
Abstract
We describe a case of lymphatic malformation (LM) with snoring as the primary symptom. The patient, an 11-year-old boy, sought medical attention due to “snoring that had worsened over 3 years, accompanied by shortness of breath for 1 month.” The preoperative examination showed that the apnea-hypopnea index during sleep was 33.4. The average overnight blood oxygen saturation was 95.3%, reaching a lowest level of 79.9%. Magnetic resonance imaging identified a space-occupying lesion in the postpharyngeal space, leading to significant compression and narrowing of the pharyngeal cavity. This suggested the possibility of a vascular malformation, with a higher proportion of vascular components. The patient underwent resection of the pharyngeal mass and temporary tracheostomy under general anesthesia, and intraoperative freeze and postoperative pathological diagnoses confirmed LM. Postoperative prognosis was favorable.
Case Report
The patient, an 11-year-old boy, presented to the department of otorhinolaryngology of Shenzhen Children’s Hospital on October 25, 2023, with “snoring that had worsened over more than 3 years, accompanied by shortness of breath for 1 month.” The patient began to experience nasal congestion and snoring without any obvious triggers 3 months before admission, and this was occasionally accompanied by open-mouth breathing. These symptoms had progressively worsened over the previous month and were accompanied by shortness of breath. The patient had been examined as an outpatient 1 week before admission, where a smooth mass was found on the left posterior pharyngeal wall. No other symptoms were experienced, such as coughing, phlegm, dysphagia, foreign body sensation, bleeding, or fever. Further specialist examination indicated slight congestion of the pharyngeal mucosa, with a localized bulge seen on the left side of the posterior pharyngeal wall. The lesion was approximately 3 cm × 5 cm in size, with a smooth surface, and no evidence of rupture or bleeding. Electronic laryngoscopy revealed a mass in the posterior pharynx (Figure 1). Computed tomography (CT) scan of neck showed a space-occupying lesion on the left side of the posterior pharyngeal wall. A plain magnetic resonance imaging (MRI) scan of the neck plus enhancement showed an irregular solid cystic mass, measuring approximately 31 mm × 21 mm × 69 mm, in the left retropharyngeal space around the C2-6 level. The cystic component showed isointensity in T1-weighted image (WI), high intensity in T2WI, with suppression of fat, diffusion restriction in diffusion WI, and slight enhancement and scattered low-intensity patches within it (Figures 2–4). Laboratory tests after admission showed no abnormalities. The clinical diagnosis was a postpharyngeal space mass (left side) accompanied by obstructive sleep apnea-hypopnea syndrome.

Electronic laryngoscopy revealed a mass in the posterior pharynx.
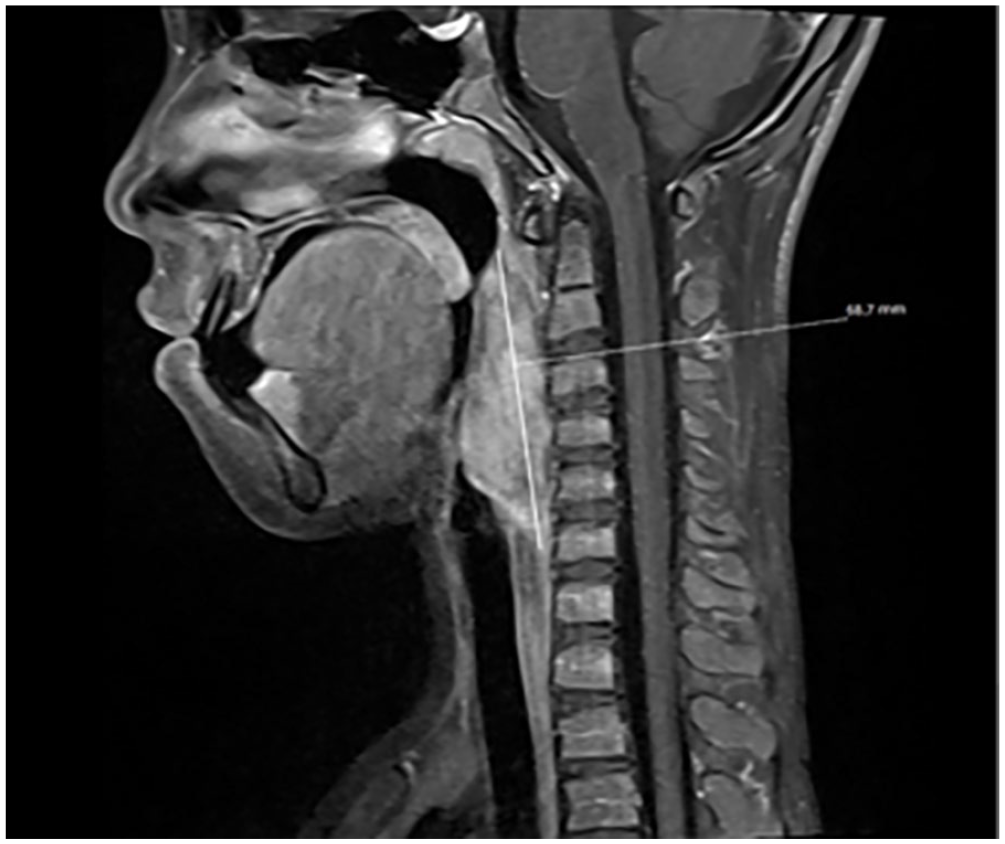
A plain magnetic resonance imaging (MRI) scan of the neck plus enhancement showed an irregular solid cystic mass, measuring approximately 31 × 21 × 69 mm.
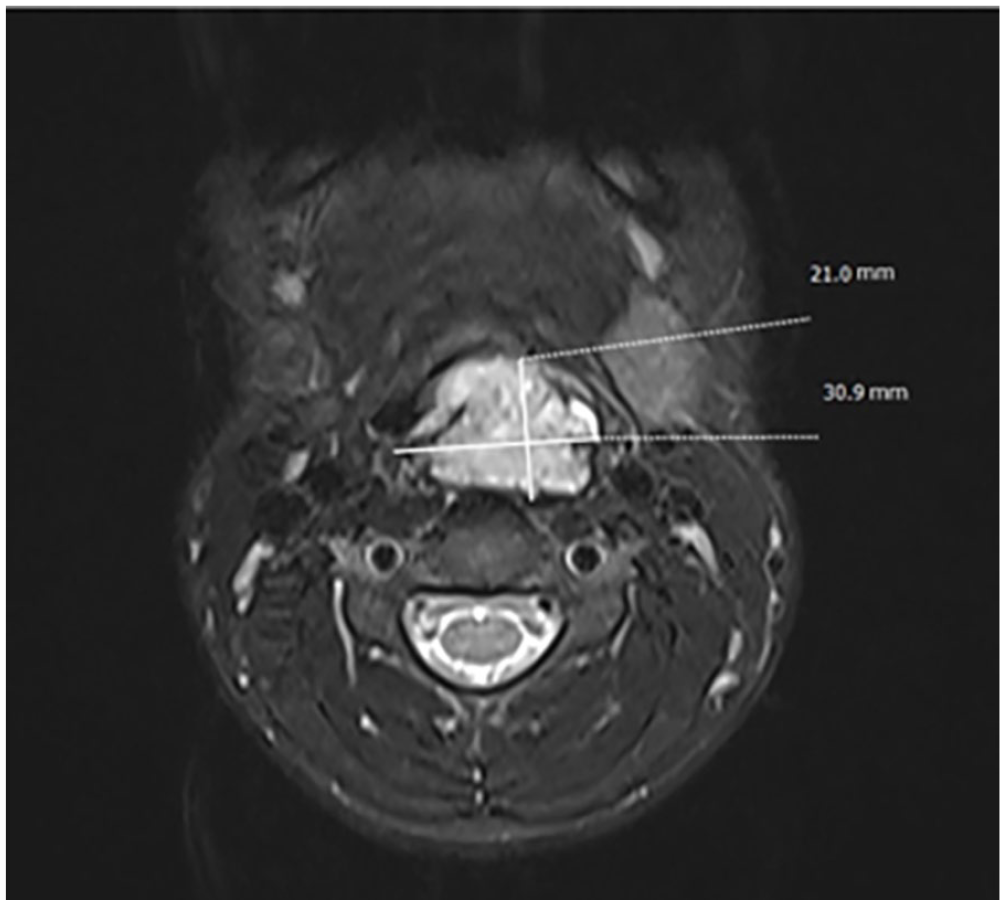
A plain magnetic resonance imaging (MRI) scan of the neck plus enhancement showed an irregular solid cystic mass, measuring approximately 31 × 21 × 69 mm, in the left retropharyngeal space, and high intensity in T2WI.
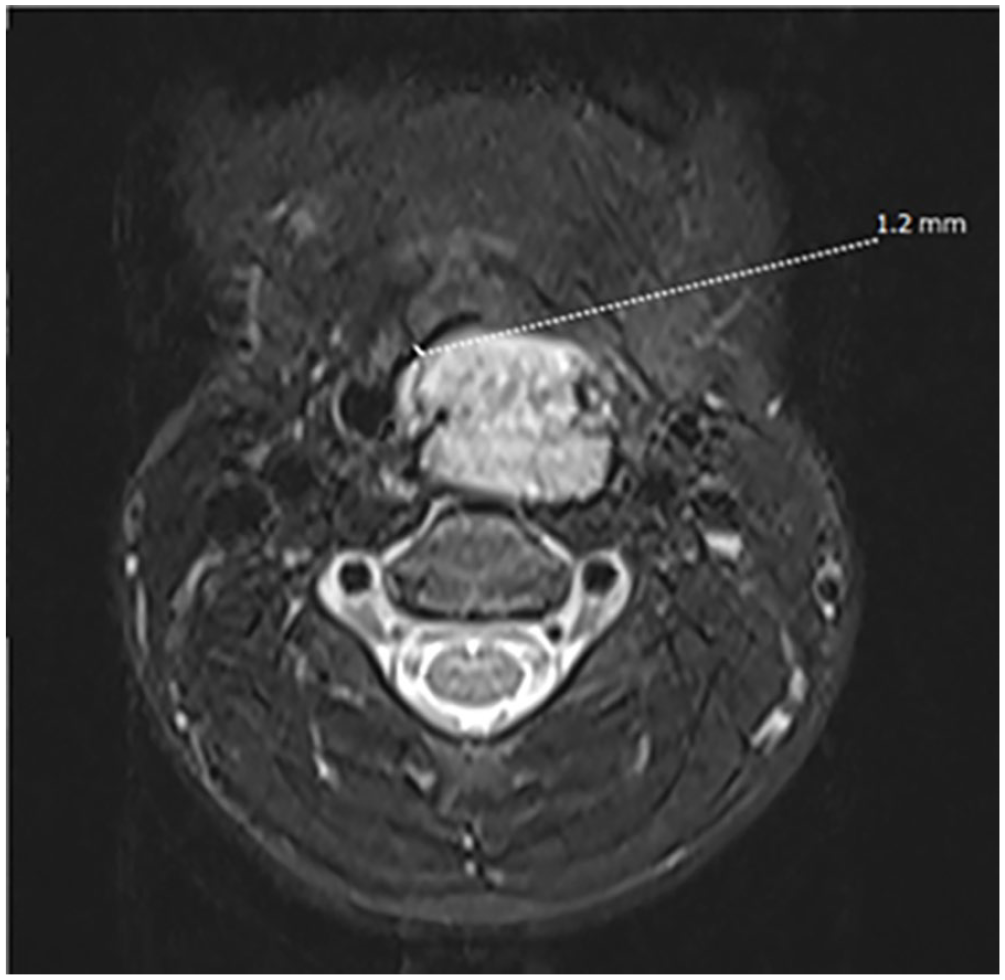
A plain magnetic resonance imaging (MRI) scan of the neck plus enhancement showed an irregular solid cystic mass, measuring approximately 31 × 21 × 69 mm, in the left retropharyngeal space, and high intensity in T2WI.
The patient underwent resection of the pharyngeal mass and temporary tracheostomy under general anesthesia on October 30, 2023. The temporary tracheostomy was performed first to avoid respiratory distress during the operation. The patient was then placed in a supine position with his head hyperextended. After the mouth was opened and the oral cavity was fixed, the mass on the left side of the posterior pharyngeal wall was observed. The pharyngeal wall was incised along the longitudinal axis of the mass to expose it, and a small amount of tissue was excised from the mass for pathological examination of frozen sections. The mass was then separated from the surrounding normal tissues using a stripper, followed by complete excision with an electrosurgical knife. Hemostasis was achieved extensively, and the incision in the posterior pharyngeal wall was sutured with absorbable 4-0 sutures. Routine pathological examination of the tissue confirmed that the mass was a lymphatic malformation (LM; Figures 5 and 6).
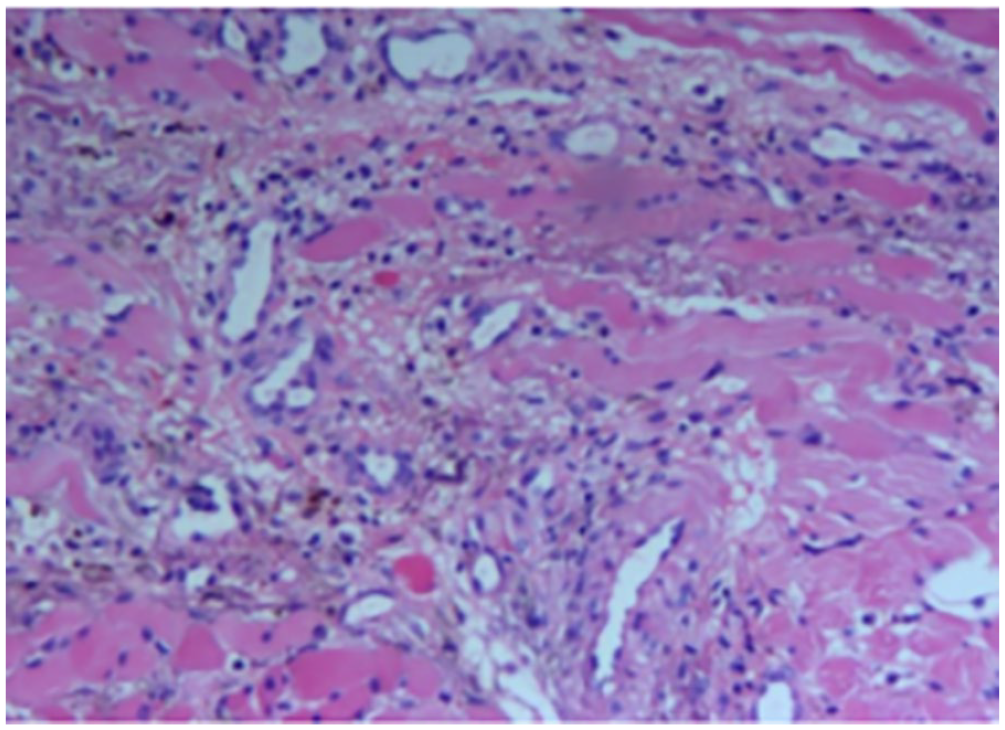
Routine pathological examination showed fiber and striated muscle tissue. Its morphology is consistent with vascular malformation, with expanded vasculature, lymphocyte infiltration and hemosiderin deposition.
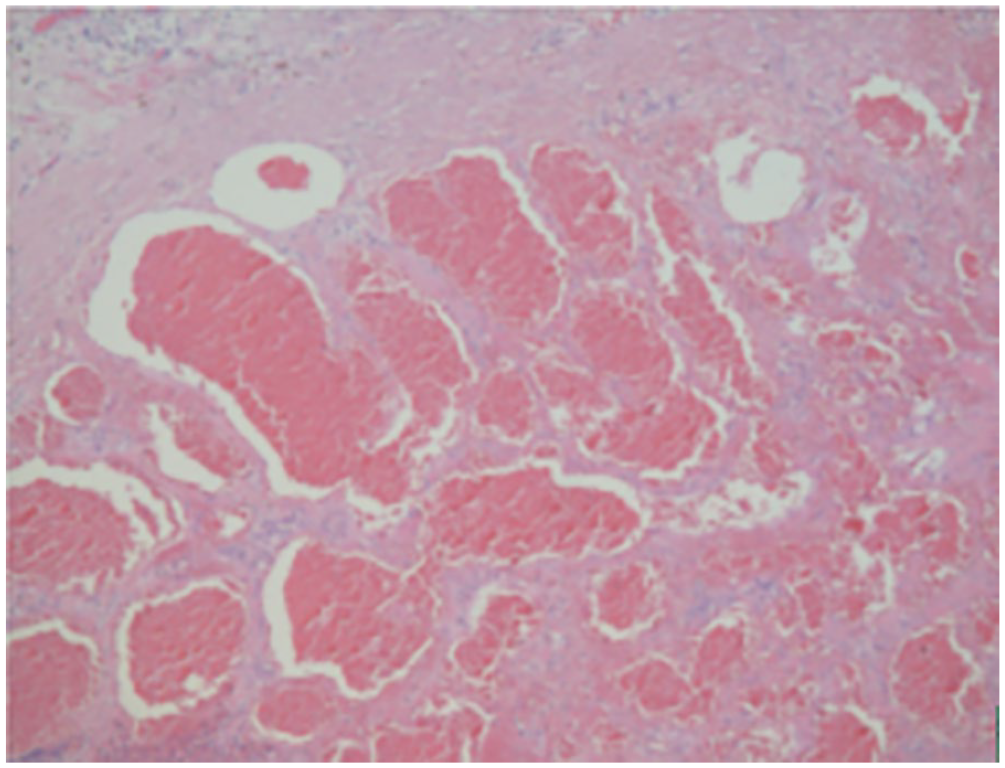
Under light microscope, vascular hyperplasia, star nodules, lumen dilation, partial congestion, tube wall thickness is different, interstitial fibrous tissue hyperplasia, and striated muscle bundle are seen.
Discussion
LMs are developmental abnormalities of the lymphatic vessels and tissues, and represent a common congenital vascular malformation. These malformations, previously known as lymphangiomas, were first reported by Wernher in 1843. 1 In 1995, a new classification proposed by Waner and Suen 2 was accepted by the International Society for the Study of Vascular Anomalies, 3 and the term lymphangioma was replaced with lymphatic malformation. Based on their clinical and histological characteristics, LMs are further classified into microcystic and macrocystic types, with a mixed type also observed clinically. LMs are mainly diagnosed in infants and young children; 90% of diagnoses are made before the age of 2 years, with no clear sex predisposition. 1 It is rarely seen in adults. LMs can occur anywhere in the body, but they are most commonly found in the head and neck region, accounting for about 75% of cases. 4 Other locations include the chest, mediastinum, axilla, groin, and limbs. Despite being congenital, LMs can grow slowly over 1 to 2 years, often without specific symptoms. In this case, the pharyngeal mass originated from the left side of the posterior pharyngeal wall and showed no symptoms until the patient started snoring 11 years after birth. Both intraoperative frozen sections and postoperative pathology confirmed the diagnosis of LM. The incidence of posterior pharyngeal LMs in children is extremely low, with no domestic reports identified to date. 5
Pediatric posterior pharyngeal LMs lack specific clinical or imaging characteristics, thus requiring differentiation from posterior pharyngeal cysts, posterior pharyngeal abscesses, and cervical neurogenic tumors. In this regard, electronic nasopharyngoscopy, neck ultrasonography, neck CT, and MRI together with histopathological examinations are important tools for differentiation. Electronic nasopharyngoscopy can provide clear and direct visualization. Preoperative neck ultrasound is simple, convenient, and rapid. On ultrasound examination, the LM appears as cystic anechoic mass with clear borders, a smooth surface, and enhanced posterior echoes. 6 It can be distinguished if there is associated infection or bleeding. Ultrasound is effective for confirming the extent of the LM, any adhesion of the lesion to surrounding tissues, and the presence of mixed vascular tumor tissues within the lesion. Imaging examinations also have significant value in the diagnosis of posterior pharyngeal LMs, providing information on localization as well as a qualitative diagnosis. MRI is considered the best imaging method for the diagnosis of pharyngeal masses. 7 The CT scan of this patient showed a cystic tumor with uniform low density, and no enhancement of the cystic content was observed after injection. A space-occupying lesion was found on the left side of the posterior pharyngeal wall in this case. MRI is superior to CT in imaging LMs, with lower or equal signals on T1WI and high signals on T2WI. 8 After finding a mass on the left side of the posterior pharyngeal wall in this case, the most common differential diagnoses included posterior pharyngeal cyst, posterior pharyngeal abscess, and cervical neurogenic tumor. 9 However, the child had no history of upper respiratory tract infection and no signs of fever, throat pain, or refusal to eat due to throat pain, which are characteristics of posterior pharyngeal abscesses. Nor was there supportive radiological evidence. After the initial clinical and radiological diagnoses, histopathological examination confirmed the diagnosis of LM.
At present, the main methods used for treating LM include conservative observation, surgery, sclerosant injection, and oral medication therapy. 10 Nevertheless, complete surgical resection represents the primary approach, aiming to remove as much of the lesion tissue as possible while preserving the function of the surrounding normal tissue structures. A challenge associated with surgery is managing the child’s airway during the perioperative period. An LM in the retropharyngeal space can cover a significant area, extending from the nasopharynx to the laryngopharynx. Both pharyngeal swelling and airway blockage can be caused by postoperative edema and bleeding. Pharyngeal obstruction often requires a tracheotomy, which is performed in approximately 50% of such cases. 11 To avoid respiratory difficulties due to the obstruction of the upper airway during and after surgery, the patient in this case chose to undergo a temporary tracheotomy before the removal of the mass. After the tracheotomy was performed, the mass was exposed with a mouth opener attached, and the pharyngeal wall was incised along the longitudinal axis of the mass. The mass was separated from the surrounding normal tissue with a dissector, and an electrosurgical knife was used to complete the excision. Adequate hemostasis was achieved, and the incision in the posterior pharyngeal wall was sutured with 4-0 absorbable sutures. The volume of intraoperative bleeding was approximately 20 ml, with no damage to the surrounding blood vessels or nerves. Postoperative prognosis was favorable.
Conclusion
In children, LMs lack typical symptoms and present with a diverse array of clinical manifestations. Among these, LMs with snoring as the primary symptom are extremely rare, potentially leading to missed or erroneous diagnoses. This report describes the case of a child with LM whose main symptom was snoring. The child underwent pharyngeal mass resection and temporary tracheotomy, with a favorable postoperative prognosis. However, more cases are needed for further study.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
PJ, WYL, HCW, and HGP contributed to the study conception and design; data acquisition, analysis, and interpretation; and drafting and critical revision of the manuscript. LL contributed to the study design and data interpretation and critically revised the manuscript. All authors provided final approval and agreed to be accountable for all aspects of the work.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author (HGP,
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our Research Project was fully sponsored by Guangdong High-Level Hospital Construction Fund Clinical Research Project of Shenzhen Children’s Hospital. (No: JCYJ20210324143008022).
Ethics Approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional review board. As a case report, no ethics approval is required in our institute.
Informed Consent
As all participants included in the study were under the age of 18 years, informed consent was obtained from all individual participants’ parents and/or legal guardian for the use of their medical records and examination images in writing this study.