
Abstract
Parathyroid carcinoma (PC) is a rare endocrine malignancy. We report 6 cases of PCs operated on in our department, during a period of 12 years (2010-2021). All of our patients presented severe hyperparathyroidism, high calcium levels, and very elevated parathormone (PTH) rates. Five were between the fifth and sixth decades of life and 1 patient was 37 years old. The parathyroid gland was only palpable in 1 case. All of our patients underwent cervical ultrasound and 5 of them underwent 99m Tc-MIBI scintigraphy. One of the patients presented bilateral parathyroid masses. All our patients were treated surgically: a parathyroidectomy was performed in all cases. In 1 patient, parathyroidectomy was performed in conjunction with a homolateral loboisthmectomy, as the diagnosis of PC was suspected preoperatively due to pulmonary metastases. The final anatomopathological study revealed PC in all cases. Follow-up was uneventful in 5 cases and 1 patient was lost to follow-up. Clinicians should suspect PC in patients with severe hypercalcemia, extremely elevated PTH levels, large parathyroid lesions, and distant metastases. Complete surgical resection, extended to the homolateral thyroid lobe, remains the recommended treatment.
Introduction
Parathyroid carcinoma (PC) is responsible for less than 1% of all cases of primary hyperparathyroidism. Its cause is often unknown, but it can be due to genetic syndromes. The presentation is often made of marked symptoms of primary hyperparathyroidism rather than signs of tumor expansion itself. The difficulty facing every clinician is the fact that the diagnosis of PC is made only during the final anatomopathological study since it is based on the identification of capsular, vascular, or perineural invasion by the tumor. Diagnosis is rarely suspected prior to surgery. Distinguishing this rare tumor from common parathyroid adenomas remains a dilemma. The reference treatment is surgery. 1 The prognosis is improved by early detection and surgical resection of the tumor. 2
The purpose of our paper is to investigate the diagnostic criteria of PCs as well as their therapeutic management modalities through a report of 6 cases of PCs operated on in our department.
Case Series
The mean age at discovery was 61.5 years, with extremes of 37 and 69 years (Table 1). We noted a male predominance with a sex ratio of 2/1. Smoking and severe chronic renal failure were found in each case.
Presentation of Our Patients.
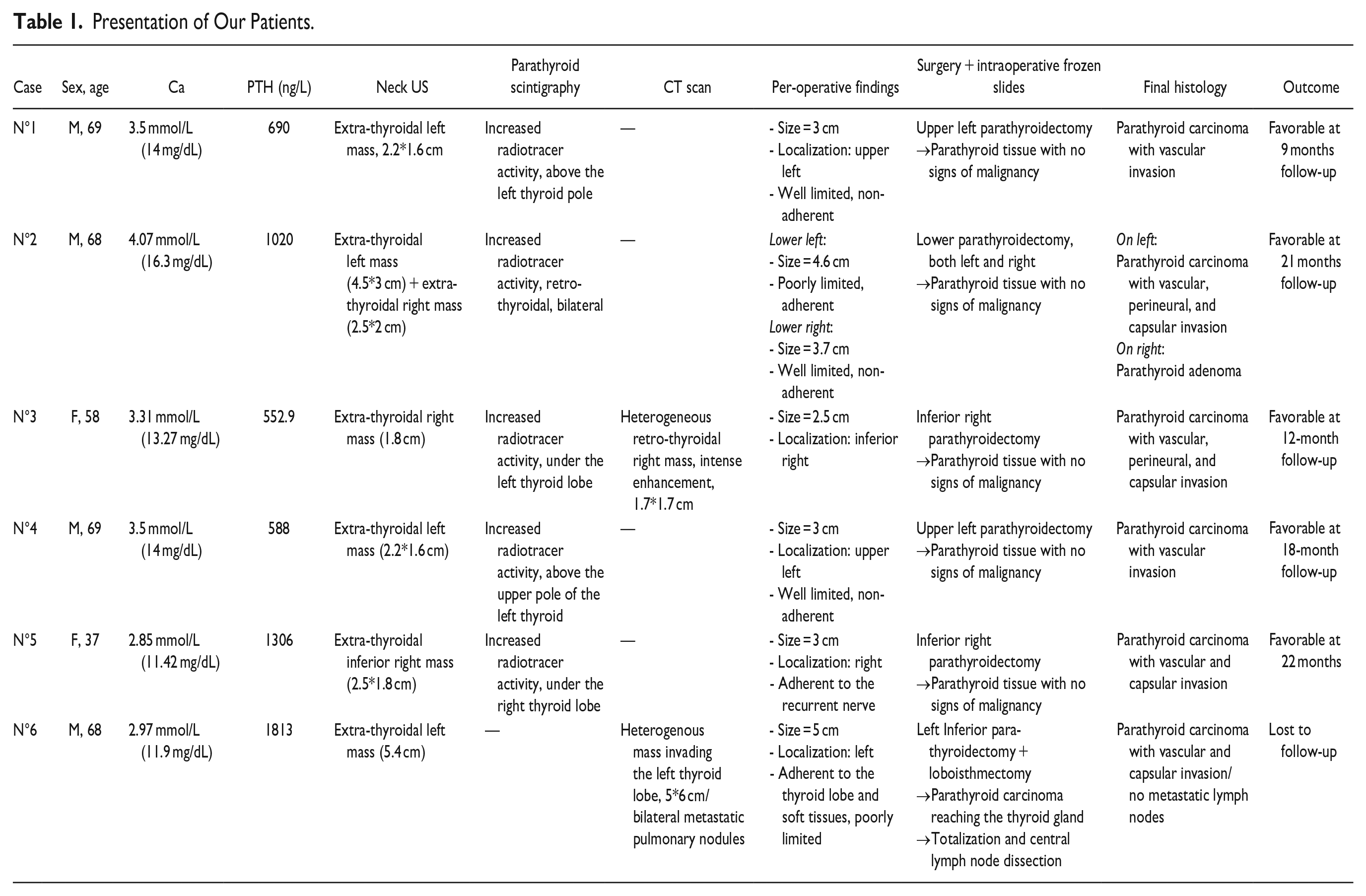
The discovery circumstances were chronic diffuse bone pain in 4 cases—2 of whom had pathological fractures—difficulty walking (steppage) in 1 case, and cervical swelling in another case. The mean delay between the onset of symptoms and consultation was 12 months (3-24 months).
Physical examination was normal in 5 cases. A neck examination revealed fixed anterior cervical swelling in 1 case, measuring 5 cm and lateralized to the left. Laboratory tests showed hypercalcemia in all cases, with a mean value of 3.37 mmol/L and parathormone (PTH) levels more than 10 times higher than the reference values. The diagnosis of primary hyperparathyroidism was retained in all patients.
Cervical ultrasound (cUS) revealed a heterogeneous hypoechoic extra-thyroidal mass in all cases, retrothyroid in 4 cases, and polar inferior in 2 cases. Bilateral masses were found in 1 case. A preoperative Tc-99m Sestamibi scintigraphy, performed in 5 cases, showed a marked increase in peri-thyroid radiotracer activity that was bilateral in 1 case. CT scan was indicated in 2 patients: in case n°3, it was carried out considering the discordance of mass location between ultrasound and scintigraphy, and in case n°6, it was carried out to explore the fixed cervical mass (Table 1). In this case, the parathyroid mass contained microcalcifications, invaded the thyroid lobe, and was associated with 15 bilateral pulmonary nodules, with metastatic appearance (Figure 1). The same patient underwent a bone scintigraphy that revealed multiple brown tumors.
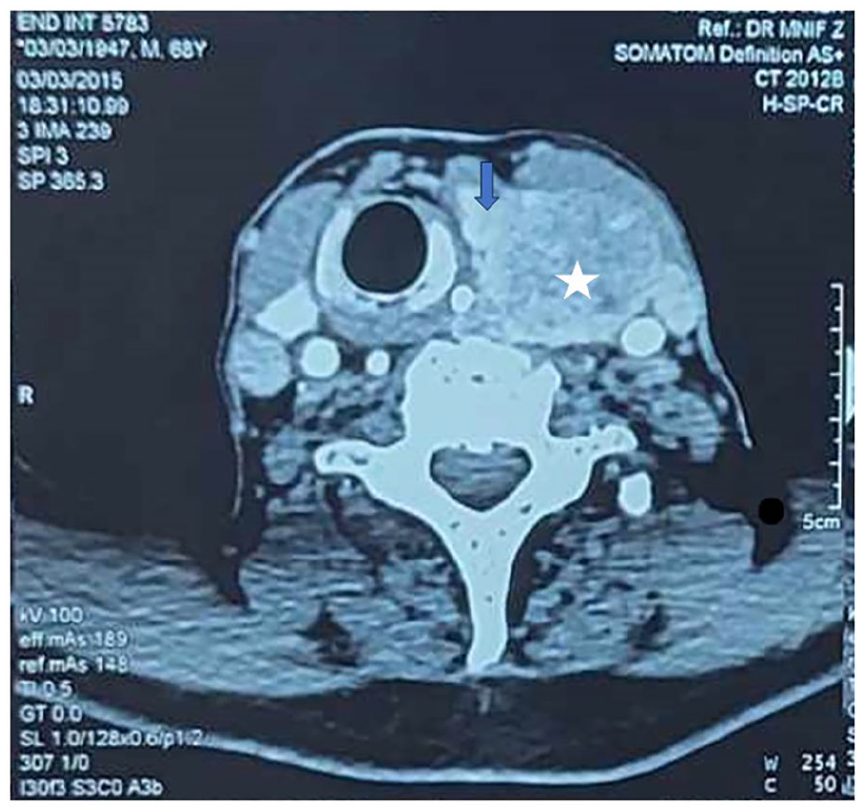
Cervical CT showing on the axial image: a heterogeneous voluminous left mass (white star), invading the homolateral thyroid lobe (Blue arrow).
All patients were operated on. During surgery, the pathological parathyroid gland was adherent in 3 cases and poorly limited in 2 cases. Its median size was 3.5 cm. Five patients underwent a parathyroidectomy with the presence of parathyroid tissue with no signs of malignancy on the intraoperative frozen section. Parathyroidectomy was bilateral in the case n°2 since the patient presented bilateral parathyroid masses. The patient n°6 underwent an inferior left parathyroidectomy and a loboisthmectomy, removing the thyroid lobe and the parathyroid gland in the monobloc. Intraoperative frozen slides revealed a PC of the parathyroid gland, reaching the thyroid without infiltrating it. During the same surgery, a totalization of the thyroidectomy and a dissection of the left central lymph nodes were performed.
The final anatomopathological examination concluded that there was PC in all cases, with signs of vascular invasion in all cases—associated with signs of capsular invasion in 2 cases, to signs of capsular and perineural invasion in 2 cases and with no other signs of local invasion in 2 cases. None of the patients had a second surgery. As for the patient with bilateral parathyroid masses (case n°2), the diagnosis was PC on 1 side and parathyroid adenoma on the contralateral side.
The metastasis scan was performed in 5 patients, using a cervico-thoraco-abdominal CT scan and bone scintigraphy. Only patient n°6 had signs of distant metastases. Calcium and PTH levels returned to normal in all cases, including the metastatic patient. The outcome was favorable in 5 patients with a mean follow-up of 16.4 months, while patient n° 6 was lost to follow-up. No local recurrences or new distant metastases were reported.
Discussion
Our series of cases has the advantage of being complete and contains all necessary clinical and paraclinical examinations. Its drawbacks are the retrospective study and the limited number of patients, but this is only due to the rarity of this entity. PC is one of the most rare malignancies, with a prevalence of 0.005% of all cancers.2,3 It is also a rare cause of primary hyperthyroidism, accounting for less than 1% of its etiologies.4,5 PC usually manifests between the fifth and sixth decades of life.3,5 Only one of our patients had an unusually young age of 37 years. Most authors agreed that the incidence of PC is equal between genders3,5 but some reported a slightly higher incidence in males. 2 No differences in incidence distribution between race and geographic regions were observed, except for Japan, as it is known to have a higher incidence of PC in 5% of all primary hyperparathyroidism cases. 6
PC typically occurs in a sporadic pattern; however, secondary and tertiary hyperparathyroidism, as well as previous radiation exposure, are considered risk factors. 3 Some rare cases of PC associated with genetic syndromes have been reported in the literature, such as hyperthyroidism jaw tumor syndrome, isolated familial hyperparathyroidism, and multiple endocrine neoplasia type 1 and 2.2,3,5
The clinical presentation is most commonly that of primary hyperparathyroidism, with general symptoms (asthenia, weight loss, polydipsia, and polyuria), bone pain or disease (osteoporosis mainly, osteofibrosis or fibrosis fibrosa cystica), muscle fatiguability, or renal disease (renal lithiasis, nephrocalcinosis, etc.). 3 But PC can rarely be nonfunctional in less than 10% of all parathyroid carcinomas. 7 In these cases, the revealing symptoms can be cervical swelling or mass-effect symptoms (dysphagia, dyspnea, or dysphonia). 8
The association of cUS and 99m Tc-MIBI scintigraphy is the most frequently used preoperative imaging study. On cUS, PC usually presents as a hypoechoic lobulated parathyroid gland, typically larger than 3 cm, with poorly defined margins and a rich vascularization. 3 cUS is also useful in the detection of associated thyroid nodules to indicate adequate surgery. 4 Whenever the diagnosis of PC is suspected, fine-needle aspiration should be avoided considering the risk of the spread of malignant cells along the needle track, with no ability to distinguish malignant from benign parathyroid lesions on cytology.3,4,9,10 It is only useful in specific cases with inconclusive scintigraphy or atypical cUS findings. 4
The European Association of Nuclear Medicine recommends implementing dual-phase imaging, combining 99m Tc-MIBI SPECT with a CT scan: the latter allows to location of the hyperfunctioning gland, evaluate its locoregional extensions, and orientate the surgeon.4,11 Some authors suggest the use of 18F-labeled choline analogs as an alternative marker for patients with standard imaging results equivocal or negative standard imaging results.12,13 It is also useful in the detection of minimally invasive parathyroid carcinomas, as well as local and distant recurrences after surgery. 14 18F-FDG positron emission tomography (PET)/CT has been used in literature for locoregional and distant extension studies in the case of poorly differentiated lesions in anatomopathological studies.11,14
In case of preoperative suspicion of PC and the presence of a voluminous parathyroid mass, CT can be performed to assess locoregional and distant extension. 10 CT scan is also useful for recurrent and metastatic cases. 10 MRI is less commonly indicated and is a second-line imaging study. 10
Surgical excision is the cornerstone of the therapeutic management of PC. Today, an “en bloc” resection of the PC and the homolateral thyroid lobe is only recommended if the latter is invaded by the tumor.1,15 Studies comparing a parathyroidectomy with a parathyroidectomy extended to the thyroid lobe did not show significant differences in recurrence rates and overall survival, as long as the tumor capsule was intact during surgery.1,15 These findings are in agreement with our findings since 83% of our patients had a parathyroidectomy without associated loboisthmectomy or lymph node dissection, with no recurrences at follow-up. In addition, in most cases, the diagnosis of PC is not made prior to or during the surgery.2,3,5,9,16 In fact, the only pathognomonic features of PC in histology are capsular, vascular of perineural invasion, only identifiable on the final anatomopathological exam.3,17 The 2022 World Health Organization classification of endocrine and neuroendocrine tumors stated the loss of parafibromin expression on immunohistochemistry, a marker of a CDC73 mutation, as associated with a malignant potential. 18 But it does not represent a definite criterion for malignancy and must correlated to clinical and histological factors. 18
A central compartment lymph node dissection should be performed in case of suspected nodal involvement. 19 In metastatic cases, metastatectomy is recommended whenever technically possible, offering better control of the calcium blood levels and hence an improvement of the overall survival. Even if a complete resection of the metastases is not achievable, a reduction surgery is to be discussed.2,20
Studies did not show benefits in adjuvant chemotherapy or radiation therapy, as no significant improvement in survival rates was noted.16,21,22 The use of immunotherapy for advanced and refractory PC has also been reported, showing tumor size regression and normalization of calcemic and PTH rates. 23
Postoperative surveillance is recommended considering the risk of local recurrence primarily and distant metastasis secondarily. 2 Serum levels of calcium and PTH are normalized after complete surgery, and each elevation of those levels should indicate an imaging examination (cUS, MRI, 99m Tc-MIBI SPECT/CT) or PET scan. 3 Mortality is much more frequently caused by hypercalcemia complications and not by the tumor itself.2,22 Studies showed that tumor resection, complete or partial, improved survival rates compared to the non-operated patients.2,16 The 5-year survival rates are between 80% and 90%. 3 But a poorer prognosis and a decreased cancer-specific survival were observed for tumors larger than 4 cm, older patients (>40 years), metastatic cases at diagnosis, and poorly differentiated tumors.2,3 The prognosis was good for our patients, with a normalization of biochemical parameters and an uneventful follow-up.
The diagnostic challenge of PCs is based on their clinical, radiological, and frozen section resemblance to parathyroid adenomas.2,22 Many studies tried to identify clinical and paraclinical signs evocative of malignancy when managing a patient with primary hyperparathyroidism. Age is controversial in literature: some studies report that patients with PC are relatively younger compared to those with benign lesions, 22 whereas others report higher age as suggestive of malignancy.2,9 Physical examination reveals a palpable neck mass in up to 75% of cases in PC versus only 5% in the case of parathyroid adenoma: This sign should alert the physician about the malignant origin of the parathyroid lesion. Lymph node metastasis can also be found in 15% to 30% of cases. 24
Significantly higher serum levels of parathyroid hormone (3-15 times normal values) and calcium (>3.5 mmol/L) were also found in patients with PC.3,9,11,22 However, no biological analysis can accurately differentiate malignant from benign parathyroid masses. 22 On ultrasound, tumors larger than 3 cm, irregular borders of the mass, decreased and heterogeneous echogenicity, or invasion of adjacent tissue are signs in favor of the malignant nature of the parathyroid mass.3,22 The presence of metastases at presentation can also orient the diagnosis: The most frequent sites are lungs, liver, and bone.2,3,22 A prospective study of quantitative analysis of parathyroid scintigraphy concluded that the standardized uptake value (SUV) of each parathyroid lesion was correlated with its final anatomopathological study and can classify lesions as adenomas, carcinoma, and hyperplasia. 25 In fact, PC has higher retention levels of the 99m-MIBI tracer than benign lesions, which helps eliminate its differential diagnosis preoperatively. 26
Conclusions
Clinicians must always keep this rare entity in mind and suspect it in the event of profound hypercalcemia, very elevated PTH levels, and a palpable tumor. The prognosis is excellent in the event of early treatment and complete surgical removal of the tumor.
Footnotes
Author Contribution
All the authors have participated in the production of this manuscript.
Data Availability Statement
The data are available from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.