
Abstract
Granular cell tumors (GCTs) are rare benign tumors that can occur in any part of the body. They are most commonly found in the head and neck region, especially the tongue. Laryngeal GCTs are rare, accounting for only 3% to 10% of all GCTs. This case report describes a 4-year-old boy with a laryngeal GCT. The patient presented with a history of hoarseness for 2 years. Stroboscopy revealed a large mass occupying the entire length of the left vocal cord. The mass was successfully removed by microlaryngeal surgery with laser ablation. The patient’s symptoms resolved after surgery, and he had an uneventful recovery. This case highlights the importance of considering GCTs in the differential diagnosis of patients with hoarseness. Early diagnosis and treatment can lead to excellent outcomes.
Introduction
Granular cell tumors (GCTs) are extremely uncommon benign tumors, first described by Abriskossoff in 1926, 1 that generally occur between the third and sixth decades of life; they are rarely observed in the pediatric age group. 2 Half of all GCTs are present in the head and neck region, mostly in the tongue. 3 Laryngeal involvement is uncommon, only occurs in 3% to 10% of cases, and commonly seen in the posterior glottis in adults, whereas it is often seen in children in the anterior glottis.4,5 Less common locations of GCTs in the larynx are the anterior commissure, arytenoids, and subglottic region. 6 There has been controversy in the literature about the origin of GCTs, initially named “myoblastoma” by Abriskossoff who believed they originated from skeletal muscle cells. However, advanced immunochemistry suggested a neuroectodermal origin due to the presence of peripheral axons. 7 Malignant transformation of GCTs is very rare, representing only 1% to 2% of cases. 8 Dysphonia and hoarseness are the most common symptoms of GCTs involving the larynx, but cough, dysphagia, and odynophagia can occur. 9 GCTs are well circumscribed, homogenous, and have a gray-yellow appearance. 10 Typically, the epithelium overlying a mass demonstrates pseudoepitheliomatous hyperplasia that mimics squamous cell carcinoma. 11
Case Report
Here, we report the case of a 4-year-old boy who presented to our ENT department with hoarseness. The boy’s parents mentioned that he had been hoarse for approximately 2 years without them seeking medical attention; however, they began to worry after he developed aphonic crying. The patient’s neonatal history was significant for Neonatal Intensive Care Uint (NICU) admission for 20 days after delivery due to bacteremia. He had an unknown history of intubation, and further examination was unremarkable. Stroboscopy showed freely mobile bilateral vocal cords and a large mass occupied the entire length of the left vocal cord. It had a free edge and a partial subglottic origin (Figure 1). The presumptive diagnosis was a large vocal cord cyst with a granular cell mass. Microlaryngeal surgery to excise the mass was scheduled with the parents’ consent.

Preoperative stroboscopic images.
The operation was performed under general anesthesia, and a small, soft, and fragile mass was identified below the left vocal cord, extending to the midline and sparing the anterior commissure. The mass was removed using heart-shaped forceps because of its flexibility; we could not excise it with scissors, so we sent it for histopathological examination. The laser (8 W) was applied to the mass bed at a depth of 1 mm below the left vocal cord and anterior commissure, respectively. Histopathology and immunochemistry confirmed the diagnosis of a GCT (Figure 2). Postoperative follow-up revealed that the patient’s symptoms persisted. Stroboscopy was repeated, and minimal remnants were confirmed under the surface of the anterior third of the left vocal cord and in the right and left subglottic areas. A revision of the microlaryngeal surgery and direct laryngoscopy with complete laser ablation were performed. The patient experienced an uneventful postoperative period.
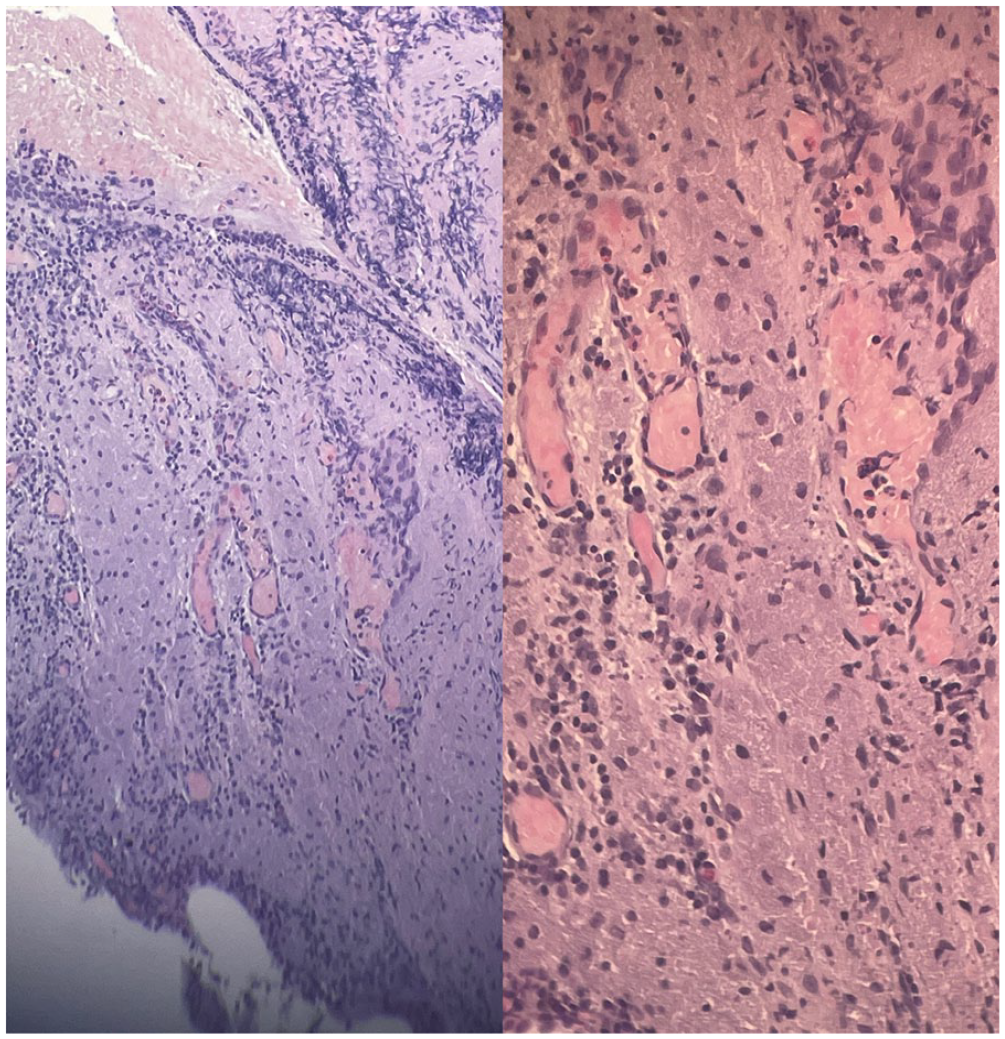
Histopathology slides taken from laryngeal lesions show a feature of moderate to severe pseudopithelimatous hyperplasia that suggests GTC.
Discussion
The first known case of a GCT was reported in 1926 by Abrikossoff. 1 The initial theory suggested that the tumor had a myogenic origin. However, this was eventually ruled out due to its presence in places devoid of myoglobin and muscle fibers. 12 Currently, the origin of tumor cells (Schwann cells) is determined through immunohistochemical studies. 7 GCTs can appear in both adult and pediatric patients. 2 Our review of the literature focused on the treatment of GCTs in men. Although these tumors are generally slow growing, they can develop aggressive characteristics, with distant metastasis observed in 1% to 2% of cases. 8 Although laryngeal GCTs are most commonly associated with hoarseness, globus sensation and dysphagia can also occur. 9 Our case had a similar presentation. Although the size of the tumor was significant, it did not cause obstruction or dyspnea in the larynx, which is not a common location for GCTs. Therefore, dysphonia was not considered as the first diagnosis.
The first differential diagnosis to consider in such cases is benign (but common) lesions of the vocal folds, such as epidermoid cysts and mucous retention exhibiting a white-colored and oval look, as well as polyps of the vocal cords and granulomas, particularly in the posterior endolarynx. In contrast to GCTs, polyps tend to have a gelatinous appearance and are typically associated with vocal abuse. GCTs exhibit a fibrotic appearance. 13
Granuloma development can be triggered by chemical or physical aggression to the larynx. Granulomas resemble the microscopic appearance of GCTs, and this type of tumor has smaller dimensions. 5 They typically appear in the posterior larynx (posterior endolarynx). 13 Recurrent respiratory papilloma should be considered in the differential diagnosis since it is the most common benign laryngeal tumor in childhood. 13
The visual observation of GCTs during laryngoscopy, along with their gradual progression, may potentially result in inadequate surgical intervention due to a lack of thoroughness on the part of surgeons. The cellular characterization of GCTs is characterized by pseudoepitheliomatous hyperplasia, and the presence of sporadic normal mitosis may lead to potential misdiagnosis as squamous cell carcinoma. 11 Nevertheless, the absence of nuclear hyperplasia or pleomorphism and the presence of granular cells can aid in distinguishing between these diseases. 14
Histological examination of surgical specimens is also relevant for the treatment of this type of tumor. Treatment involves resection with a complete margin to decrease the risk of recurrence. 5 A granuloma return occurs in 2% to 8% of patients with free borders. When the borders are affected, the risk of a recurrence amounts to 21% to 50%. 15 In the present case, the tumor was resected using a transoral CO2 laser. Despite the positive outcome, follow-up assessments are recommended to check for possible recurrence and malignant transformation. 2 Following the patient for an extended period is recommended, as is having an endoscopic examination performed at least once per year considering that GCT grows slowly and takes around 6 to 7 months to become symptomatic. 16 Routine follow-up examinations are conducted at the King Abdulaziz University Hospital in Riyadh, involving the utilization of outpatient fiberoptic laryngoscopy for a period of up to 6 months post-surgery. The purpose of these examinations is to verify the presence of any remaining or recurring GCTs. While the occurrence of GCTs in the vocal cords is few, it is crucial for otolaryngologist to acquire knowledge about this specific type of tumors and be knowledgeable about the many therapeutic approaches available for managing these individuals.
Conclusion
GCTs of the larynx are rare and distinct. They can be considered as differential diagnoses for adult males with persistent dysphonia. A thorough evaluation combined with comprehensive surgical resection can significantly enhance vocal function and prevent future recurrence. Endoscopic carbon dioxide laser excision is an effective and minimally invasive surgical technique that can help preserve vocal cord function and quality of life. It is necessary to conduct additional research on GCTs of the vocal cords to increase our understanding of this rare entity and its management.
Footnotes
Data Availability
Data in this article were obtained from King Abdulaziz University Hospital registry in Riyadh, Saudi Arabia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent/Patient Consent
Informed consent for patient information to be published in this article was not obtained because no personal or identifiable information/images were submitted in this article.