Mediation Analysis
If the causal relationship was confirmed in the 2-sample MR analysis, the risk factors of the dependent variable (outcome) were included as covariates in the multivariate MR analysis, and the causal relationship between exposure and outcome was re-estimated. The causal effect of GERD on CRS was considered independent of the other risk factors if the results remained significant after the inclusion of the covariates. Otherwise, exposure (GERD/CRS) was considered to have a causal effect on the outcome (CRS/GERD) through other risk factors. However, the results of the multivariate MR analysis could only indicate the direct causal effect of the exposure on the outcome for the causal relationship of the exposure with other risk factors, which does not represent the total causal effect where the indirect causal effect is unclear. 28
For this case, we used 2-step MR analysis to explore the mediating effect of exposure on the outcome through other risk factors. 29 The 2-step MR analysis is divided into 2 steps. The first step is to determine the causal effect of exposure on the mediator to obtain α, and the second step is to determine the causal effect of the mediator on the outcome to obtain β. We used the product of coefficients (α and β) method of mediation analysis as the mediation effect. The total effect of exposure on the outcome minus the mediating effect yields the direct effect of exposure on the outcome. In the analysis, the standard error and 95% CI of the mediating effect were calculated using the delta method.
Statistical Analysis
All statistical analyses were performed using the “TwoSampleMR” and “MR-PRESSO” packages in R software version 4.2.3. The F-statistic was calculated using the following formula: F = Beta2/SE2. 30
Results
Causal Relationship Between GERD and CRS
For the causal effect of GERD on CRS, 74 SNP were used as the IVs for GERD (Supplemental Table S2), and the results showed that genetically predicted GERD was associated with an increased risk of CRS. The results of the weighted median method were consistent with the results of IVW, but the results of the MR Egger test were not significant. However, no significant horizontal pleiotropy was detected in this causal association, and therefore, the results of the random-effects model of IVW were regarded as a main effect. For the causal effect of CRS on GERD, 14 SNP were used as IVs for GERD (Supplemental Table S3); however, we did not find the genetically predicted causal effect of CRS on GERD. The results of the MR analysis are shown in Figure 2. The scatterplot demonstrated the association between the outcome and exposure (Supplemental Figure S1).
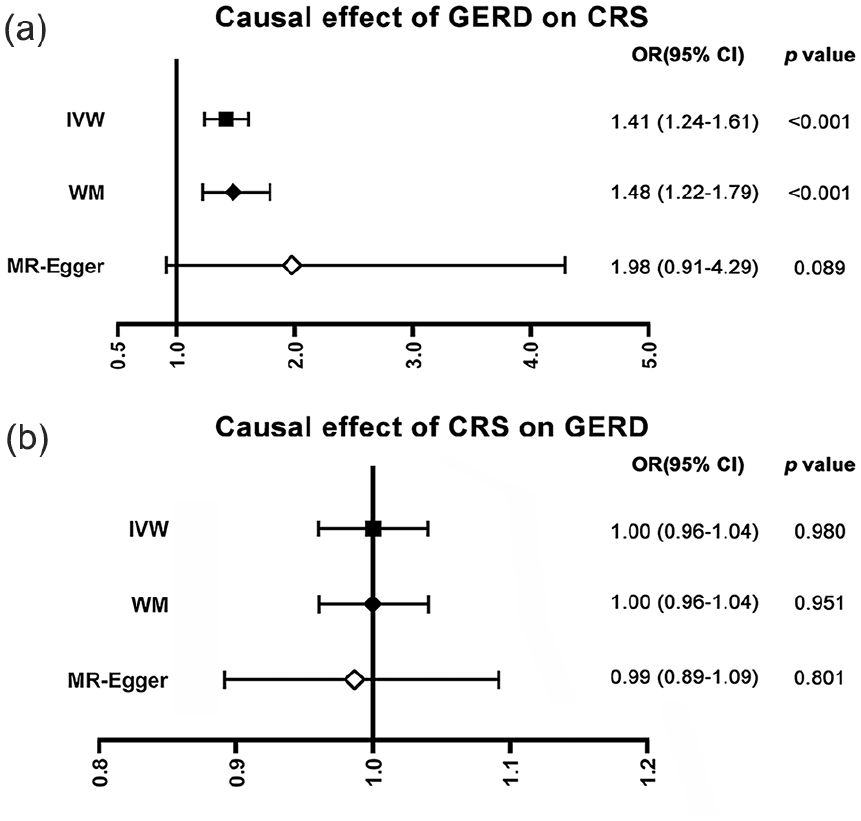
Causal relationship between GERD and CRS. (a) Causal effect of GERD on CRS; (b) Causal effect of CRS on GERD; GERD, gastroesophageal reflux disease; CRS, chronic rhinosinusitis.
Multivariable MR Analysis for the Adjustment of Potential Confounders
We used AR, cigarettes per day, BMI, and asthma as covariates for the multivariate MR analyses to correct for the causal effect of GERD on CRS. The results showed that the direct causal effect of GERD on CRS estimated by multivariate MR was significant. The results are shown in Table 1.
Multivariable MR Analysis for the Adjustment of Potential Confounders.
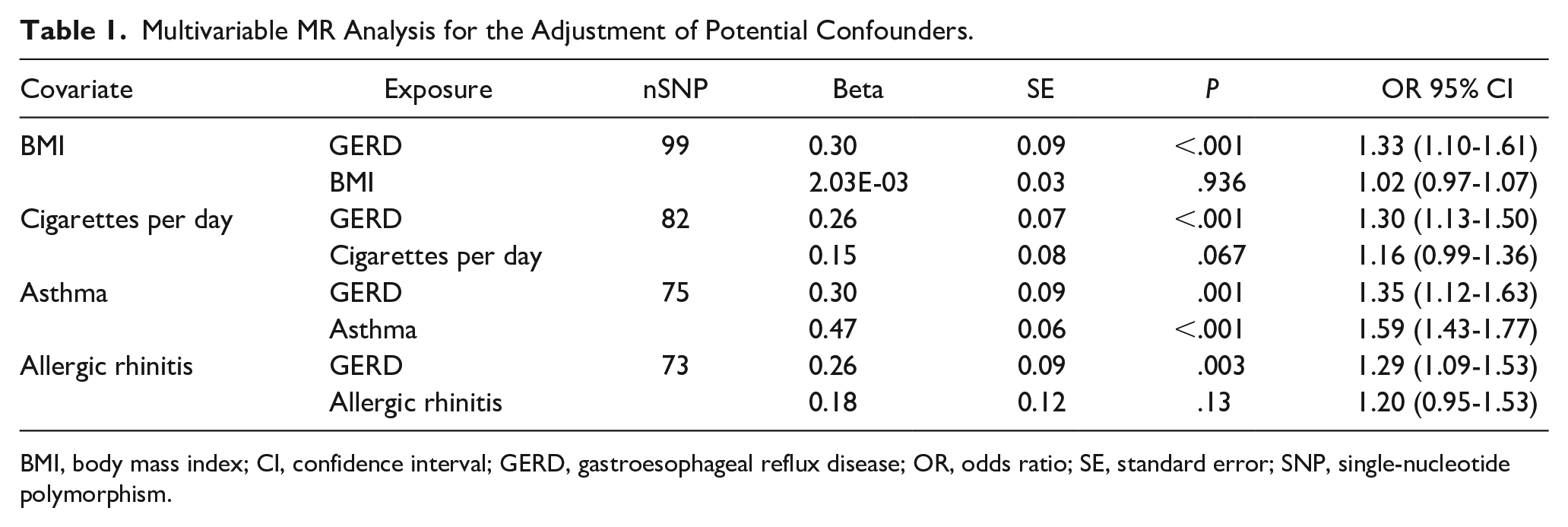
BMI, body mass index; CI, confidence interval; GERD, gastroesophageal reflux disease; OR, odds ratio; SE, standard error; SNP, single-nucleotide polymorphism.
Mediation Effect on the Causal Effect of GERD on CRS
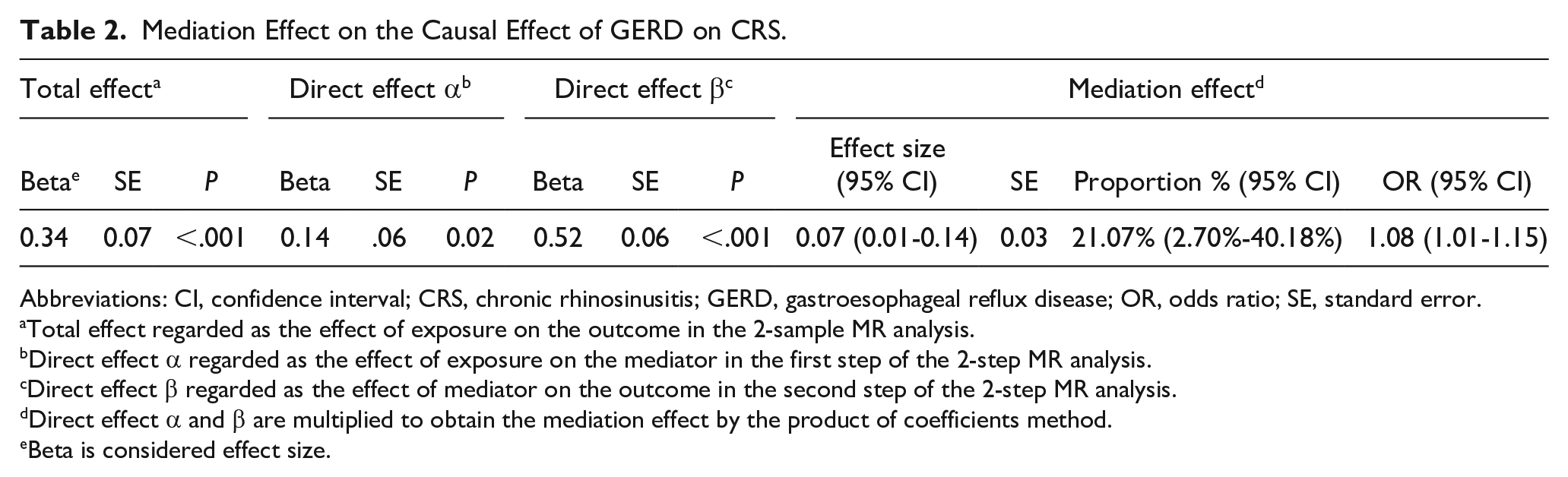
To clarify the indirect causal effect of GERD on CRS, we performed 2-step MR analysis using asthma, BMI, and cigarettes per day. For the first step, 64, 65, and 74 SNP (Supplemental Tables S5-S7) were used as IV of GERD to analyze the causal relationships between GERD and asthma, BMI, and cigarettes per day. The results showed a significant causal effect of GERD on asthma, cigarettes per day, and BMI. For the second step, we redetermined the causal effects of cigarettes per day, BMI, and asthma on CRS to apply to the current analysis. Supplemental Tables S8 to S10 show the instrumental variables in the analyses, and there were no duplicated IV in the 2 MR analyses of the single risk factor involvement. The direction of the causal effects in both analyses was identical to the direction of the causal effect of GERD on CRS. The direction of the causal effect was identical to that of GERD for CRS. However, the multivariate MR analysis showed that the causal effects of BMI and cigarettes per day on CRS became nonsignificant after adjustment for GERD, suggesting that only asthma was involved in mediating the indirect causal effect of GERD on CRS. The results of the 2 MR analyses are shown in Supplemental Tables S11 and S12. Based on the coefficient product method, the causal effect of GERD on CRS mediated through asthma was calculated as 21.07% (95% CI: 2.70%-40.18%), and the results are shown in Table 2.
Mediation Effect on the Causal Effect of GERD on CRS.
Abbreviations: CI, confidence interval; CRS, chronic rhinosinusitis; GERD, gastroesophageal reflux disease; OR, odds ratio; SE, standard error.
Total effect regarded as the effect of exposure on the outcome in the 2-sample MR analysis.
Direct effect α regarded as the effect of exposure on the mediator in the first step of the 2-step MR analysis.
Direct effect β regarded as the effect of mediator on the outcome in the second step of the 2-step MR analysis.
Direct effect α and β are multiplied to obtain the mediation effect by the product of coefficients method.
Beta is considered effect size.
Heterogeneity and Pleiotropy Tests
We excluded SNP with horizontal pleiotropy using MR-PRESSO, which showed that there were no anomalous SNP with significant horizontal pleiotropy in these causal explorations, as shown in Supplemental Table S13. The MR-Egger intercept method also showed no significant horizontal pleiotropy in the study, and Cochran’s Q test found heterogeneity in the reverse MR analysis (Supplemental Table S14). The leave-one-out analysis showed that the results we obtained were not strongly influenced by any single SNP (Supplemental Figure S2). The funnel plot showed no abnormal SNP with significant heterogeneity in the MR analysis (Supplemental Figure S3).
Discussion
The MR analysis revealed the causal effect of genetically predicted GERD on CRS, and multivariate MR analysis confirmed the robustness of this result. In addition, mediation analysis indicated that asthma involvement mediated part of the causal effect of GERD on CRS. Furthermore, our findings do not support the causal effect of CRS on GERD.
GERD is a common comorbidity of patients with CRS and a major concern for rhinologists. A study conducted by Ulualp et al 31 in 1999 found an increased rate of laryngopharyngeal reflux in patients with CRS. Subsequently, several epidemiologic studies have observed a higher prevalence of CRS in the GERD population than in the non-GERD population, further supporting the correlation between CRS and GERD.32,33 In addition, a meta-analysis provided further evidence for a potential association between the two.7,34 However, due to the inherent limitations of observational studies, previous studies were unable to make inferences about a causal association between the two. Meanwhile, our findings provide direct evidence for a causal effect of GERD on CRS, which is a significant strength of MR studies.
A previous prospective study demonstrated that the rate of nasopharyngeal and distal esophageal reflux was significantly higher among patients with CRS who had failed nasal endoscopic surgery than in controls. 35 Another study found that the severity of GERD was associated with postoperative recurrence in patients with CRS without nasal polyps (CRSsNP). 36 Both studies suggest that GERD may be an important causative factor in patients with refractory CRS. However, it has not been established whether intervention for GERD can improve the prognosis of CRS, and previous studies evaluating the improvement of CRS symptoms with proton pump inhibitors have achieved conflicting conclusions.37-40 This study confirms the role of GERD in the pathogenesis of CRS, which implies that treatment for GERD should be a key concern for rhinologists in patients with CRS, especially refractory CRS or recurrent CRS with GERD.
Previous studies have detected pepsin in nasopharyngeal biopsy tissues, nasal secretions, and nasal lavage fluids, respectively, providing direct evidence of gastric reflux into the nasal cavity in patients with GERD, as well as potential explanations for the causal effect of GERD on CRS.41-43 Due to the lack of a mucus-bicarbonate barrier in the nasopharyngeal and nasal mucosa, even small amounts of gastric acid and pepsin can cause irreversible damage, inducing chronic inflammation of the mucosa. The swollen mucosa can also block sinus drainage channels, causing secondary sinusitis. Vagal dysfunction induced by GERD can also lead to edema and dysfunction of the sinus mucosa. In addition, Cvorovic et al 44 detected Helicobacter pylori in the sinus mucosa of patients with CRS and GERD, suggesting that H. pylori infection may also play a pathogenetic role. These results explain why the prevalence of CRS is higher in patients with GERD. Second, the respective studies by DelGaudio et al 35 and Chambers et al 45 also found that this reflux may lead to persistence of CRS without remission after treatment. Therefore, for these patients, concomitant GERD treatment with CRS therapy is warranted.
As a heterogeneous disease with complex etiology, there are several potential etiologies and comorbidities of CRS. 46 In the latest MR study, our team verified the effects of smoking, obesity, AR, and asthma on CRS at the genetic level. 12 In this study, multivariate MR and mediation analyses confirmed the causal effect of GERD on CRS independently of AR, BMI, and smoking but mediated by asthma. The finding of asthma as a mediator is consistent with the results of a more recent study. 47 Furthermore, we found that the mediating effect of asthma was approximately 21.07%. The mechanisms of GERD-induced asthma include the reflux and reflex theories, which link the pathophysiology of the upper gastrointestinal tract to that of the airway. The former refers to mucosal damage to the upper airway by refluxed pepsin and gastric acid, and the latter refers to GERD-induced reflexes of the autonomic nervous system, which manifest as bronchoconstriction.48-51 The unified airway theory, on the other hand, explains the causal effects of asthma on CRS, including the upward spread of airway inflammation and the production of more inflammatory cells and mediators by the body, which induces inflammation of the nasal sinus mucosa.52-54 The results of the present study imply that GERD has an indirect effect on CRS by inducing asthma, in addition to the direct effect. This provides a more comprehensive explanation for the causal association between GERD and CRS. This means that, in the future, we may be able to effectively reduce the incidence of CRS in patients with GERD by targeting the inflammation within the airway in these patients.
Our study has several strengths. First, MR studies can provide high-level evidence for causal associations, and multivariate MR analysis further enhances the robustness of our findings. On top of that, we used mediation analysis to reveal the bridging role that asthma plays in the relationship between GERD and CRS. During the analysis, we used GWAS data from appropriate sources to prevent overlapping samples, and the large sample of the study population, rational MR analysis methods, and multiple sensitivity analyses further enhanced the reliability of the study.
Our study also has some shortcomings. First, the majority of the sample population was European, although GERD affected a small proportion of individuals from the Qskin cohort in Australia and AR affected individuals from the United States who were of European ancestry. Second, this study focused on European populations, and future studies involving other populations should be conducted to further validate the findings of this study. Third, CRS can be categorized into 2 phenotypes, CRS with nasal polyps and CRSsNP, as well as 2 endotypes, eosinophilic CRS and non-eosinophilic CRS. However, we could not differentiate the specific types of CRS because of limitations of the GWAS data.
Conclusion
This study found a causal association of GERD on CRS, with asthma as a mediator, implying that the Unified Airway Theory plays an important role in the mechanism of concomitant CRS in patients with GERD. This provides high-quality evidence of causality and lays the foundation for future clinical and mechanistic studies targeting this association, and clinically, treatments targeting airway inflammation may be able to prevent the development of CRS in patients with GERD.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241286611 – Supplemental material for Causal Relationship Between Gastroesophageal Reflux Disease and the Risk of Chronic Rhinosinusitis: Insights from Multivariable and Mediation Mendelian Randomization Analysis
Supplemental material, sj-docx-1-ear-10.1177_01455613241286611 for Causal Relationship Between Gastroesophageal Reflux Disease and the Risk of Chronic Rhinosinusitis: Insights from Multivariable and Mediation Mendelian Randomization Analysis by Ce Wu, Zengxiao Zhang, Xudong Yan, Lin Wang, Longgang Yu and Yan Jiang in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
Data Availability Statement
All data included in this study were uploaded as supplements and are also publicly available through published GWASs and open GWAS datasets (UK Biobank, FinnGen, the GWAS & Sequencing Consortium of Alcohol and Nicotine Use, the within family GWAS consortium, the Trans-National Asthma Genetic Consortium, the Kaiser Permanente Research Program on Genes).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Natural Science Foundation of China (Grant/Award Number: 81770978).
Ethics Approval
There are no human participants in this article and informed consent is not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.