
Abstract
Keywords
Introduction
Conductive hearing loss (CHL) exerts widespread negative effects on daily life and is associated with communication difficulties, poor academic performance, impairments in social functioning, cognitive decline, and mood-related symptoms.1-3 Prompt hearing rehabilitation with a bone conduction device (BCD) is well accepted as a treatment for patients with irresolvable bilateral CHL; however, it has been difficult to reach a consensus on the optimal strategy for hearing management in patients with unilateral conductive hearing loss (UCHL), as it is generally believed that 1 ear with normal hearing (NH) can provide the sensory cues necessary for basic comprehension of speech. Furthermore, hearing performance is highly variable among individuals with UCHL.4,5 Given the increasing demand for quality of life, concerns regarding the societal and public health impacts of UCHL have grown, and multiple studies have demonstrated that UCHL may involve the typical problems associated with asymmetric hearing, especially in challenging listening environments.6,7
Binaural hearing facilitates exceptional performance in listeners with bilateral NH in competitive listening tasks, such as speech perception in noise and sound source localization.8,9 The main processes contributing to the advantages conferred by binaural hearing during speech perception are binaural summation, binaural squelch, and the head shadow (HS) effect. Summation effect, also known as redundancy effect, illustrates the performance advantage gained from a second ear due to the presence of redundant and/or complementary speech information in both ears. Squelch effect also represents the auditory performance advantage derived from binaural listening, which is attributed to an enhanced internal signal-to-noise ratio (SNR), facilitated by the calculation of interaural time differences (ITDs) and interaural level differences (ILDs). HS effect describes the performance advantage derived from an enhanced monaural SNR at 1 ear, resulting from sound attenuation due to the physical obstruction presented by the listener’s head. 10 Together, these properties enable the transmission of a sound signal with a more favorable SNR to the auditory center of the brain, thus resulting in a decrease in the speech reception threshold (SRT) and improving speech intelligibility. Sound source localization is a complex auditory ability that plays a key role in the integration of peripheral and central auditory processes. Sound sources are localized based on the perception of the source position in 3 planes: vertical, horizontal, and distance. In general, stereo-localization of sound sources relies on the combined processing of monaural and binaural hearing cues.11-13 Vertical and distant localizations are highly dependent on monaural spectral shape cues generated from the pinna, head, shoulders, and bust, although studies have confirmed that distance localization is easier in familiar hearing environments.11,12 Horizontal localization abilities arise from the integration and processing of differences in the timing (ITD) and intensity (ILD) of sound signals between the 2 ears. ITD is the basis for localizing sound sources at frequencies below 1,500 Hz, whereas ILD is the basis for localizing sound sources at frequencies above 1,500 Hz.11,13 Several studies have reported that patients with UCHL experience deterioration in speech perception, spatial hearing abilities, and academic achievement upon elimination of binaural cues.3,14-16
BCDs bypass impaired or compromised components of the external and/or middle ear, and stimulate the cochlea by vibrating the skull. 17 Evidence has demonstrated that BCDs are an effective rehabilitation method for the treatment of UCHL, especially in those who cannot use conventional hearing aids and those for whom hearing reconstruction surgery is temporarily contraindicated (eg, in patients with congenital aural atresia, or chronic otitis media with external ear canal eczema).18,19 It has been proven that BCDs are associated with improvements in speech recognition in both quiet and noisy environments in patients with congenital and acquired UCHL.15,20,21 However, large inter-individual variations in sound localization have been reported among participants, and most patients with UCHL fitted with BCDs continue to exhibit poorer sound localization ability than those with NH. For example, Agterberg et al 14 and Vogt et al 22 demonstrated improved sound localization in both patients with congenital and acquired UCHL fitted with BCDs, while others have reported no obvious improvements in patients with congenital UCHL.23,24 Inevitably, these studies are constrained by the heterogeneity of the study populations, variations in age, duration of hearing loss, degree of hearing loss, and duration of BCD usage. Moreover, such studies have predominantly focused on congenital cases or a combination of congenital and acquired cases. However, it is crucial to acknowledge the significant distinction between congenital and acquired UCHL. In cases of congenital UCHL, adaptations to residual binaural hearing during auditory development can occur, 19 potentially resulting in differences in speech recognition and sound localization ability when individuals with congenital UCHL are fitted with a BCD.
Acquired UCHL typically results from conditions such as otitis media, 25 middle ear cholesteatoma, 26 and trauma. 27 Even though the issues associated with unilateral hearing loss (UHL) have been extensively documented, the compliance rate of BCD utilization among these patients is still low. In addition, to the best of our knowledge, there is a lack of prior research investigating the impact of BCDs on the components of binaural hearing effects and sound localization performance specifically in individuals with acquired UCHL. Therefore, the primary objective of this study was to examine how acquired UCHL influences speech recognition and sound source localization performance in multisource competing environments. Additionally, we aimed to determine whether BCDs provided hearing benefits in these challenging listening tasks. Ultimately, the goal of this research was to establish a theoretical basis for hearing intervention programs in clinical settings. To mitigate confounding variables, acquired UCHL was simulated using an earplug combined with an earmuff in listeners with bilateral NH, and a within-subject repeated-measures design was used to compare hearing outcomes among 3 listening conditions: NH, unilateral plug (UP; simulated UCHL), and UP + BCD. Binaural hearing outcomes were examined according to factors influencing the SRT, including summation, squelch, HS effects, and the mean absolute error (MAE) of sound source localization.
Materials and methods
Participants
Twelve adults with NH were recruited and signed up to participate in this study. All participants had NH with pure tone audiometry (PTA) of air conduction (AC) thresholds less than or equal to 20 dB Hearing Level (HL) across octave frequencies, 250 to 8000 Hz, bilaterally. Other criteria for inclusion are (1) a native speaker of Mandarin; (2) no current or previous history of chronic ear disease; and (3) sufficient understanding of test content and cooperating well with the pretest. The participants who were not able to do the instructions or those without enough motivation were excluded from this study. Two listeners did not accomplish the whole test because of time conflicts. Therefore, 10 participants (mean age: 29.9 ± 4.77, from 25 to 38 years) were included in the final statistical analysis. All experimental protocols were approved by the Ethics Committee of Anhui Medical University Committee (PJ 2022-14-50) and written informed consents were obtained from all participants.
Measurements
All measurements were carried out in a double-walled, sound-attenuating auditory lab. Seven speakers (Genelec 8030A) were placed horizontally to form a semicircle facing the listener, 30° apart and ranged from −90° to 90°. Participants sit on a chair in the center of the loudspeaker cone, 1 m from each speaker. The height of the seat could be adjusted individually to enable the listener’s ears to be at the same elevation as the speakers.
Sound field hearing thresholds
Sound field hearing thresholds were measured with warble tones played by the speaker located at the front (0°, azimuth). The mean sound field hearing threshold was defined as the average of the thresholds for frequencies from 0.25 to 4 kHz.
Speech reception thresholds and binaural hearing effects
SRTs were evaluated using the Mandarin Speaking Test Materials (MSTMs). 28 Target speech stimuli from MSTMs were spoken by an adult male who is a native speaker of Mandarin. The MSTMs contain 10 lists of 50 disyllabic words, all of which have been analyzed for equivalence to serve as speech stimuli. To reduce the influence of vocabulary memory on speech outcomes, the order of the word list was played in randomized without repetition for each participant. The masker was the broadband speech-spectrum noise (SSN) fixed at 65 dB Sound Pressure Level (SPL) and was presented continuously during the SRT evaluation task. During the SRT test, each run was started with a speech stimulus at 65 dB SPL. Participants were told to ignore the background SSN to make the best guess of the presented speech stimuli played by the speaker. They were requested to make a response of repeating each disyllabic word in 5 seconds after the end of each speech presentation. The SRT was estimated using a 2 dB-up, 2 dB-down tracking procedure of target speech stimuli according to their responses. To obtain the most accurate SRT results for each participant, the words within the SRT neighborhood intensity were played multiple times for the participant to respond. The SRT50 was defined as the SNR at which 50% of the presented speech stimuli were understood correctly. The measurement was performed as a closed disyllable test, where listeners did not receive any feedback after answering.
Binaural summation effect, squelch effect, and HS effects are calculated with the target speech and SSN in co-located and separated conditions as follows:
Binaural summation effect (S0N0): speech signals and SSN were presented from the front (0°, azimuth).
Binaural squelch effect (S0NHL): speech signals were presented from the front (0°, azimuth), while SSN was presented from the UHL side (+90°, azimuth).
HS effects (SHLNNH): speech signals were presented from the UHL side (+90°, azimuth), while SSN was presented from the NH side (–90°, azimuth).
Sound localization
To assess sound localization abilities, broadband noise (0.5–20 kHz) burst with a 1000 mseconds (long) duration was presented at 3 different sound levels (65–75 dB SPL, in 5 dB SPL increments) in randomly interleaved from 7 speakers. During the testing session, the loudspeakers were randomly presented twice for each sound level burst, with a total of 42 stimulus trials in each run. Participants are not allowed to move their heads during the presentation of the noise bursts. After each presentation, participants were allowed to indicate the direction of the sound source and could turn their heads to observe the number assigned to the loudspeaker they believed produced the sound burst and were requested to return their heads to face the front loudspeaker (0, azimuth) after giving responses without receiving any feedback.

The accuracy of sound localization was evaluated by the MAE (equation (1)). αRESP and αTRAG represent the response and target azimuths (in degrees), respectively. Equation (2) is applied to calculate the best linear fit to the target-response relationship for each participant, in which g represents the response gain (slope) and b represents the response bias (offset).
Procedures
UHL simulation and confirmation
UHL was simulated using a foam earplug (E-A-R soft; 3M Company, Saint Paul, MN, USA) inserted in the external ear canal together with an earmuff covering the whole auricle (Peltor X5A; 3M Company, Saint Paul, MN, USA). 29 To ensure optimal attenuation, the earplug was inserted as deeply as possible into the subject’s ear canal, and the earmuff was placed carefully to cover the whole pinna without obstructing the contralateral ear. Simulation was uniformly performed on the right side and all manipulations were performed to the tolerance of participants. Typically, this simulation method led to moderate UCHL, characterized by a range from 41 to 60 dB HL.
The UHL simulation effect of the earplug and earmuff combination was confirmed using sound field hearing thresholds measured by the loudspeaker at 0° azimuth. The contralateral ear of the simulated side was also plugged with the same combination of earplug and earmuff, and this contralateral plugging was not retained during the formal speech recognition and sound localization tests. NH thresholds (without plugging) and bilaterally plugged hearing thresholds at frequencies of 0.25, 0.5, 1, 2, and 4 kHz were recorded, and the average difference was considered as the attenuation provided by the simulation of UHL. The attenuation values were obtained for all participants before the formal trials.
Device
The BAHA5 was used as a bone conduction stimulator and was fitted with a softband on the mastoid posterior to the pinna. The tightness of the softband was adjusted based on the participant’s comfort level; besides, special care was taken to avoid contact between the audio processor and the earmuff. Before the formal test, the device was set to omnidirectional mode and automatically adjusted for directionality and noise reduction. Due to the inherent limitations of the Bone-anchored Hearing Aid (BAHA) device, it is not feasible to replicate the exact hearing level of the contralateral side across all frequencies on the plugged side. Consequently, the volume settings for the BAHA5 are determined based on participant preferences, guided by the patient’s maximum comfort threshold. This approach aims to provide the closest possible match to the contralateral hearing that the patient can tolerate, thereby striving to achieve improved interaural loudness balance. All settings remained constant throughout the experiments.
Listening and test conditions
Three listening conditions were measured for all participants (C1): NH condition (without plugging); (C2) UP condition (simulated UHL) and (C3) UP + BCD condition (simulated UHL aided with BCD, Figure 1). All participants’ listening conditions were randomly varied, and the positions of the earbuds, earmuffs, and BCDs were not allowed to be moved during the experiment.
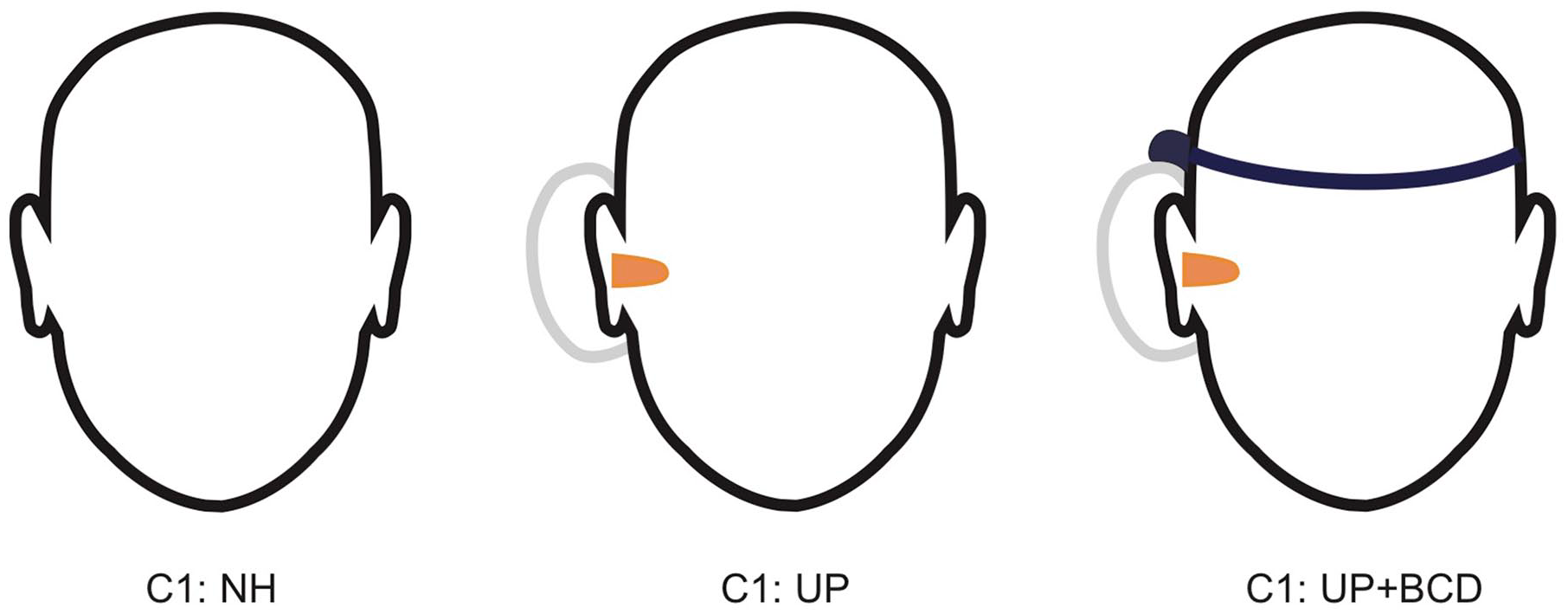
Schematic diagram of the 3 listening conditions, C1 (NH), C2 (UP), and C3 (UP + BCD) the tests of speech perception abilities and sound source localization.
Analyses
The data in this study were presented as mean ± standard deviation (SD), and a normal distribution test was conducted to check the data normality. To evaluate differences under different hearing conditions, the Wilcoxon signed-rank test was performed. A P-value <.05 was regarded as a significant difference in this study. The statistical analysis was performed by SPSS 26.0 (IBM Inc, New York, NY, USA). Figures were drawn using Adobe Illustrator 2020 (Adobe Inc, San Jose, CA, USA) and GraphPad Prism 8.0 (GraphPad Inc, San Diego, CA, USA).
Results
Sound Field Hearing Thresholds
Table 1 and Figure 2 show the mean ± SD for sound field hearing thresholds measured under the NH, bilateral plug, and bilateral plug + unilateral BCD conditions for the range of 0.25 to 4 kHz. A significant increase in the hearing threshold was observed in the bilateral plug condition when compared with the threshold observed in the NH condition (54 ± 3.65 dB HL vs. 13.9 ± 3.57 dB HL, P < .01). When BCD assistance was employed, we observed a substantial decrease in the mean hearing threshold relative to the bilateral plug condition (27.3 ± 1.25 dB HL vs. 54 ± 3.65 dB HL, P < .01); however, the aided hearing thresholds remained higher than those in the NH condition (27.3 ± 1.25 dB HL vs. 13.9 ± 3.57 dB HL, P < .01).
The Means and SDs of Sound Field Hearing Thresholds (dB HL).

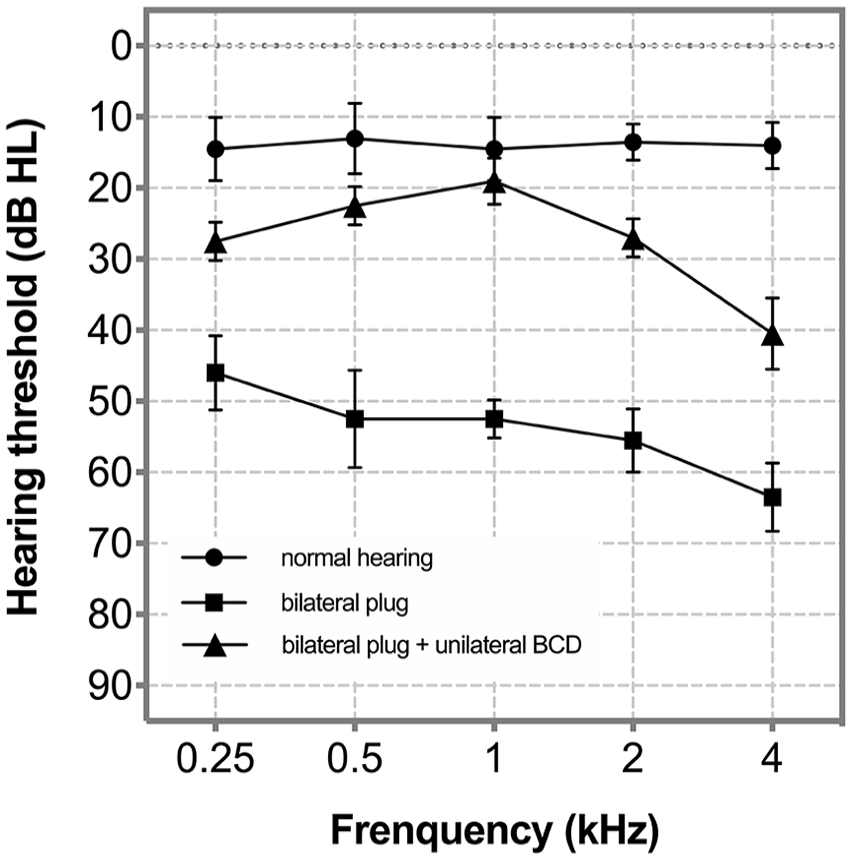
The means and SDs of sound field hearing thresholds at frequencies from 0.25, 0.5, 1, 2, and 4 kHz. Error bars represent ±1 SD.
SRTs and Binaural Hearing Effects
Table 2 and Figure 3 show the SRTs in the 3 spatial configurations of S0N0 (summation effect), S0NHL (squelch effect), and SHLNNH (HS effect). In the NH condition (C1), the mean SRT was −10.6 ± 3.63 dB SNR for the S0N0 configuration, −8.7 ± 4 dB SNR for the S0NHL configuration, and −18.1 ± 5.57 dB SNR for the SHLNNH configuration. Unilateral plugging (C2) resulted in significantly higher (ie, worse) SRTs in each spatial configuration of S0N0 and SHLNNH (S0N0: −6 ± 3.97 dB SNR, P < .01, SHLNNH: −6.5 ± 4.28 dB SNR, P < .01) when compared with those measured in the NH condition (C1). However, in the configuration of S0NHL, no significance was found (S0NHL: −7.1 ± 3.93 dB SNR, P = .087). When BCD assistance was employed (C3), the SRTs changed to −7.9 ± 4.07 dB SNR for the S0N0 configuration, −7.9 ± 4.63 dB SNR for the S0NHL configuration, and −12.6 ± 4.25 dB SNR for the SHLNNH. In the S0N0 and SHLNNH configuration, the mean SRT was significantly lower (i.e., better) in C3 than in C2 (all P < .01), but remained higher (i.e., worse) than that in C1 (S0N0, P < .05; SHLNNH, P < .01). However, in the S0NHL configuration, there were no significant differences between C3 and C2 (P = .209) or between C3 and C1 (P = .394).
The Means and SDs of SRTs (dB SNR).
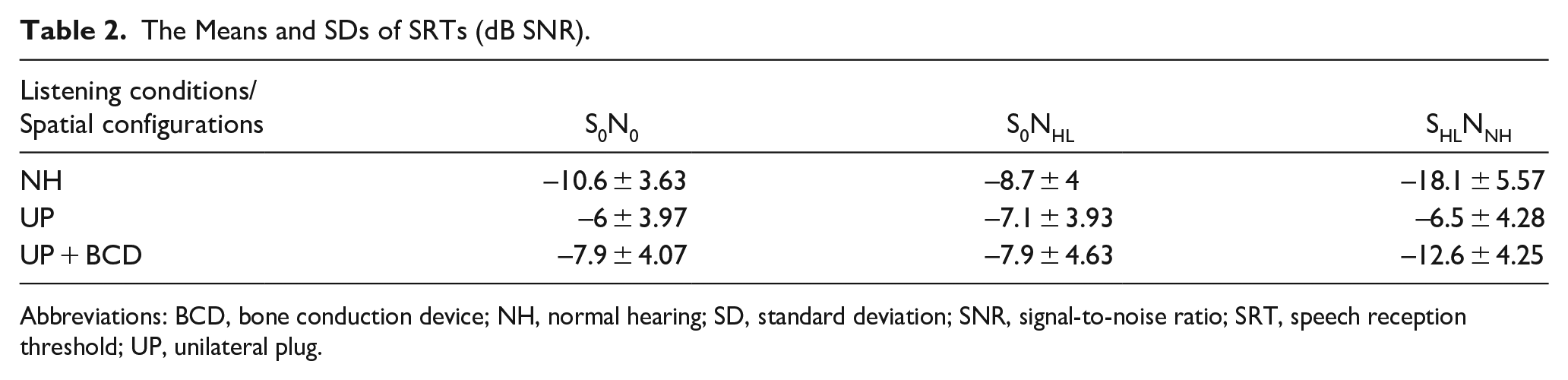
Abbreviations: BCD, bone conduction device; NH, normal hearing; SD, standard deviation; SNR, signal-to-noise ratio; SRT, speech reception threshold; UP, unilateral plug.
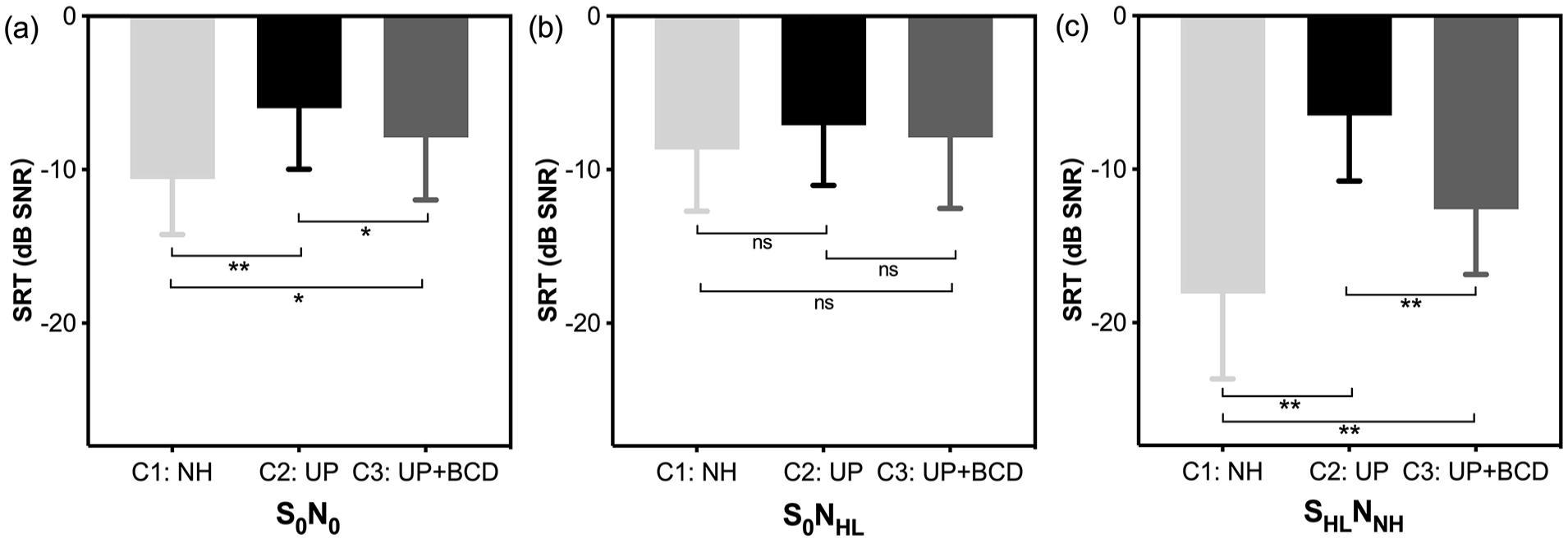
The means and SDs of SRTs (in dB SNR) were performed in the NH condition (C1), UP condition (C2), and UP + BCD condition (C3). Three binaural hearing effects of (a) S0N0 (summation effect), (b) S0NHL (squelch effect), and (c) SHLNNH (HS effect) were measured, respectively. Lower SRTs represent better speech perception abilities in noise.
Sound Source Localization
Figure 4a shows the target–response plots of 2 representative participants (P4 and P7) in the UP (C2, left column) and UP + BCD (C3, right column) conditions. The sound levels of the presented stimuli are indicated as solid black (65 dB SPL) or hollow square (70 dB SPL) data points. In C3, both listeners perceived the stimuli mainly via the unplugged left ear (P4, bias = 0.042; P7, bias = 0.173). BCD assistance improved the accuracy of sound source localization for P4, as demonstrated by a decrease in the MAE from 66.43° to 37.14°. However, BCD did not improve sound source localization in P7, who exhibited an increase in the MAE from 68.58° to 74.29°. In Figure 4b, the MAEs measured in the UP condition (C2, x-axis) are plotted against those measured in the UP + BCD condition (C3, y-axis). Data points above the dashed diagonal suggest that the participant acquired a more accurate sound localization ability in C3 than in C2. For all listeners, the accuracy of sound source localization was poorer in C2 (MAEC1 vs MAEC2, 0 vs 61.22° ± 18.69°, P < .01) and C3 (MAEC1 vs. MAEC3, 0 vs 52.43° ± 18.13°, P < .01) than in C1. Most listeners (7/10) exhibited better localization ability in the aided condition (data points above the dotted diagonal line). However, statistical analysis revealed no significant improvement in sound localization accuracy with the use of BCD (MAEC2 vs MAEC3, 61.22 ± 18.69° vs 52.43 ± 18.13°, P = .059).
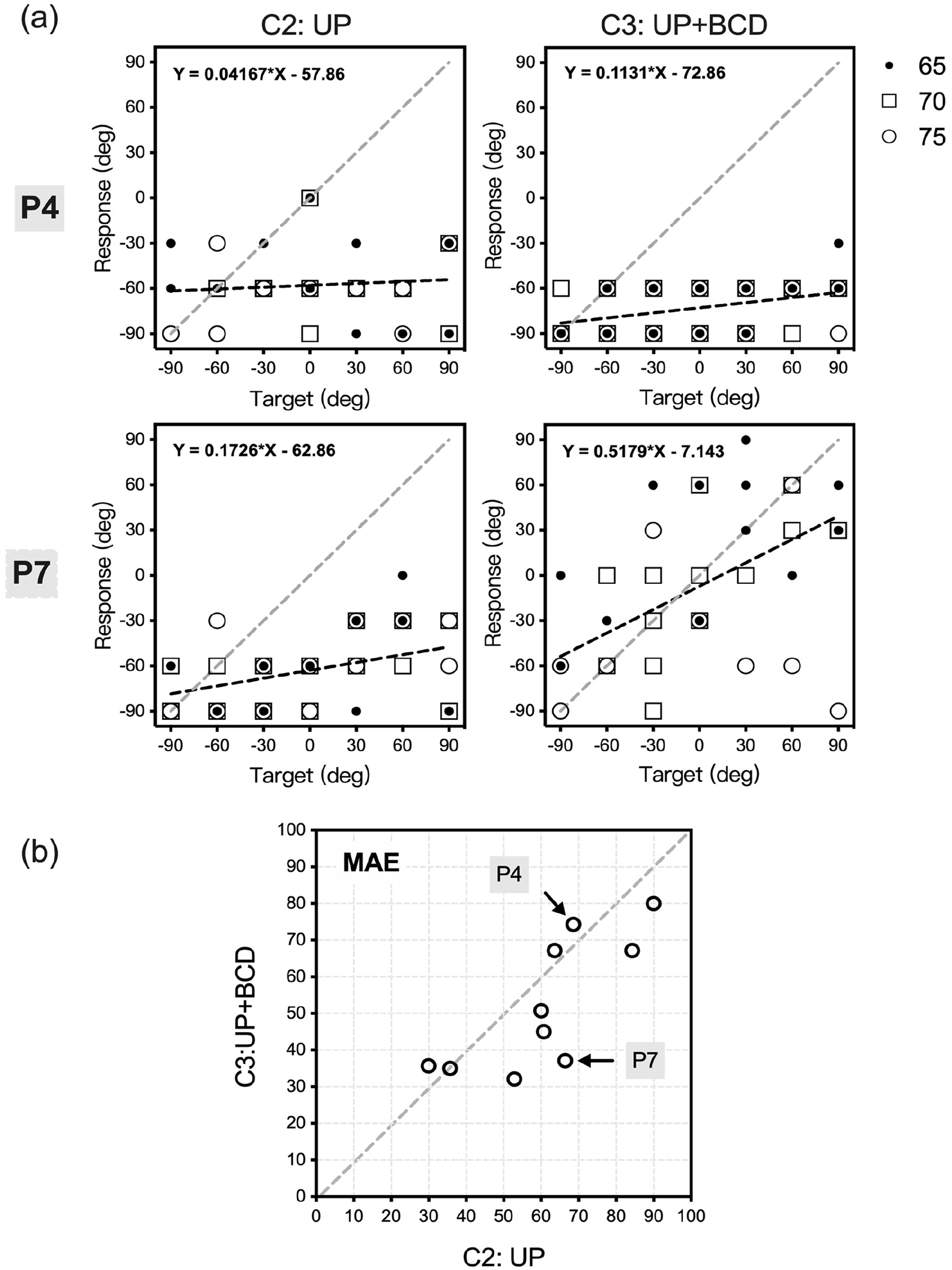
(a) Target-response plots of 2 representative participants (P4, P7) in listening conditions of the UP condition (C2, left column) and UP + BCD condition (C3, right column). Sound levels of presented stimuli are indicated by black solid data points (65 dB SPL), hollow square data points (70 dB SPL), and hollow circle data points (75 dB SPL). Best-fit linear regression for the integration all sound levels is indicated by a black dashed line. The gray dashed diagonal indicates the best sound source localization level of MAE measured in C1. (b) The MAEs measured in the UP condition (C2, x-axis) are plotted against those measured in the UP + BCD condition (C3, y-axis). P4 and P7 depicted in (a) are marked.
To further investigate the characteristics of BCD assistance (C3) on the acquired UCHL (C2), the MAE for sound source localization was evaluated at 3 different sound levels, respectively (Figure 5a). The localization ability was significantly more accurate (lower MAE value) in C3 than in C2 at 65 dB SPL (P < .05), but not at 70 dB SPL (P = .052) and 75 dB SPL (P = 1). Then, we separately calculated the difference in MAE between C2 and C3 from different angles (Figure 5b). Significant differences in MAE between these two listening conditions were found at presented angles of +30° (P < .05) and +60° (P < .05), but not at −90° (P = .676), −60° (P = .172), −30° (P = .311), 0° (P = .523), or +90° (P = .202).
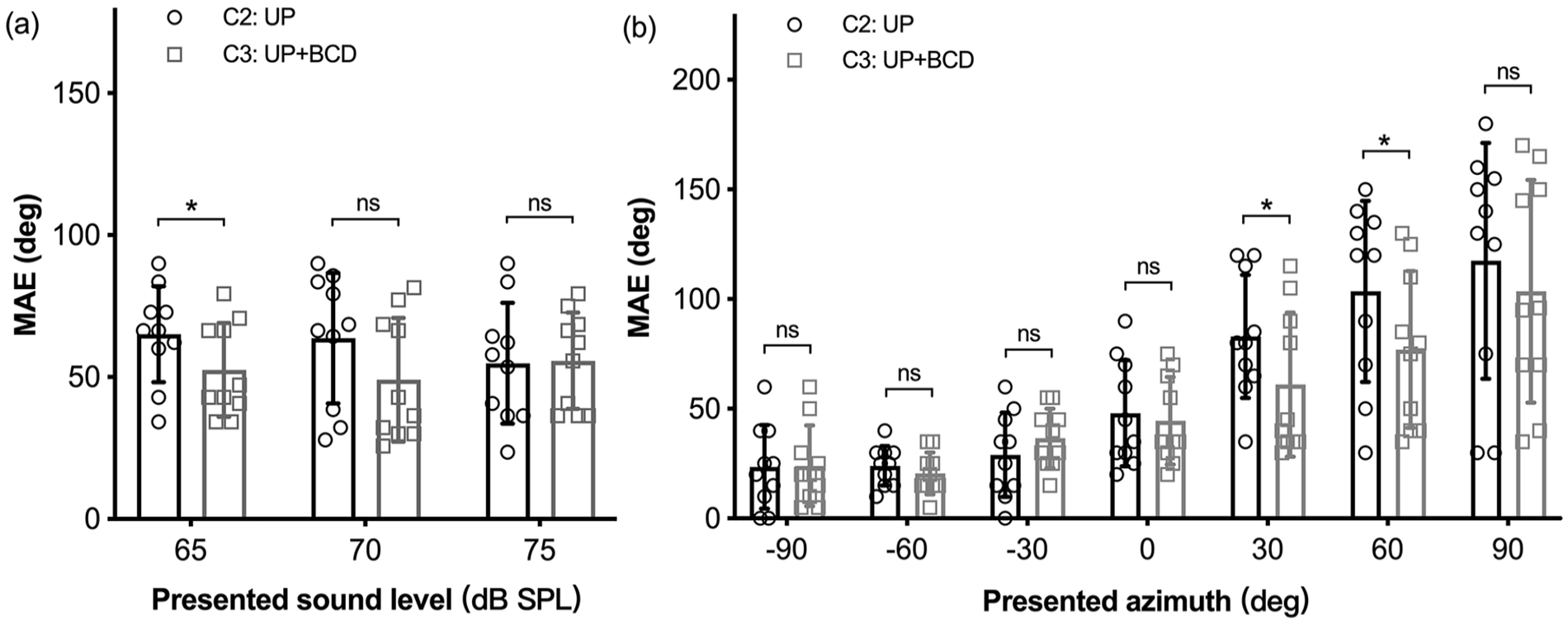
Individual MAE (deg) of sound source localization were represented at (a) 3 sound levels and (b) 7 presented azimuths. MAEs measured in the UP condition (C2) and UP + BCD condition (C3) are indicated by hollow circle and hollow square, respectively. Error bars represent ±1 SD.
Discussion
The present study evaluated differences in speech perception based on binaural hearing effects and sound source localization ability among individuals with simulated UCHL in NH (C1), UP (C2), and UP + BCD (C3) conditions. BCD assistance (C3) improved the summation and HS effects in all listeners with simulated UCHL, resulting in a lower (ie, better) SRT than that observed in C2; however, no significant differences in squelch effects were observed between C2 and C3. Notably, most listeners exhibited more accurate sound source localization in C3 than in C2, demonstrating the benefits of BCDs. BCD assistance mainly improved localization accuracy when the noise stimuli were presented at low intensities and on the hearing-impaired (plugged) side, suggesting that the benefits of BCD for sound localization are not based on the reacquisition of binaural processing.
Speech Perception Based on Binaural Hearing Effects
Consistent with our results, a previous study using simulated UCHL also reported significantly worse speech perception in noise (S0N0) in the UP condition than in the NH condition. 29 Our analysis of the HS effect indicated that SNR was significantly lower (ie, better) in the NH condition (C1) than in the UP condition (C2). While no studies to date have tested SNR to examine the HS effect in listeners with simulated UCHL, our results are comparable to those of previous studies comparing SNR between patients with UCHL and control listeners with NH. 30 This finding aligns with the view that enhancing monaural SNRs in hearing aids is more effective for optimizing speech intelligibility than preserving ILDs.10,31 When measuring the summation and HS effects, the use of BCD in C3 decreased the SNR when compared with that in C2, leading to mean improvements of 1.9 and 6.1 dB SNR for speech perception in noise. Owing to variations in methodology and the coupling system,32,33 discrepancies may occur when assessing binaural hearing outcomes, rendering comparisons between the current data and those from prior studies challenging. Most of these studies have reported a beneficial effect of BCDs on speech perception in these 2 test conditions for patients with UCHL.15,20,21,30 However, the BCD did not significantly influence the squelch effect (P = .417). Similar results were described by Kunst et al, 34 who reported no significant changes in the SNR measured under S0NHL conditions before and after the use of a bone-anchored hearing aid in patients with UCHL. This lack of statistical significance may be because binaural hearing cannot be achieved under the instant aided condition, given the existing level of hearing asymmetry and the internal processing time of the BCD. Moreover, the small sample size limits the ability to detect subtle changes.
Sound Source Localization
All listeners exhibited ideal, accurate sound source localization (MAE = 0) in the NH condition (C1). Consistent with some previous literature on relatively good monoaural sound localization ability in patients with UCHL, unilateral plugging induced a dramatic decrease in localization accuracy for all listeners, yielding an average MAE of 61.22 ± 18.69°. Agterberg et al 14 proposed that some listeners with UCHL may use remaining binaural cues, monaural spectral pinna cues, and HS effects to localize sound sources. In our study, listeners may have been unable to adapt to the newly distorted binaural cues remaining after instant plugging, which may have prevented them from regaining localization ability within a short period. Snik et al 24 described a similar situation in which better localization ability was observed in patients with congenital UCHL than in those with acquired UCHL. Taken together, these findings emphasize the importance of adaptation in monaural sound localization.
In patients with unilateral sensorineural hearing loss receiving cochlear implants, significant improvements in sound source localization ability have been demonstrated, 35 while the hearing in the contralateral (NH) ear remains unaffected 36 ; moreover, the use of cochlear implants has been shown to have a positive impact on the overall quality of life of these patients. 37 However, BCDs stimulate both the ipsilateral (impaired) ear and the contralateral (NH) cochlea, leading to “cross-hearing” that may introduce interfering inputs to the NH ear. 38 Thus, the effect of BCDs on sound source localization in patients with UCHL remains controversial. Some studies have reported beneficial effects of BCDs in patients with congenital UCHL (ie, congenital unilateral microtia and atresia), 22 while others have reported no obvious effects of BCDs on localization accuracy. 23 As such, researchers have assumed that patients with congenital UCHL may learn to use monaural spectral cues and the remaining binaural cues to localize sound sources, and that the binaural hearing provided by the BCDs cannot restore the ability to decipher the original cues in such a short time. Among patients with acquired UCHL who had previous experience with binaural hearing, the limited number of relevant studies yielded consistent results regarding the ability of BCDs to increase the accuracy of sound source localization. Agterberg et al 14 retrospectively analyzed data for 12 patients with acquired UCHL treated using BCDs for at least 1 year, following which improved localization based on biaural cues (ie, ILDs and ITDs) was observed. Our results are in line with previous literature, supporting the notion that BCDs significantly improve horizontal sound source localization in most listeners with simulated UCHL (P < .05).
To further investigate the characteristics of BCD assistance and whether its benefits are related to the effects of binaural processing, we evaluated the impact of BCD assistance on sound source localization at different intensities and angles of presentation. BCD assistance (C3) significantly improved the accuracy of sound source localization at low intensities (65 and 70 dB SPL) and on the sides of hearing impairment (30° and 60°). The lack of improvement at 75 dB SPL can be explained by the relatively good accuracy of localization in the UP condition (C2), rather than by a decrease in performance when using the BCD. This better unaided localization accuracy may be attributable to a sound level high enough to be heard by hearing-impaired (plugged) ears. Notably, we also observed that improvements in localization accuracy with BCD assistance (C3) did not seem to be based on binaural cues, as the use of BCD only improved localization accuracy for stimuli presented on the side of the plugged ear. The inability to achieve binaural hearing with the BCD may be the result of delays in processing time (>3 mseconds) and asymmetric hearing thresholds. 14 It is important to note that most participants in previous studies were recruited retrospectively and had more experience with BCD listening than the participants in the current cohort, which explains why the improvement in sound localization reported by Agterberg et al 18 was based on binaural cues. Further studies are needed to determine the time required for individuals with acquired UCHL to adapt to these processing time delays, and the asymmetric hearing thresholds of a BCD for restoring binaural hearing.
Study limitations and prospects
Due to challenges associated with clinical patient involvement and the requirement for a high level of cooperation from participants in binaural effects and acoustic localization testing, we chose to simulate UCHL in order to minimize confounding factors among the enrolled patients. This approach contributes to one of the main strengths of our study, which is the homogeneity of the participant population. However, it is important to acknowledge certain limitations of this study. First, the simulated UCHL does not accurately replicate a real hearing loss condition. Second, no correlations between listener characteristics (eg, age, sex, degree of hearing loss, and degree of aided hearing threshold) and binaural hearing outcomes were observed. Third, it is important to note that the participants in this study, who already possess spoken language skills, can infer some speech information. This may not apply to children with more limited speech and language development. Thus, to optimize the fitting of BCDs for patients with acquired UCHL, larger studies encompassing real patients from diverse populations are required to better understand how these factors contribute to speech perception and sound source localization ability. Additionally, comparing the outcomes of BCDs with AC devices could provide further insights. It is also important to consider that results might vary in subjects with unilateral mixed hearing loss, as a sensorineural component could alter the quality of neural processing, and a cochlear deficit might introduce further distortions in the acoustic information being processed.
Conclusion
In conclusion, our results demonstrate that the BCD provided stable hearing benefits in binaural hearing effects and sound source localization ability for cases of acquired UCHL where traditional hearing aids cannot be used. Although the benefits obtained by the BCD use appear not to be based on the reacquisition of binaural processing, our results have clinical implications for the promotion of BCD use in patients with acquired UCHL, especially among those who are unable to undergo traditional surgery to improve hearing.
Footnotes
Acknowledgements
We thank Rongtao Cui, Fei Tao, Wei Liu, Yousong Lu, and Jinchao Dong from iFLYTEK company for their technical support.
Author contributions
Conceptualization: Chongxian Yu and Yujie Liu. Data curation: Chongxian Yu and Wenqian Wang. Formal analysis: Yujie Liu, Chongxian Yu, and Yuan Jiang. Funding acquisition: Yehai Liu. Methodology: Yujie Liu and Chongxian Yu. Project administration: Yujie Liu and Xiaoming Zhang. Data visualization: Ping Wang and Xin Ni. Original draft: Chongxian Yu and Mei Zhong. Writing—review & editing: Yujie Liu and Yehai Liu.
Data Availability
All data generated or analyzed during this study are included in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Science and Technology Innovation Microenterprise Project of the National Health Commission (No. 20003).
Ethical Approval
All experimental protocols were approved by the Ethics Committee of Anhui Medical University Committee (PJ 2022-14-50) and written informed consents were obtained from all participants.