
Abstract
Awake tracheostomy is rare in the pediatric population. We describe the case of a 10-year-old male who underwent awake tracheostomy due to airway obstruction from an oropharyngeal rhabdomyosarcoma. Given the varying medical understanding and communication skills in children, advanced planning and interdisciplinary collaboration are essential to keep the patient calm and safe during awake tracheostomy.
Introduction
Awake tracheostomy is an established method of securing a patient’s airway when alternative means, such as orotracheal intubation, are unfeasible. The most common indication in the adult patient is an obstructive aerodigestive malignancy. 1 The patient is kept conscious and spontaneously ventilating to prevent airway compromise during tracheostomy creation. Awake tracheostomy is commonly described in the adult literature, but there are only 2 published case reports of pediatric awake tracheostomy. We present the case of a 10-year-old male who underwent awake tracheostomy due to airway compromise from a large obstructive oropharyngeal rhabdomyosarcoma.
Case Report
We present a 10-year-old male with a history of biliary atresia and liver transplantation at 7 months of age necessitating lifelong immunosuppression with Tacrolimus. The patient had been complaining of throat pain and underwent multiple antibiotic courses at an outside hospital for presumed peritonsillar abscess for approximately 1 month. The patient presented to our pediatric emergency department with chief complaint of throat pain, food intolerance, muffled voice, drooling, and dyspnea. On exam, he was found to have complete occlusion of the oropharynx with a large soft tissue mass (Figure 1A). Bedside flexible nasopharyngoscopy revealed complete obstruction of the oropharyngeal airway with inability to pass the laryngoscope beyond the oropharynx or visualize the larynx.
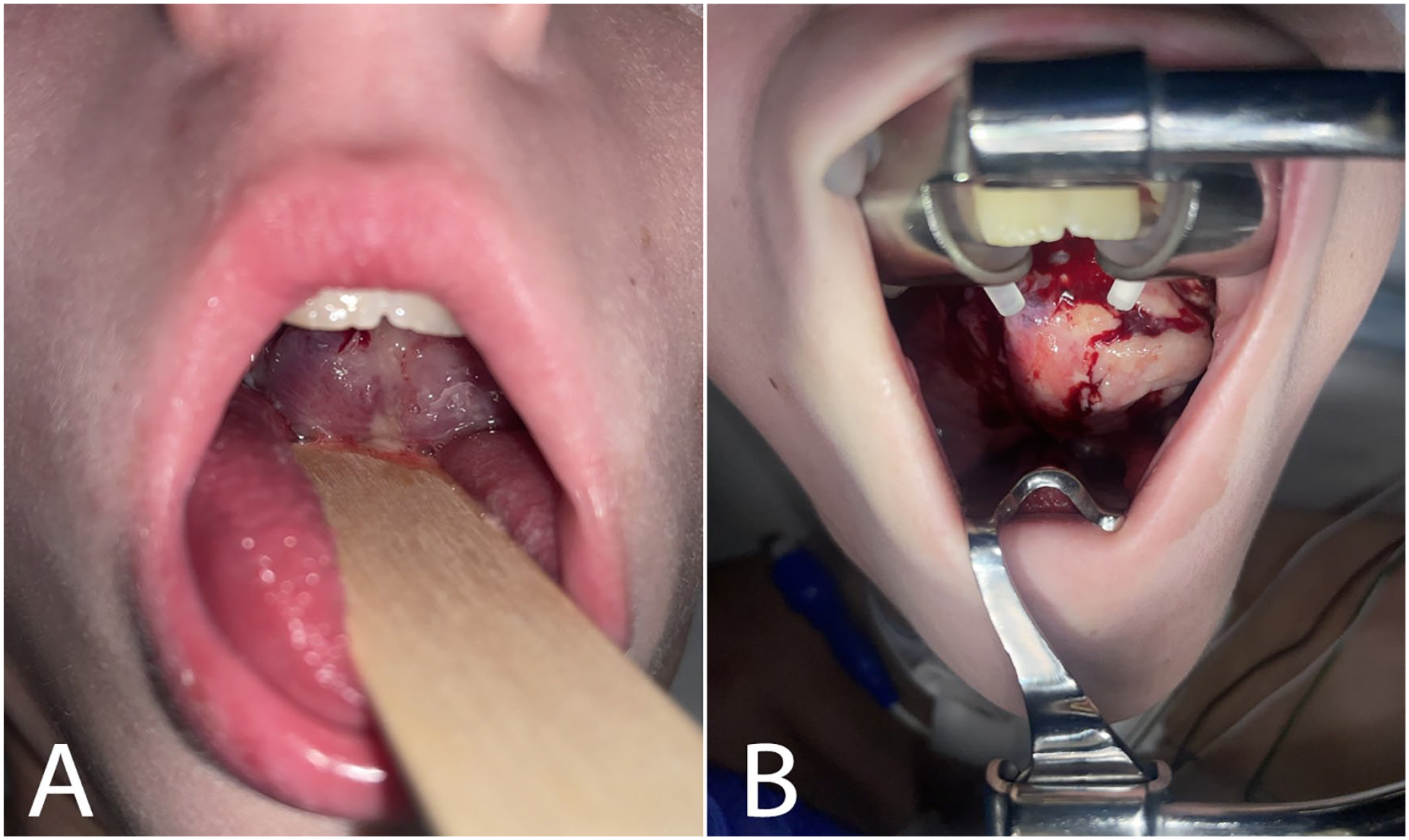
Oropharyngeal mass visible on arrival (A) and with Crowe-Davis retractor in place during oropharyngeal biopsy (B).
A contrast-enhanced computed tomographic scan of the neck demonstrated a large heterogeneously enhancing soft tissue mass in the left oropharynx measuring approximately 6.5 × 5.7 × 6.4 cm with involvement of the nasopharynx and left parapharyngeal space (Figure 2A-F).
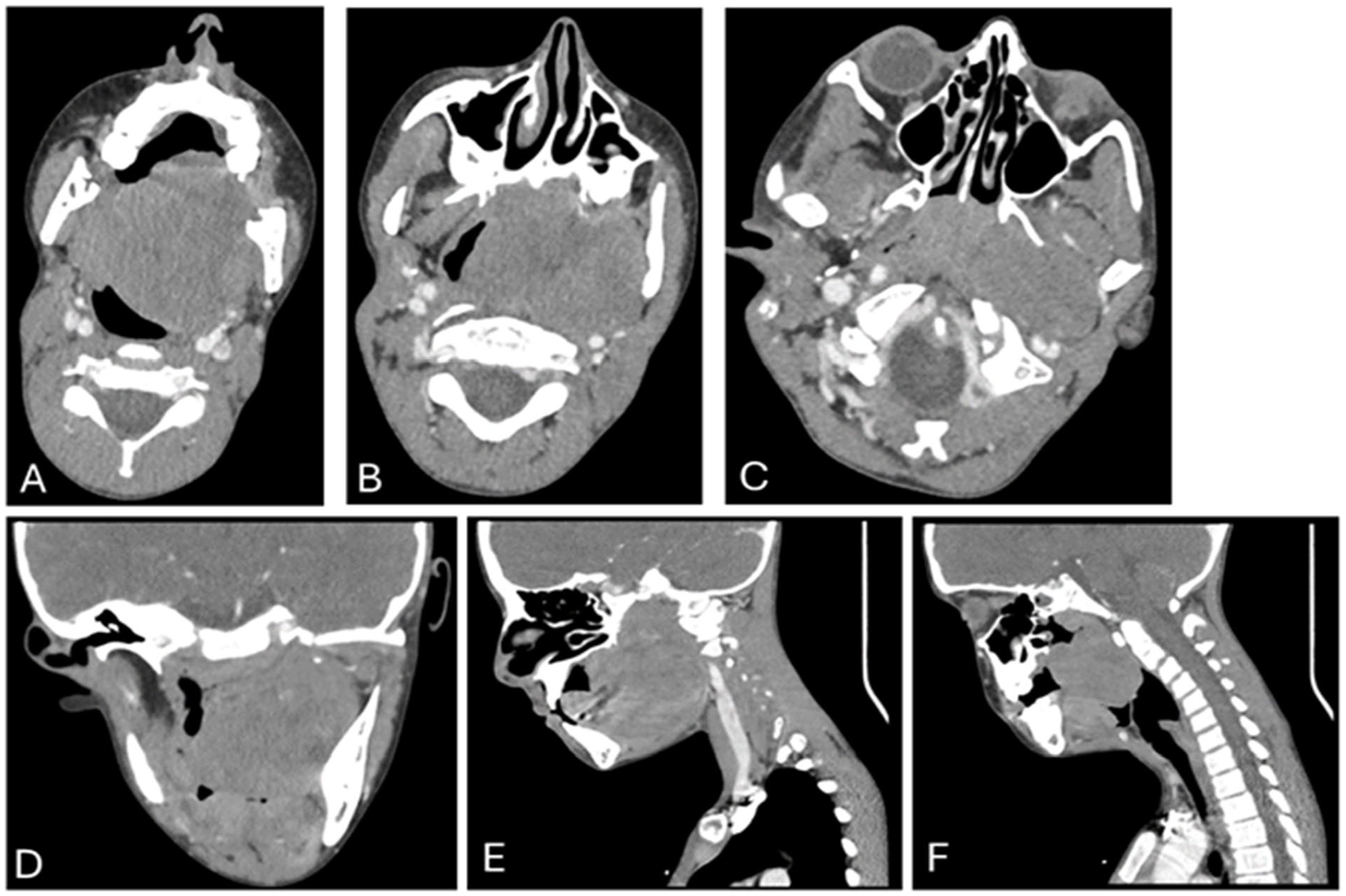
Contrast-enhanced CT neck demonstrating a large left oropharyngeal mass with parapharyngeal and nasopharyngeal extension. Axial (A-C), coronal (D), and sagittal (E, F) series are displayed. CT, computed tomography.
Given the extent of airway obstruction, it was determined that endotracheal intubation prior to tracheostomy would not be possible. We discussed awake tracheostomy with the patient’s legal guardian and the anesthesiology team. The patient was taken to the operating room. The anesthesia team administered a 1-mcg/kg intravenous bolus of dexmedetomidine to achieve conscious sedation with spontaneous ventilation. The neck was marked and injected with lidocaine/epinephrine mixture. Upon injection of local anesthetic, the patient began to become agitated. Low-dose inhalational anesthetic (sevoflurane) was started, after which the patient began to have upper airway obstruction and desaturation.
The neck was quickly prepared with betadine, and emergent tracheostomy was performed in the usual fashion. Due to the emergent nature of the procedure, draping was not possible (Figure 3). The neck skin was incised with a vertical 1.5-cm incision, cervical strap muscles were split in the midline, and the trachea was identified, skeletonized, and incised vertically at rings 2 and 3. The stoma was matured with chromic catgut suture, and non-absorbable retention sutures were placed alongside the tracheotomy and taped to the chest. Upon tracheostomy tube insertion, general anesthesia was induced with a combination of propofol, morphine, and sevoflurane. After the tracheostomy procedure was completed, a Crowe-Davis mouth gag was inserted, and the patient underwent oropharyngeal biopsy with cup forceps (Figure 1B). The patient tolerated the procedure well.

Intraoperative photographs during awake tracheostomy.
Final pathologic analysis revealed an oropharyngeal sclerosing rhabdomyosarcoma with a MYOD1 mutation. The patient eventually underwent neoadjuvant chemotherapy, tumor excision with neck dissection, and postoperative chemoradiation. The patient’s cancer is in remission, and he is doing well 9 months after tracheostomy placement. Eventual decannulation is planned after obtaining a capped sleep study.
Discussion
Upper aerodigestive malignancy, the most common indication for awake tracheostomy in adults, is rare in the pediatric population. For this reason, pediatric awake tracheostomy is uncommon and only 2 case reports are described in the literature. Ahuja et al described the case of a 10-year-old male with airway compromise secondary to a retropharyngeal abscess. 2 They described premedication with nebulized 4% lidocaine, encouraging the child to position themselves in a comfortable sitting position on the operating room table, and allowing the child’s father to accompany him into the operating room. They also described a resident physician keeping the patient occupied with a cartoon movie displayed on a cellphone and frequent verbal prompting. Yuan et al also described using 2 anesthesiologists and a child-life specialist to keep their 7-year-old patient occupied with dolls, conversation, and a movie displayed on a tablet. 3 Both cases utilized preoxygenation with 100% oxygen and intravenous glycopyrrolate. Yuan et al also anesthetized the neck with topical 4% lidocaine first, followed by sedation with intravenous midazolam (0.05 mg/kg) and intravenous ketamine (0.5 mg/kg) administered slowly over 10 min.
Planning and multidisciplinary teamwork are essential to care for the pediatric patient with a compromised airway. Despite close collaboration with the anesthesia team, the patient in our case began to have acute upper airway obstruction on the operating room table during preparation for surgery. An emergent tracheostomy was performed successfully. The acute airway obstruction in the operating room may have been precipitated by patient agitation after injection of local anesthetic or by initiation of inhalational anesthetic. The size of the oropharyngeal mass may have also played a role in the patient’s agitation and rapid desaturation. The large mass likely led to greater obstruction with supine positioning, ultimately reducing the patient’s tolerance of the procedure. The size of the airway mass and degree of expected obstruction must be considered when planning an awake tracheostomy.
In hindsight, some of the aforementioned strategies may have proven useful to improve the patient’s experience in our report. For example, the patient may have benefited from an intravenous benzodiazepine or a low-dose intravenous anesthetic, rather than an inhalational anesthetic. In addition, positioning the patient more upright and using topical lidocaine cream prior to lidocaine skin injection may have helped. A less intrusive form of positive pressure ventilation, such as high flow nasal cannula, may have also been preferable to the bag-mask ventilation that was used.
Conclusion
Awake tracheostomy is exceedingly rare in the pediatric patient population. We present the case of a child who underwent awake tracheostomy due to an obstructing oropharyngeal rhabdomyosarcoma. Given the potential limitations in understanding and communication in children, additional patient comfort measures should be considered during awake tracheostomy. These can include topical anesthesia, patient distraction with media players or child life specialists, optimal operating room positioning, and appropriately dosed sedatives or anxiolytics. Planning and close collaboration with all involved services (anesthesia, operating room personnel, etc.) is essential to effectively care for these challenging patients.
Footnotes
Acknowledgements
None.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent/Patient Consent
We have obtained informed consent to publish this article from the patient’s legal representative (mother).
Trial Registration Number/Date
Not applicable.
Grant Number
Not applicable.