
Abstract
Background
Over the last few decades, reflux diseases, such as laryngopharyngeal reflux (LPR) and gastroesophageal reflux disease (GERD), have been identified as significant contributors to inflammatory upper aerodigestive tract diseases. Establishing a direct relationship between reflux disease and chronic rhinosinusitis (CRS) is challenging due to the high prevalence of both diseases and their potential for independent coexistence.
Objective
The purpose of this study is to review the existing literature and evaluate the evidence of an association between reflux diseases and CRS.
Methods
A comprehensive electronic search was conducted across multiple databases to identify all studies that investigated the relationship between LPR, GERD, and CRS from January 1, 1950, to June 16, 2022. Only studies with English manuscripts involving adult populations were included, while case series, case reports, and in vitro studies were excluded. The risk of bias was evaluated using The Newcastle-Ottawa Scale for case-control studies and the NIH quality assessment tool for observational cohort and cross-sectional studies.
Results
The search strategy yielded a total of 427 articles, out of which 25 studies examined the correlation between reflux diseases and CRS. The meta-analysis indicated a significant association between the presence of GERD and CRS compared to control groups (P < .001; CI 3.56 [2.25, 5.65]), as well as significantly higher pH values and pepsin detection in CRS patients when compared to healthy individuals (P = .003). Furthermore, all studies that evaluated proton pump inhibitor (PPI) therapy in CRS patients reported positive outcomes, with 93% of CRS patients showing improvement on PPIs.
Conclusion
The existing literature provides suggestive evidence of an association between reflux diseases and CRS, with regards to both prevalence and treatment. Nonetheless, further studies are required to confirm this relationship.
Keywords
Introduction
Chronic rhinosinusitis (CRS) continues to pose a significant public health concern globally, with a prevalence estimated at 10.9% in the Western world. 1 It is widely acknowledged that a considerable portion of patients diagnosed with CRS suffer from a reduced quality of life (QOL). This situation can be further aggravated when combined with additional conditions like asthma, bronchiectasis, and aspirin-exacerbated respiratory disease. 2 The condition is characterized by inflammation of the nasal and paranasal sinuses’ mucosa, resulting in nasal obstruction and discharge, facial pain, and headaches. 3 Various factors and etiologies have been linked to CRS, such as viral infections, asthma and allergies, immune deficiencies, or environmental factors, including smoking or pollution.4,5 Due to the chronicity and complexity of its pathophysiology, CRS has a detrimental impact on the patients’ QOL, productivity, and emotional well-being. 6 Patients with CRS pose a challenge to the medical field as they frequently do not respond to conventional medical and surgical treatments. 7 Therefore, it is crucial to further comprehend the pathogenesis of the disease.
In recent decades, reflux diseases, including laryngopharyngeal reflux (LPR) and gastroesophageal reflux disease (GERD), have been identified as significant contributors to inflammatory upper aerodigestive tract conditions such as asthma, chronic cough, chronic laryngitis, and dental erosions. Prior studies have suggested additional manifestations, such as sinusitis, pharyngitis, and recurrent otitis media. 8 Establishing a direct relationship between reflux disease and CRS is challenging as both are highly prevalent and may coexist independently. 9 Nonetheless, numerous studies have found a link between GERD and CRS.6,7,10 Moreover, this association was more prevalent in pediatric age groups, as several studies have demonstrated.11–13 For instance, Phipps et al 11 observed that 63% of children with sinusitis exhibited GERD, with 79% experiencing improvement in sinus symptoms after GERD treatment. Similarly, Bothwell et al 13 found that 89% of children with medically refractory CRS reported relief of symptoms after anti-reflux therapy, avoiding the need for surgery.
Although the mechanisms underlying the association between reflux diseases and CRS are not fully understood, several theories have been proposed in recent years to explain this relationship. The first theory involves the direct exposure of gastric contents to the nasal sinus mucosa, resulting in inflammation, impaired mucociliary clearance, and obstruction of the sinus ostia, leading to recurrent infections.14,15 The second hypothesis suggests that dysfunction of the autonomic system mediated through the vagus nerve can cause reflex sinonasal swelling, inflammation, and consequent ostial blockage.16,17 The final hypothesis proposes a direct role for Helicobacter pylori colonization in the paranasal mucosa. 18
As the pathogenesis of CRS is not fully understood and the role of reflux diseases in the development of CRS in adults is still uncertain, it is crucial to conduct a literature review to investigate the relationship between reflux diseases and CRS. The objective of this study is to examine the available evidence on the association between reflux diseases and CRS, including their prevalence, pathological mechanisms, treatment effectiveness, and impact on sinus surgery.
Materials and Methods
Study Design and Eligibility Criteria
This review study was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Studies investigating the association between GERD, LPR, and CRS were included, and study designs such as cross-sectional, case-control, clinical prospective and retrospective cohort as well as randomized and non-randomized clinical trials were considered. Only studies with English manuscripts conducted on adult populations were included.
CRS was considered present if diagnosed clinically or using a validated tool such as the European Position Paper on Rhinosinusitis and Nasal Polyps 2020 (EPOS 2020) criteria. CRS is characterized by inflammation of the nose and paranasal sinuses, manifested by two or more symptoms, one of which must be either nasal obstruction or nasal discharge (anterior or posterior nasal drip), along with facial pain/pressure and a reduction or loss of smell. Additionally, endoscopic signs and/or CT changes must be present, such as nasal polyps, mucopurulent discharge, or edema primarily in the middle meatus for endoscopic signs, and mucosal changes within the ostiomeatal complex and/or sinuses for CT changes. All symptoms must have existed for more than 12 weeks.. 18 The studies that did not apply EPOS criteria, relying instead on imaging modalities or nasal endoscopy (NE) for diagnosis, have hindered the establishment of a standardized approach to assess CRS. The diagnosis of LPR/GERD was established if any of the following tests were positive: dual-probe esophageal pH study, single-probe esophageal pH study, oropharyngeal pH monitoring, gastrointestinal endoscopy, esophageal manometry, or pepsin detection.
Information Sources
For the implementation of this systematic review, we conducted an electronic search from January 1, 1950, until June 16, 2022 on the following databases: PubMed, Cochrane Library, Embase, Scopus, and ProQuest Dissertations and Theses Global. We used a combination of keywords and controlled vocabulary (eg, MeSH, EMTREE) to identify studies related to the concepts of “sinusitis,” “laryngopharyngeal reflux,” and “reflux interventions.” Searches were tailored to each database. The search in EMBASE was restricted to adults. No other filters or limits were applied to our search strategy. The full search strategies are listed in Figure 1. We also scanned the bibliography of each study that discussed the association of LPR/GERD and CRS to identify any missed studies from our search strategy.
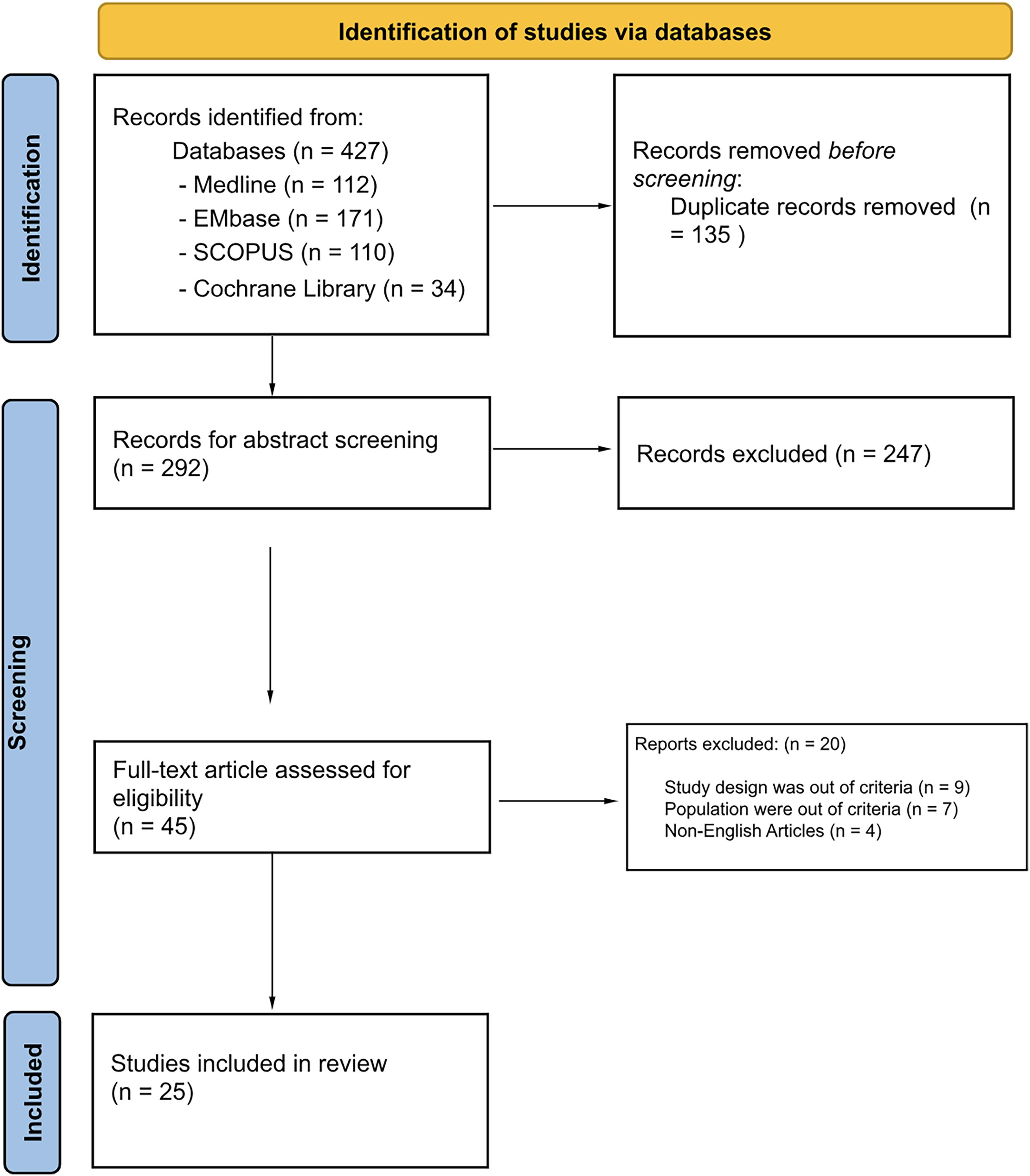
PRISMA flow diagram of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Study Selection
The search results underwent review by two independent authors for each study, without blinding, after eliminating duplicate entries. The initial screening process included evaluating the titles, followed by a brief abstract review. In cases where there was uncertainty or discrepancies, the reviewers engaged in discussions, and any outstanding issues were resolved by involving a third reviewer. Two independent reviewers then conducted a full-text assessment, and studies that met the eligibility criteria were included in the systematic review. Four different study types were identified, and those meeting the inclusion criteria were grouped accordingly into the following categories:
Prevalence of reflux diseases in CRS patients. Levels of pepsin and pH in sinonasal or nasopharyngeal tissue. Effect of anti-reflux treatment on CRS outcomes. Influence of reflux diseases on functional endoscopic sinus surgery (FESS) outcomes.
Data Extraction Sheet
A standardized data extraction sheet was created to fulfill the study's objectives. The full text of these potentially eligible studies was evaluated fully by at least two independent authors. Any disagreement resolved by another author. The following information was extracted for this systematic review: authors, publication year, country, study design, sample size, selection criteria, measurements, and study results.
Risk of Bias
Two authors evaluated each included article for quality and assessed the risk of bias (RoB). A total of 25 articles were evaluated using the Newcastle-Ottawa Scale for case-control studies and the NIH quality assessment tool for observational cohort and cross-sectional studies. These tools allowed for the evaluation of the quality of all parts of the studies, including the introduction, methods, statistical analyses and reporting of results, and discussion of findings. The articles were classified into three categories: high RoB (poor publication quality), moderate RoB (mediocre publication quality), or low RoB (excellent publication quality). The majority of the included studies had a moderate RoB, while only one study had a low RoB. Further details are shown in Figure 2.
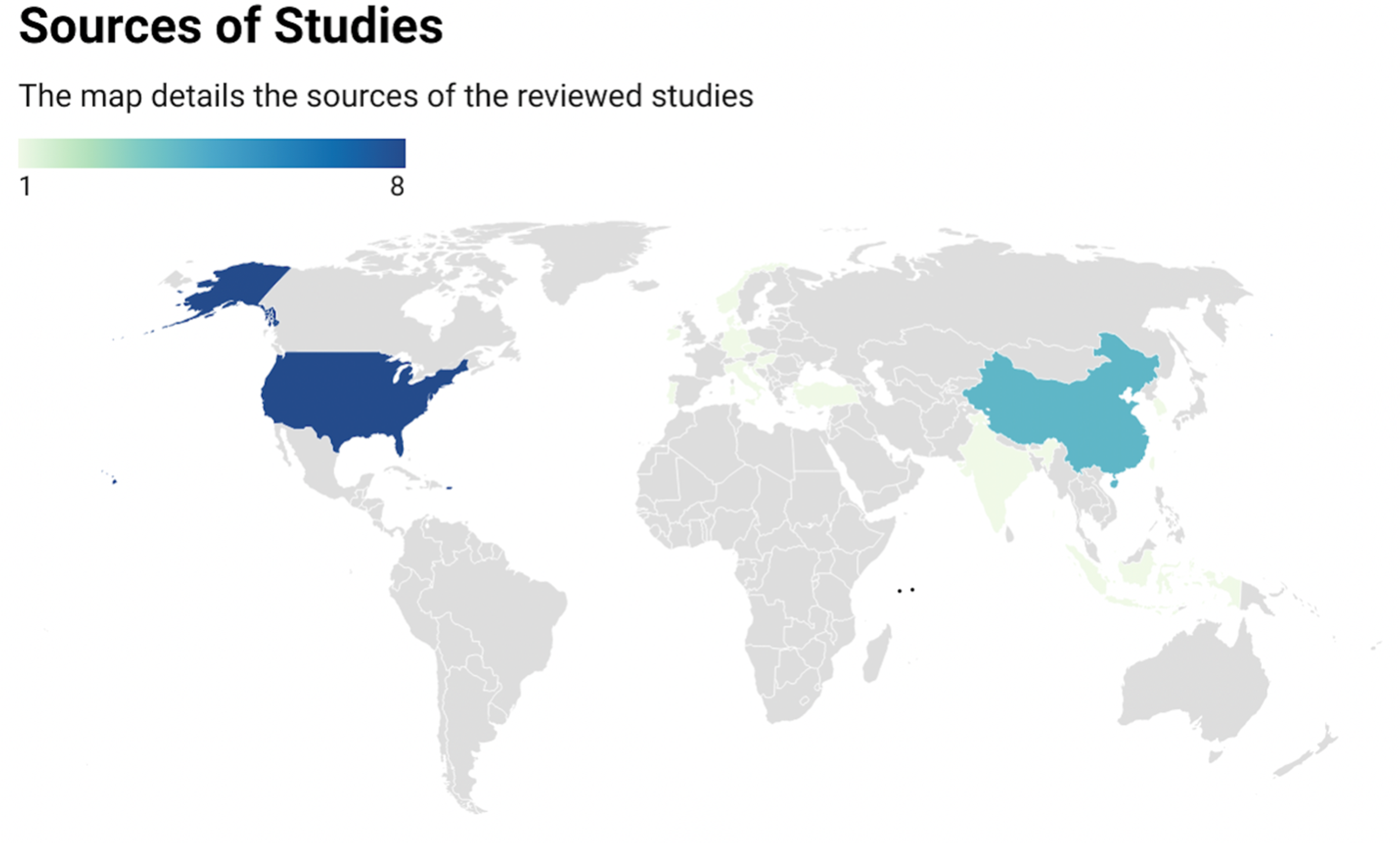
Sources of reviewed studies.
Statistical Analysis
All analyses were conducted using RevMan (version 5.4.1; Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2020). The study results were reported as the weighted rate difference with a 95% confidence interval and were combined using a fixed-effects model. Forest plots were generated to assess the pooling results. A P-value less than .05 was considered significant, and heterogeneity between trials was evaluated using the Higgins I2 test according to the Cochrane Handbook.
Results
A total of 427 articles were identified through the search strategy (Figure 1), out of which 25 studies investigated the association between reflux diseases and CRS. Furthermore, 117 882 patients’ data were pooled from 11 studies to conduct the meta-analysis. The majority of the identified studies were from the United States of America, followed by China. More details about the studies’ origin are shown in the map (Figure 2). The majority of the reviewed studies were observational cohort studies, followed by case-control studies, while clinical trials were a minority. More details are shown in Figure 3. The majority of the included studies had a moderate RoB, while only one study had a low RoB. Further details are shown in Figure 4.
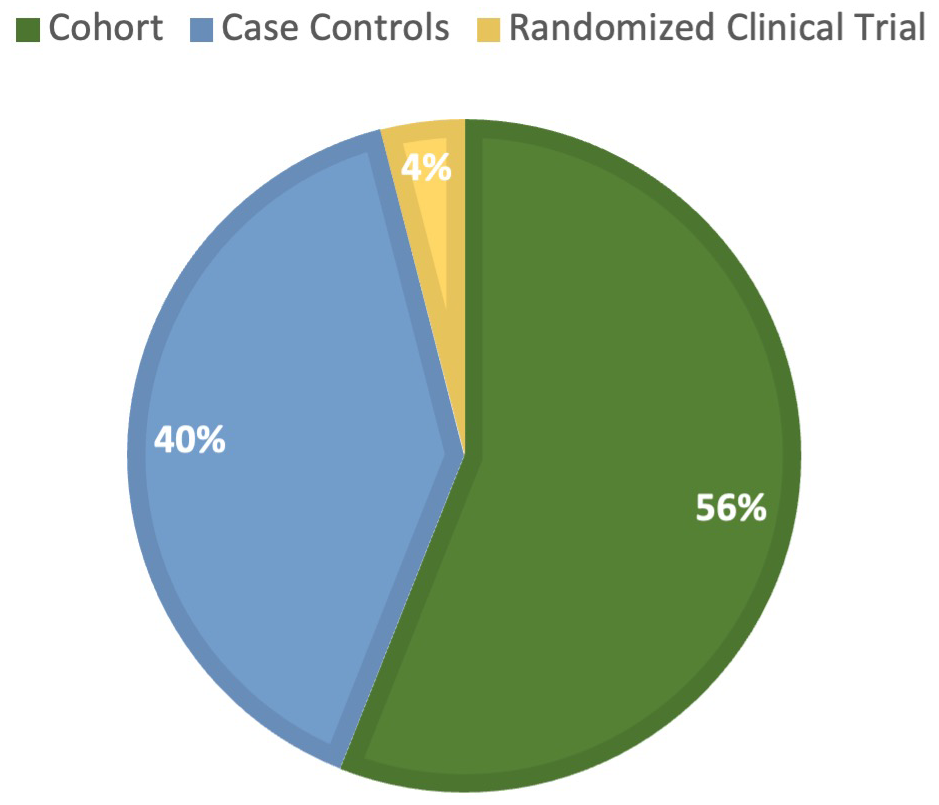
The methodological designs of the included studies.
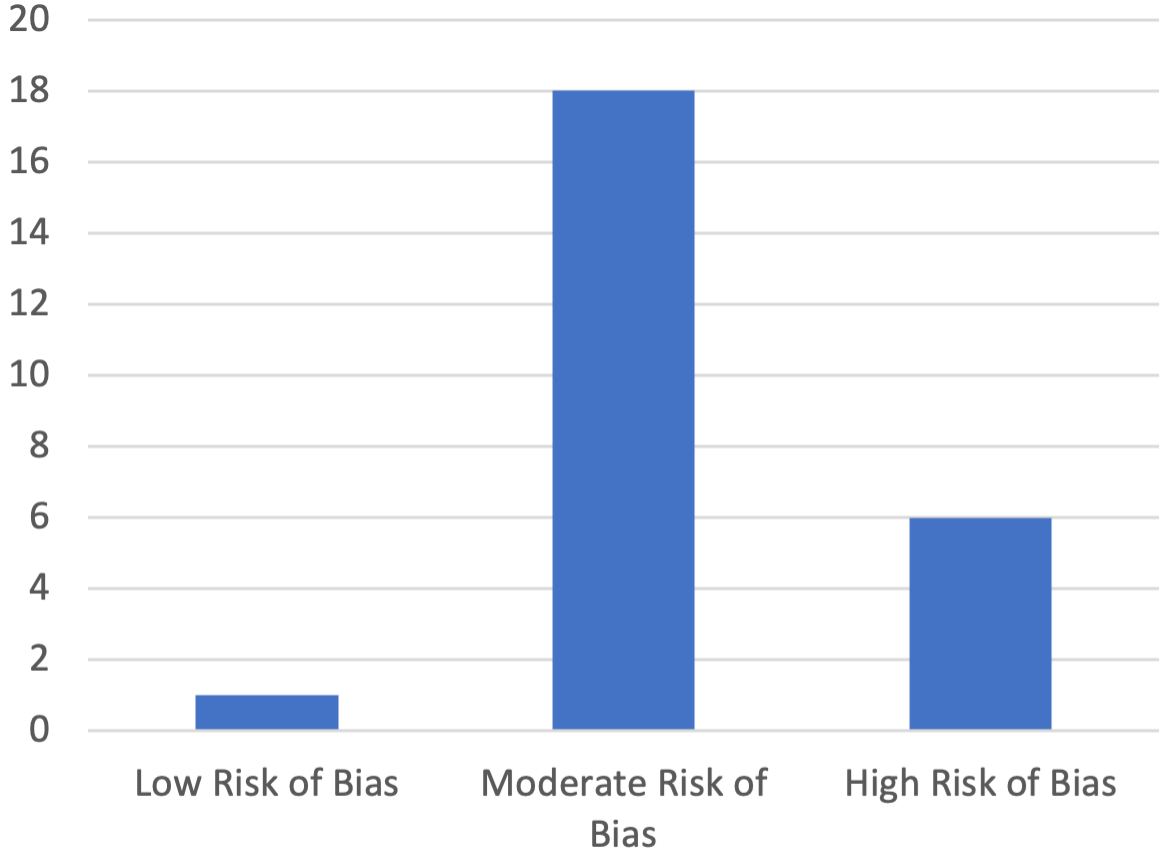
The quality assessment of the included studies.
The Prevalence of Reflux Diseases in CRS Patients
Out of the 25 studies included in this systematic review, 12 reported on the prevalence of acid reflux disease in CRS patients, with a summary of their findings provided in Table 1. A meta-analysis of eight studies involving 117 778 subjects revealed a significant association between GERD and CRS compared to control groups, with a P-value of P < .001; 3.6 [2.3, 5.7]. However, the Higgins I2 test demonstrated significant heterogeneity among the studies, with an I2 of 80%. Further details are presented in Figure 5.
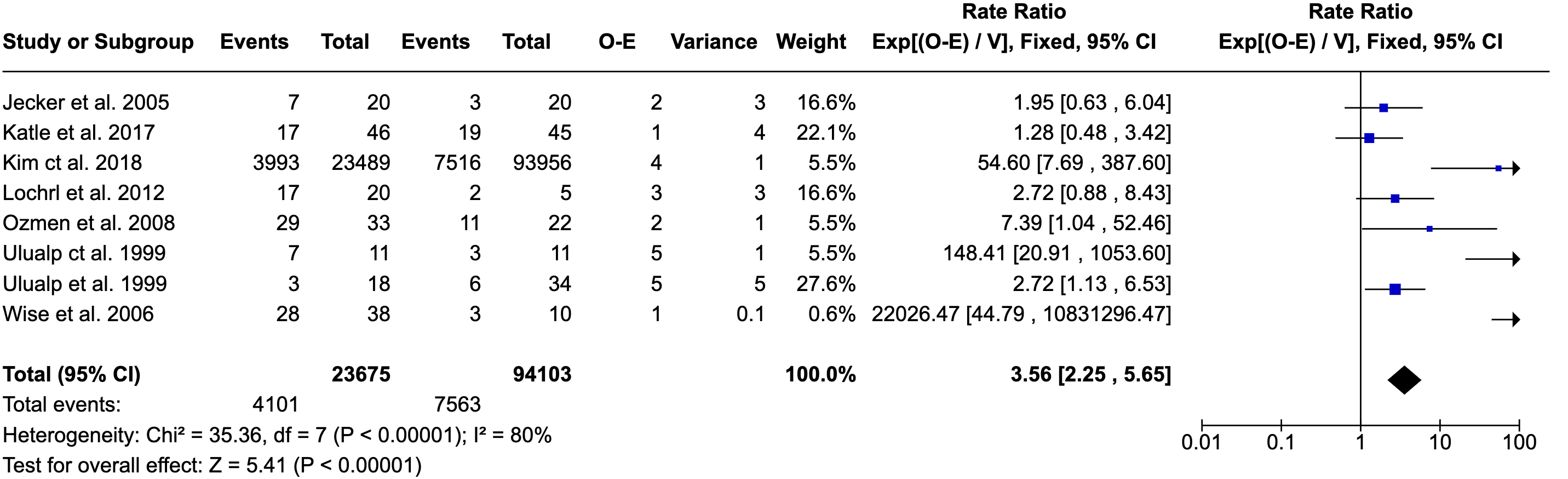
Forest plot of the association of CRS and reflux disease. CRS, chronic rhinosinusitis.
Studies Evaluating the Prevalence of Reflux Diseases in CRS Patients.
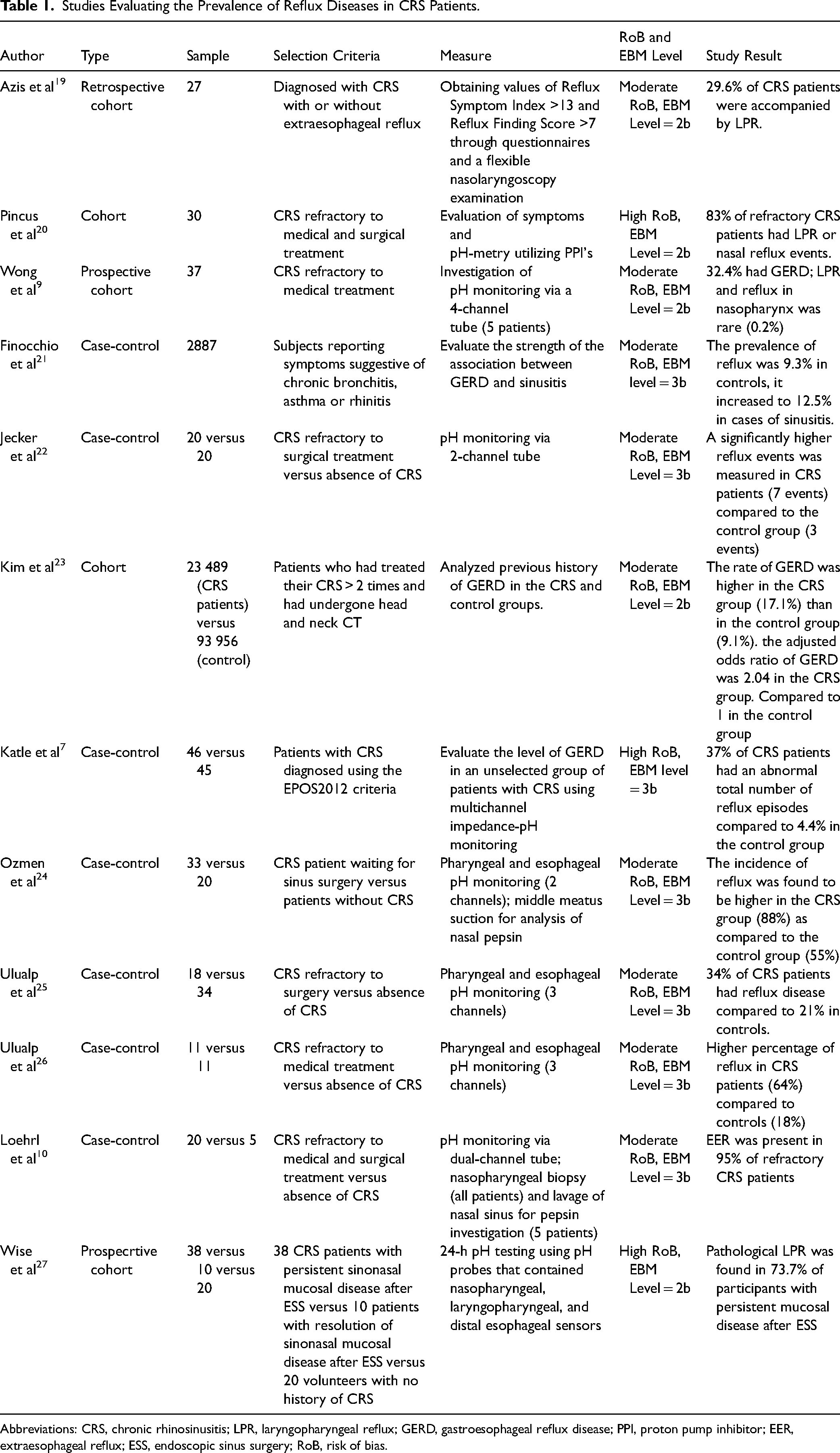
Abbreviations: CRS, chronic rhinosinusitis; LPR, laryngopharyngeal reflux; GERD, gastroesophageal reflux disease; PPI, proton pump inhibitor; EER, extraesophageal reflux; ESS, endoscopic sinus surgery; RoB, risk of bias.
Four other studies also examined the prevalence of reflux disease in CRS patients but could not be included in the meta-analysis. Wong et al reported that 32.4% of CRS patients who were refractory to medical treatment were suffering from GERD. Similarly, Pincus et al found that 83% of CRS patients who were refractory to both medical and surgical treatment had LPR or nasal reflux events. Furthermore, Finocchio et al reported that reflux disease was more common in CRS patients, with a prevalence of 12.5% compared to 9.3% in controls. Azis et al found that reflux disease was present in 29.6% of CRS patients (Table 1).
The Levels of Pepsin and pH in Sinonasal or Nasopharyngeal Tissue
Out of the 25 studies that were included in this analysis, 9 studies measured the pepsin and pH levels in sinonasal or nasopharyngeal tissue of patients with CRS and compared them to control groups. The findings of these studies have been summarized in Table 2.
Studies Evaluating Levels of Pepsin and pH in Sinonasal and Nasopharyngeal Tissues of CRS Patients.
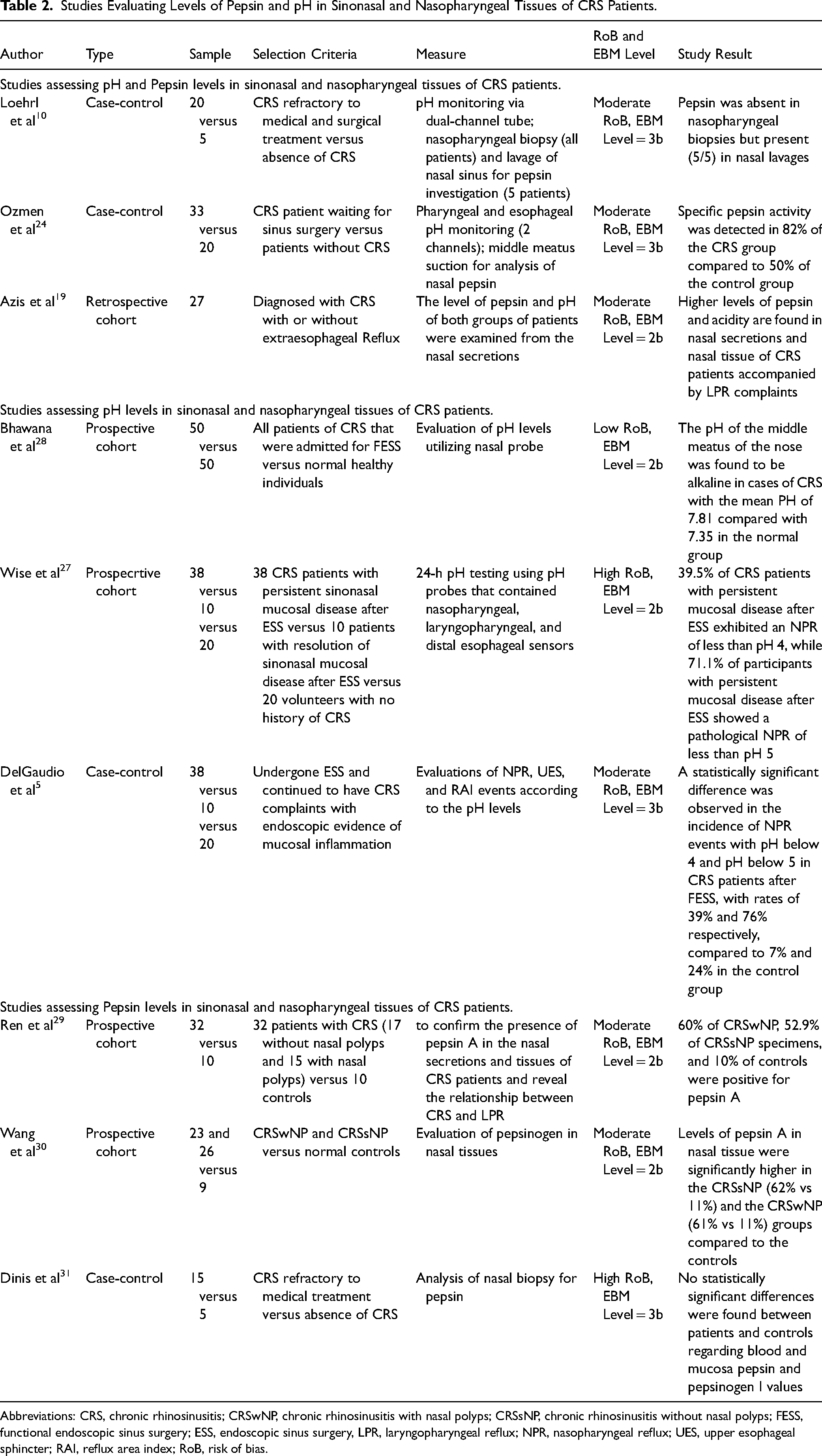
Abbreviations: CRS, chronic rhinosinusitis; CRSwNP, chronic rhinosinusitis with nasal polyps; CRSsNP, chronic rhinosinusitis without nasal polyps; FESS, functional endoscopic sinus surgery; ESS, endoscopic sinus surgery, LPR, laryngopharyngeal reflux; NPR, nasopharyngeal reflux; UES, upper esophageal sphincter; RAI, reflux area index; RoB, risk of bias.
A meta-analysis of three studies (DelGaudio et al Ozmen et al and Ren et al) comprising 104 subjects revealed a significant elevation of pH values and frequency of pepsin detection among CRS patients when compared with healthy subjects, with a P-value of .003. The meta-analysis also showed that CRS patients are 11.5 times more likely to have elevated pH and pepsin levels when compared with healthy individuals. Further details can be found in Figure 6.

Forest plot of elevated pH and pepsin levels in CRS versus without CRS patients. CRS, chronic rhinosinusitis.
In other studies that could not undergo meta-analysis, Wang et al found that levels of pepsin A in nasal tissue were significantly higher in patients with CRS compared to normal controls. Additionally, Loehrl et al found that all CRS patients who underwent nasal lavage were positive for pepsin A, while patients who had nasopharyngeal tissue biopsies for pepsin in their study were found to be negative. Furthermore, Azis et al found that CRS patients with LPR had higher levels of pepsin and acidity in their nasal tissues and secretions when compared to CRS patients without LPR. Moreover, both Wise et al and DelGaudio et al reported that following endoscopic sinus surgery, 39.5% and 39% of patients with CRS had nasopharyngeal pH levels below 4. Additionally, the pH levels of below 5 were observed in 71.1% and 76% of the patients, respectively. In contrast, Bhawana et al found that the pH levels of CRS patients were more alkaline compared to the control group (7.8 ± .8 vs 7.4 ± .8). Finally, Dinis et al found no statistically significant differences between patients and controls regarding blood and mucosal pepsin and pepsinogen I values. Further details about the reviewed studies can be found in Table 2.
The Effect of Anti-Reflux Treatment on CRS Outcomes
Out of the 25 studies reviewed, 4 studies provided valuable data on the effectiveness of proton pump inhibitor (PPI) treatment for CRS patients. Pincus et al, DiBaise et al, Nanda et al, and Anzi et al demonstrated that anti-reflux treatment for patients suffering from CRS could be beneficial in reducing nasal symptoms. Pincus et al reported that over 90% of patients with CRS significantly improved when placed on an anti-reflux treatment (PPIs). Additionally, DiBaise et al found that 81% of CRS patients had an improvement in at least one sinus symptom after 3 months of anti-reflux treatment, with 45% showing improvement in two or more symptoms. Anzic et al compared two groups of CRS patients; the control group received a placebo, while the active treatment group received anti-reflux treatment. Interestingly, CRS and NE scores both decreased significantly more in the active treatment group after 8 weeks when compared to the placebo group. Nanda et al assessed the use of PPI treatment following FESS and found that PPI treatment for CRS patients post-FESS provided greater relief of signs and symptoms compared to the control group who did not receive PPI treatment post-FESS. Further details about the reviewed studies are presented in Table 3.
Studies Evaluating the Effect of Anti-Reflux Treatment on CRS Outcomes.
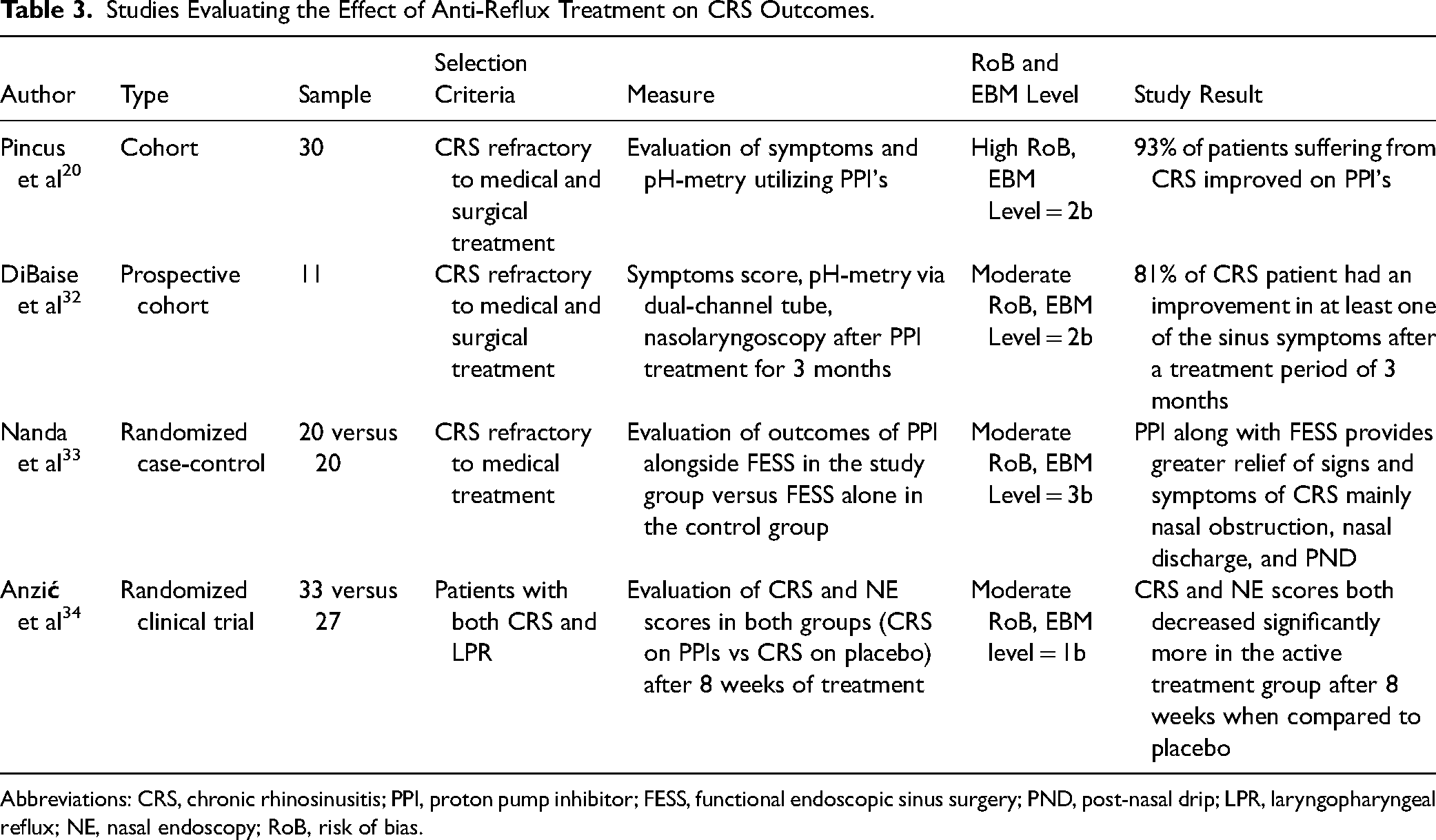
Abbreviations: CRS, chronic rhinosinusitis; PPI, proton pump inhibitor; FESS, functional endoscopic sinus surgery; PND, post-nasal drip; LPR, laryngopharyngeal reflux; NE, nasal endoscopy; RoB, risk of bias.
The Influence of Reflux Diseases on FESS Outcomes
Four out of 25 studies reviewed provided data on the impact of reflux on FESS outcomes. Xu et al found that CRS patients with GERD had higher QOL improvements following FESS compared to those without GERD. However, Chambers et al reported that 41% of CRS patients who experienced poor FESS outcomes had a significant history of GERD. In contrast, DeConde et al and Verim et al found no difference in FESS outcomes between CRS patients with and without reflux disease. More details about the studies assessing the influence of reflux on FESS outcomes are presented in Table 4.
Studies Evaluating the Influence of Reflux Diseases on FESS Outcomes.
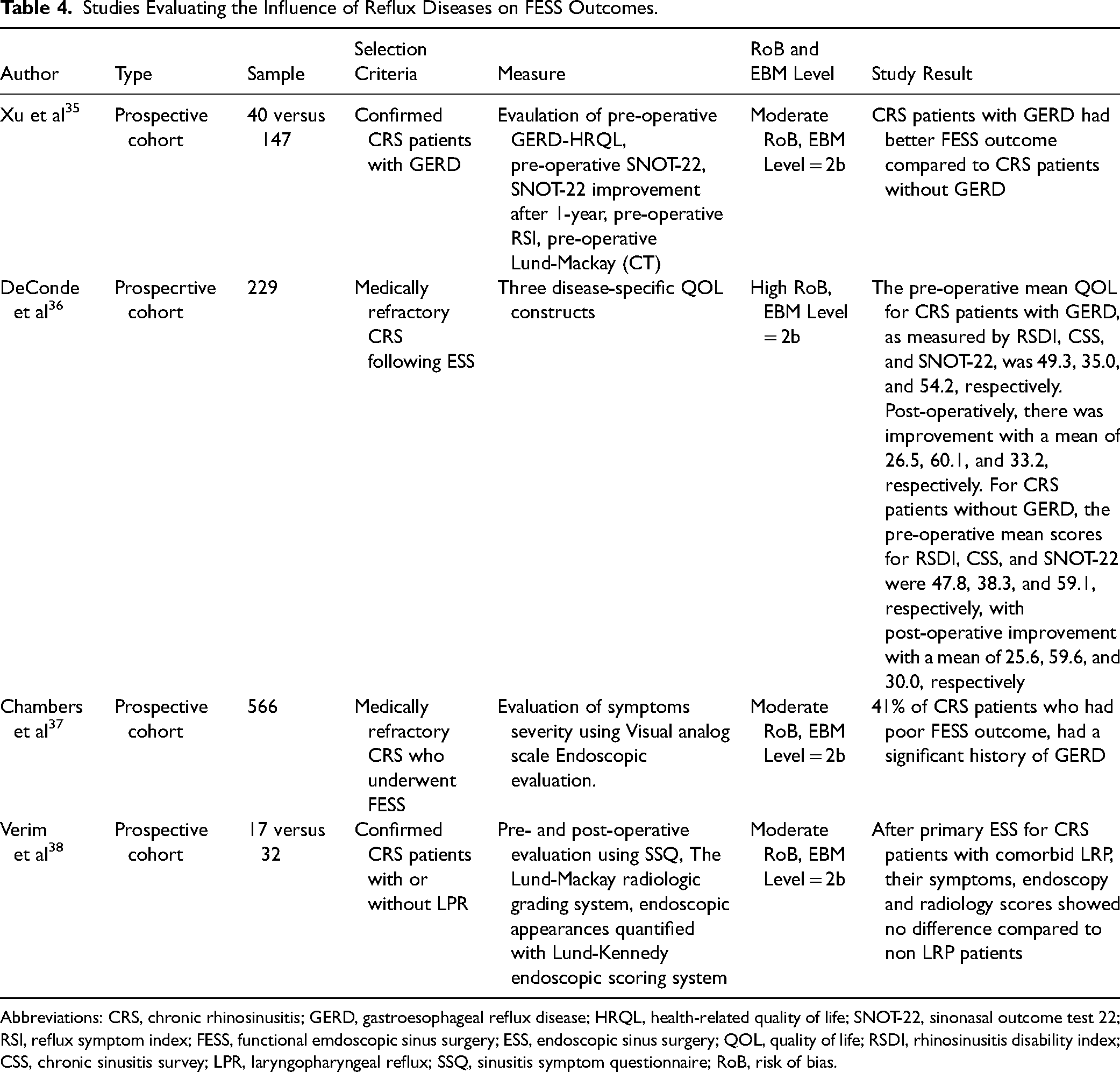
Abbreviations: CRS, chronic rhinosinusitis; GERD, gastroesophageal reflux disease; HRQL, health-related quality of life; SNOT-22, sinonasal outcome test 22; RSI, reflux symptom index; FESS, functional emdoscopic sinus surgery; ESS, endoscopic sinus surgery; QOL, quality of life; RSDI, rhinosinusitis disability index; CSS, chronic sinusitis survey; LPR, laryngopharyngeal reflux; SSQ, sinusitis symptom questionnaire; RoB, risk of bias.
Discussion
A systematic review and meta-analysis of the current literature revealed that reflux diseases, whether it is LPR or GERD, have multiple associations with CRS in various ways. For instance, several reports have demonstrated the ability of gastric acid to reach up to the larynx and nasopharynx.39,40 Multiple studies have assessed the prevalence of acid reflux among CRS patients, particularly those with refractory medical treatment,10,26,41 surgical treatment,27,33,42 or medical and surgical treatment. 40 However, the findings showed high variability among the studies, with some reporting a prevalence above 75% and others as low as 12%. The discrepancy in the prevalence between studies could be explained by the sample size, as larger samples had lower prevalence rates.24,43 The meta-analysis showed a significant correlation between the presence of GERD/LPR and CRS, indicating a significant association between the two conditions.
In the majority of the studies reviewed, impedance-pH monitoring was used to assess reflux diseases, which is considered the gold standard tool for diagnosing GERD and LPR, thereby providing reliable results about the presence of reflux disease. However, in CRS diagnosis, several studies did not adhere to a validated clinical criterion, such as the EPOS 2020 guidelines, which raises concerns about the accuracy of the reported cases of CRS. Nevertheless, the results of all current studies concur regarding the established association and relationship between recalcitrant CRS and reflux diseases, supporting the notion that such a relationship exists based on the available evidence.
The impact of reflux on patients can exhibit a range of effects, spanning from being entirely asymptomatic to manifesting multiple symptoms like hoarseness, cough, or globus sensation, as reported by Koufman et al 44 We posit that the diversity in these outcomes could be attributed to a constellation of intricate individual factors. In the context of the larynx, even a mere frequency of three reflux episodes per week can give rise to significant ailment, as articulated by Koufman et al. 45 This correlation is tied to the compromised defenses of the laryngeal epithelium.
The activity of pepsin-A in the laryngeal epithelium has been extensively researched.42,43 In this review, most included studies found high levels of pepsin-A in CRS patients compared to controls, with some discrepancies in pepsin levels in different types of collected samples. These discrepancies could be attributed to the sensitivity of anti-pepsin-A antibodies, the single-detection method used in some studies, or the timing of sample collection. The reason for high nasal tissue pepsin-A levels remains unclear, whether due to gastric acid reflux or serum effusion. However, one study found that when comparing nasal pepsin-A and laryngeal pH levels, the pepsin assay was 100% sensitive and 92.5% specific to LPR. 24 Thus, high pepsin-A levels found in CRS patients in this review could indicate a high comorbidity of LPR among these patients. Regarding nasal tissue pH levels in CRS patients, conflicting results were demonstrated with one study reporting an alkaline pH, while others reported an acidic pH. The meta-analysis revealed that patients with CRS were 11.5 times more likely to have elevated pH and pepsin levels compared to healthy individuals.
The use of PPIs in the management of LPR is still a matter of controversy, as some studies have shown significant improvement,34,41,46,47 while others have reported no superiority over placebo if treated for 4 weeks or less. 47 This suggests that the effectiveness of PPIs depends on the dose and duration of treatment, with Karkos et al 48 recommending that PPIs be prescribed for 2 to 6 months. 49 Moreover, the conflicting response to PPI treatment could be attributed to the role of non-acid refluxate in inducing such symptoms. PPIs have also been proposed as an alternative treatment for recalcitrant CRS in several studies. A systematic review of the current literature revealed that PPIs are effective in relieving CRS symptoms refractory to medical and surgical treatment. In Anzić et al's study, although CRS and LPR symptoms improved significantly with 20 mg omeprazole over 8 weeks, most patients still had active disease at the end of the trial. 34 Although with a small sample size, DiBaise et al assessed CRS symptoms at 4, 8, and 12 weeks of PPI treatment, with most patients showing improvement at 8 weeks, but the majority showing dramatic improvement by 12 weeks ranging from 25% to 89%. 32 This could explain Anzić et al's findings, highlighting the need for a higher dose or longer duration of treatment. 34 Furthermore, in Nanda et al's study, greater improvement was observed in patients who took PPI following FESS than in those who did not, especially after 3 months. 33
Based on the available evidence regarding the association between reflux diseases and refractory CRS, 4 studies specifically examined the outcomes of FESS in cases with or without comorbid GERD/LPR. The majority of these studies assessed surgical outcomes using disease-specific QOL questionnaires, while only one used a visual analog scale (Chambers et al), which is a non-specific method for assessing post-operative QOL in CRS patients. Interestingly, only Chambers et al found that GERD had a negative effect on the outcome of FESS. On the other hand, in 2021, Xu et al found the opposite, with greater improvement after FESS in patients with a significant history of GERD. The other studies found no significant difference in FESS outcomes between GERD and non-GERD patients.
Due to the conflicting findings, a definitive conclusion cannot be drawn from the aforementioned studies. Nevertheless, it was anticipated that the presence of GERD would have an adverse impact on the post-FESS outcomes in CRS patients, given the high incidence of GERD in refractory CRS cases. It is our belief that further studies, utilizing standardized methods to evaluate the QOL of patients with comorbid GERD after FESS, are necessary to either confirm or disprove the existence of such an influence.
Our study aligns closely with the findings of Leason et al, 50 confirming the established association between acid reflux and CRS. Additionally, we have contributed supplementary evidence substantiating the beneficial impact of PPIs on the outcomes of CRS patients. This benefit is observed whether PPIs are administered as standalone treatment or subsequent to FESS, as demonstrated by Anzic et al 34 and Nanda et al. 33 These findings serve to underscore the role of GERD in hindering the successful resolution of CRS through medical or surgical interventions, a facet not definitively ascertained by Leason et al. 50 It's important to note, however, that the presence of GERD did not exert any noticeable impact on the outcomes of FESS, as reported by Xu et al 35 and Verim et al 38 Furthermore, our research introduces additional supporting evidence that highlights elevated levels of pepsin in CRS patients when compared to control groups, a fact established by the studies of Ren et al 29 and Wang et al 30 This phenomenon is particularly prominent in the subgroup of CRS patients with LPR, as opposed to those without, as demonstrated by Azis et al 19
Our systematic review encountered several limitations. Firstly, due to language constraints, we only accessed studies that were published in English. Additionally, the lack of universal adoption of EPOS criteria to evaluate CRS hindered our ability to establish a standard method for CRS assessment. Moreover, the studies reviewed in this systematic review did not provide sufficient information about the extent of FESS surgeries performed. Furthermore, our review included a substantial proportion of case-control study designs, where the compared study groups or populations had inherent differences. Moreover, only one eligible randomized clinical trial was found to be included in this review. Additionally, the overall lack of substantial evidence-based medicine, combined with the scarcity of multiple eligible randomized clinical trials, undermines our ability to confidently provide recommendations. Finally, the substantial heterogeneity among the included studies posed a challenge to conduct a comprehensive meta-analyses.
Conclusion
There is suggestive evidence from the literature supporting an association between reflux diseases and CRS. The majority of the included studies have reported a high prevalence of reflux diseases among patients with CRS. In terms of treatment, most of the studies have shown that recalcitrant CRS patients could benefit from PPIs if given the proper dosage and duration. Additionally, while some studies suggest that GERD may negatively impact FESS outcomes, this was not demonstrated in all studies. Despite the suggestive association between LPR and CRS shown by this meta-analysis, a cause-effect relationship has yet to be established, and further related studies are still required to confirm such an association.
Footnotes
Author's Note
Fahad Alhussain is considered a co-first author and contributed equally to the first author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.