
Abstract
Granular cell tumors (GCTs) are uncommon neoplasms, often originating from Schwann cells, with granular cytoplasm being a hallmark feature. Laryngeal GCTs, comprising 3% to 10% of cases, present diagnostic challenges due to their resemblance to squamous cell carcinoma. We present a case of a 46-year-old male with throat pain, diagnosed with a laryngeal GCT. Histopathological examination and immunohistochemistry confirmed the diagnosis. Laryngeal GCTs typically manifest as small, firm submucosal nodules, posing challenges in differentiation from vocal fold polyps. Diagnosis relies on histological examination, with characteristic features including eosinophilic granular cytoplasm and positive staining for specific markers. Malignant transformation, though rare, necessitates vigilant monitoring and accurate diagnosis. Treatment involves complete surgical excision with long-term follow-up to detect recurrence. This case underscores the importance of awareness and accurate diagnosis in managing laryngeal GCTs, ensuring timely intervention and optimal patient outcomes.
Introduction
Granular cell tumor is an uncommon soft tissue neoplasm with uncertain origin of cell type. Electron microscopy and immunohistochemistry studies suggest that it likely originates from Schwann cells. This tumor is characterized by granular cytoplasm due to the accumulation of secondary lysosomes, leading to its name, although this histological characteristic is nonspecific.1,2 Granular cell tumors tend to be solid and homogenously enhanced on CT scans, often mimicking a squamous cell carcinoma.
Granular cell tumors can develop in any part of the body, with around 50% occurring in the head and neck region. Laryngeal granular cell tumors make up 3% to 10% of all cases.3-5 Less than 2% of these tumors are malignant and they have a poor prognosis. 2
Case Presentation
A 46-year-old male patient presented to ENT outpatient department with complaints of throat pain for 3 months, with no history of change in voice, difficulty breathing, difficulty swallowing, painful swallowing, loss of weight, and loss of appetite. On examination by video laryngoscopy, a small white nodule was seen in the interarytenoid region (Figure 1A) with no congestion of arytenoids and the false and true vocal cords are anatomically and functionally normal. Clinically, the lesion was more in favor of a benign lesion, so the patient underwent microlaryngeal surgery and an excision biopsy (Figure 1B). Histopathology reported as sections show a polypoidal fragment lined by hyperplastic stratified squamous epithelium. There is focal ulceration with underlying lobules of mucus glands. The stroma reveals a well-circumscribed lesion composed of sheets of cells with moderate to abundant eosinophilic granular cytoplasm (Figure 2A). The nuclei are oval, with no evidence of mitosis or necrosis. The cells are observed entrapping the glands. Features are suggestive of a granular cell tumor, and immunohistochemistry for S-100 is recommended for confirmation. The S-100 stain shows strong cytoplasmic positivity in 100% of tumor cells (Figure 2B). These features are consistent with granular cell tumors.
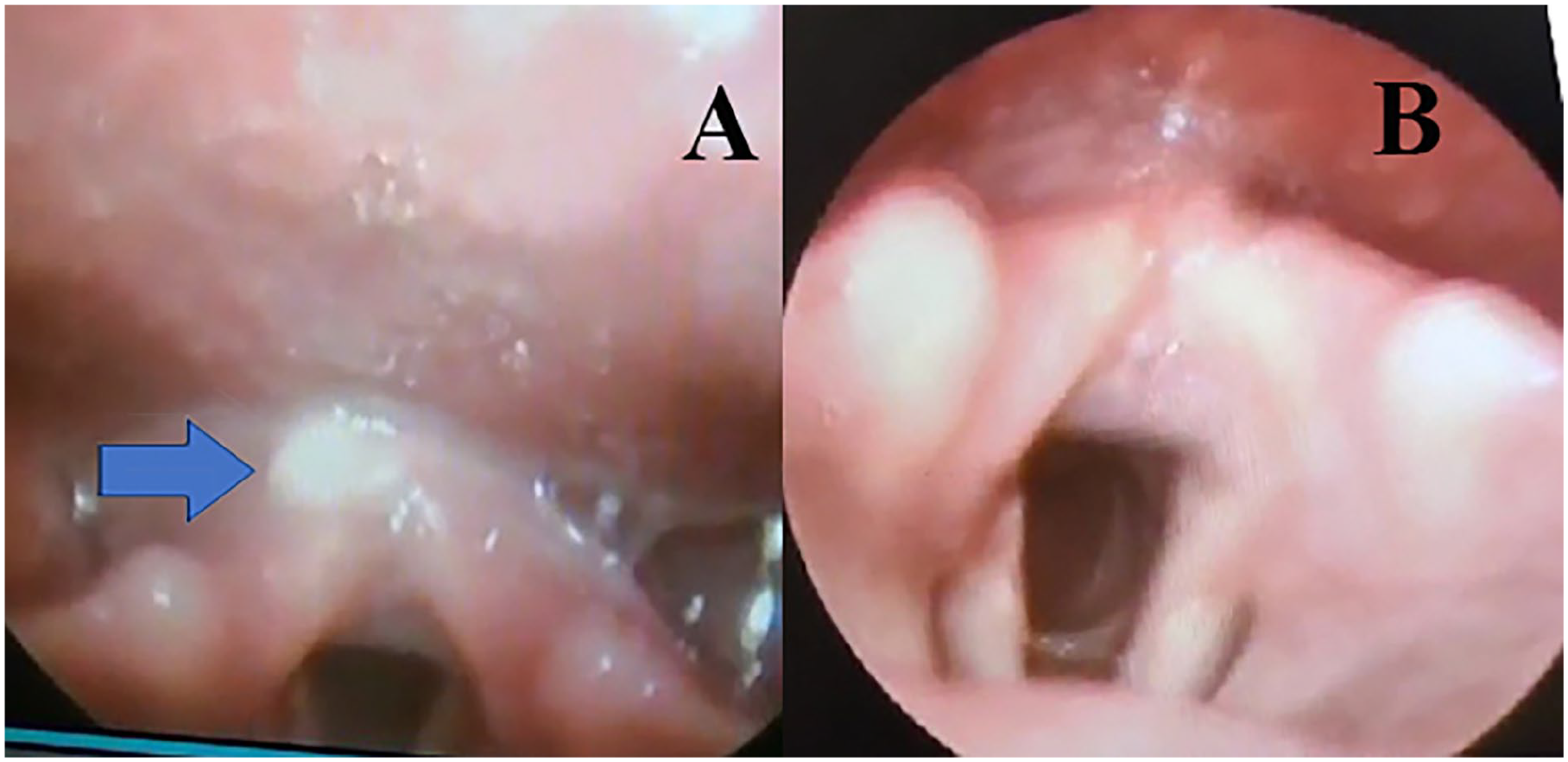
(A) Figure with arrowhead shows one small white nodule seen in the interarytenoid region. (B) Figure with video laryngoscopy after micro laryngeal surgery and excision.
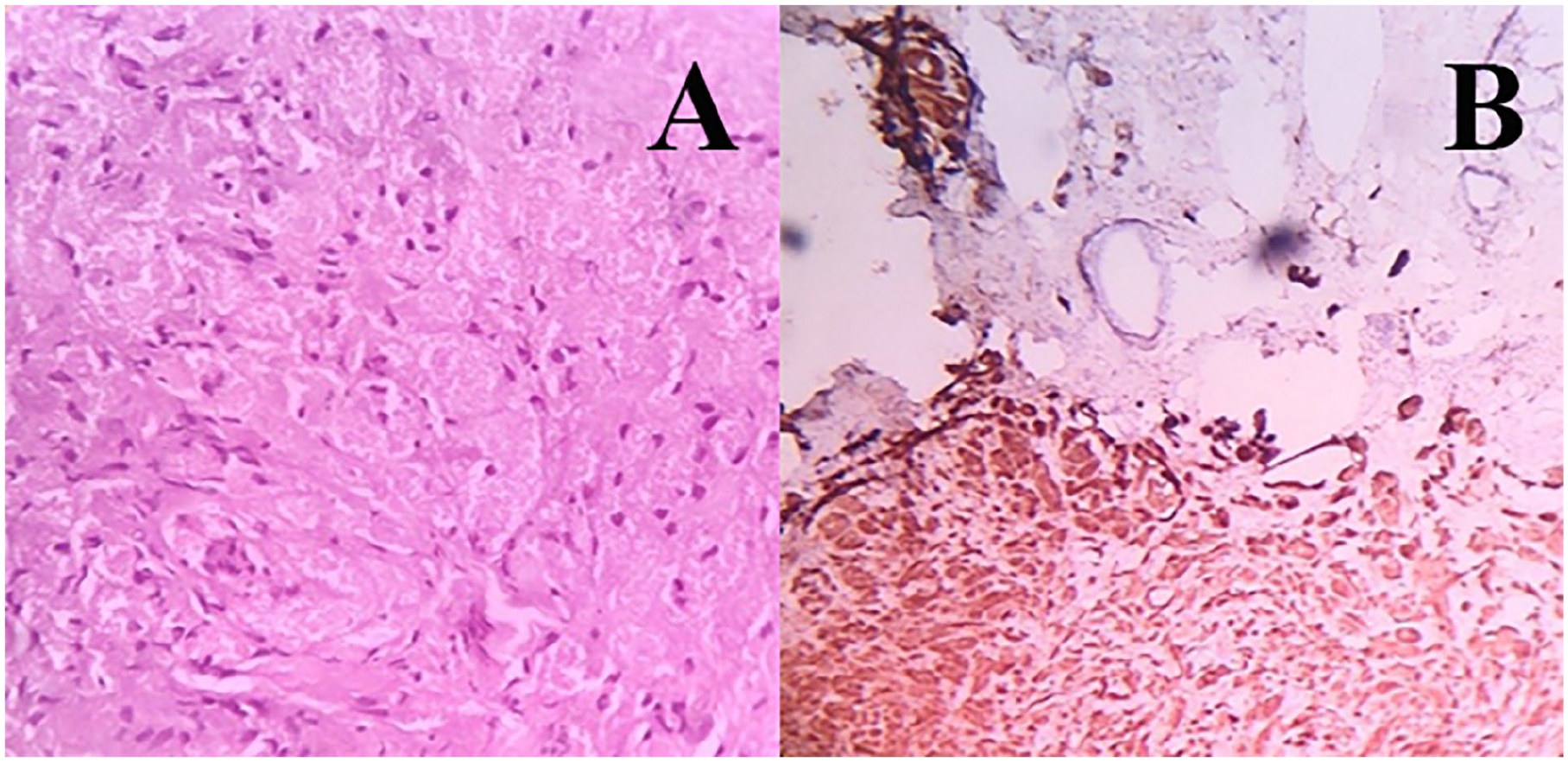
(A) Histopathological reported as sections show polypoidal fragment with hyperplastic stratified squamous epithelium lining—suggestive of granular cell tumor. (B) Immunohistochemistry: S-100 cytoplasmic positive in tumor cells (100%) intensity strong.
The patient is asymptomatic with no evidence of recurrence to date.
Discussion
In 1926, Abrikossoff introduced the term “myoblastic myoma” to describe granular cell tumors (GCTs) based on their perceived differentiation from skeletal muscle. 6 Despite controversy over their origin, immunohistochemistry demonstrates positivity for the S-100 protein and neuron-specific enolase, supporting Schwann cell theory. Electron microscopy reveals clusters of squamous cells with basement membranes similar to perineurium, dehydrated axons, and angulated bodies,7-9 further supporting Schwann cell origin.
Laryngeal GCTs present as small, rounded, firm submucous tumors, often mimicking vocal fold polyps or granulomas. They are typically small (less than 2 cm) and well-circumscribed but non-encapsulated. 10 Predominantly found in the posterior third of the true vocal cords, they may also occur in various laryngeal regions. Differentiating them from polyps involves considering their fibrotic nature and larger size.
While CT and MRI features are generally regarded as nonspecific for diagnosing granular cell tumors, they remain viable options for preoperative diagnosis of GCTs in the head and neck region. On T1-weighted MRI scans, GCTs typically appear slightly hypointense and show homogeneous contrast enhancement. Conversely, T2-weighted MRI images exhibit a heterogeneously increased signal. CT scans usually reveal these lesions as solid masses with relatively homogeneous enhancement, resembling squamous cell carcinoma. 6 Diagnosis is confirmed through histological examination, as endoscopic biopsies limited to the mucosa may result in misdiagnosis. The cytoplasm of GCTs contains ill-defined spindle-shaped or polygonal vacuolated nuclei and eosinophilic granules. 1 These granules stain positively for PAS, S-100 protein, neuron-specific enolase, vimentin, myelin-associated glycoprotein (Leu-7), and CD 68 (KP-1).
Malignant GCTs are rare (1%-2% of cases) 4 and are suspected in cases with nuclear pleomorphism, frequent mitoses, increased nucleus/cytoplasm ratio, spindle-shaped cellularity, necrosis, and large nucleoli. Clinically, suspicion arises with tumor size ≥4 cm, rapid growth, recurrence, or infiltration into adjacent tissue.
Treatment for benign GCTs involves complete surgical resection, aiming for a negative free margin. Frozen biopsy confirmation is recommended during surgery. Radiation or chemotherapy is not recommended due to limited responsiveness and potential malignant transformation. 1 Despite proper resection, an 8% to 21% recurrence rate exists, often at the primary site, possibly due to diagnostic failures or inadequate removal. 11
Conclusion
Although laryngeal GCTs are rare and typically benign, accurate diagnosis and appropriate follow-up are crucial. Regular long-term follow-ups, including fiber optic laryngoscopy, are necessary to confirm recurrence. This case emphasizes the importance of awareness, accurate diagnosis, and timely treatment for laryngeal GCTs.
Footnotes
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval is not required for this study in accordance with local guidelines. The authors declare that appropriate written informed consent was obtained from the patient for the publication of details of his medical cases and any accompanying images.