
Abstract
Objectives:
Congenital cholesteatomas originate from epithelial tissue present within the middle ear in patients with an intact tympanic membrane, no history of otologic surgery, otorrhea, or tympanic membrane perforation. They are diagnosed by a pearl-like lesion on otoscopy and computed tomography (CT) scan showing an expansile soft-tissue mass. We describe a series of patients with no prior otologic history presenting with progressive unilateral conductive hearing loss and normal otoscopy. The CT scans showed ossicular erosion without obvious soft-tissue mass. Surgery confirmed incudostapedial erosion found to be cholesteatoma. In this study, we characterize the clinical course of patients diagnosed with isolated incudostapedial cholesteatoma (IIC) and review possible pathologic mechanisms.
Methods:
Retrospective review of IIC cases treated by the Department of Pediatric Otolaryngology, Rady Children’s Hospital, San Diego, 2014 to 2020. Data included patient demographics, clinical features, imaging, surgical findings, and audiologic data.
Results:
Five patients were diagnosed with IIC (3 [60%] female; mean age at presentation 10.7 years [range 5.5-16.0]). All patients presented with postlingual unilateral conductive hearing loss and normal otoscopy without any past otologic history; delay in diagnosis ranged from 4 months to several years. The CT scans showed ossicular chain erosion with an absent long process of the incus and/or stapes superstructure. All patients underwent middle ear exploration, revealing a thin layer of cholesteatoma in the incudostapedial region, confirmed by histopathology. Mean preoperative speech reception threshold was 55 dB and improved to a mean of 31 dB in the 4 patients who underwent ossicular chain reconstruction.
Conclusion:
Isolated incudostapedial cholesteatoma should be included as a possible etiology in pediatric patients with insidious onset of unilateral conductive hearing loss with normal otoscopy, unremarkable otologic history, and a CT scan showing ossicular abnormality/disruption without notable middle ear mass. These patients should be counseled preoperatively regarding the possibility of cholesteatoma and should undergo middle ear exploration with possible ossiculoplasty.
Keywords
Introduction
Cholesteatomas represent a destructive, epithelial growth of the temporal bone and can be either acquired or, more rarely, congenital. Congenital cholesteatomas arise in the middle ear behind an intact tympanic membrane without prior history of otologic infection, surgery, or tympanic membrane perforation. 1,2 Although many remain asymptomatic, others can present with conductive hearing loss, labyrinthitis, facial nerve palsy, or intracranial complications—either alone or in combination. 3,4 Diagnosis is made either by otoscopy (pearly white mass in the middle ear), during myringotomy and tube placement, and/or on computed tomography (CT) of the temporal bones—appearing as an expansile mass within the middle ear, sometimes with mastoid extension. 3,4 We describe the clinical course of 5 pediatric patients who presented with unilateral conductive hearing loss, normal otoscopy, no previous otologic history, and CT imaging showing erosion versus abnormality of the incudostapedial region. Surgical exploration of the middle ear confirmed erosion of the incus and/or stapes with a thin layer of cholesteatoma adjacent to the ossicles, but no bulky mass or further bony erosion. Histology demonstrated cholesteatoma—previously not visible either on microscopic ear examination or readily on the CT scan. These isolated incudostapedial cholesteatomas (IICs) do not display the typical examination or imaging features of cholesteatoma and cannot be easily visualized on CT, delaying the diagnosis until symptoms progress.
The exact pathologic origins of cholesteatomas remain an active area of investigation. Acquired cholesteatomas are thought to arise from chronic infections of the middle ear, tympanic membrane perforation (traumatic or surgical), or retraction pocket that permits keratinous debris to enter the middle ear and proliferate. 5 The mechanism of congenital cholesteatoma is not fully understood either, although some hypotheses exist. Perhaps, despite an intact tympanic membrane, congenital cholesteatomas arise via squamous epithelial invasion of a retraction pocket or marginal perforation of tissue, similar to acquired cholesteatomas. 6 Alternatively, inflammation of the middle ear may induce mucosal metaplasia, subsequently forming keratin. 7 Perhaps, the most favored theory of IIC formation postulates that it may originate from aberrations in the normal embryological process of middle ear epithelial formation. 8,9
Isolated incudostapedial cholesteatomas likely represent a subset of posterosuperior congenital cholesteatoma, presenting later in childhood, although the etiology cannot be confirmed with complete certainty. They erode a very specific region of the incudostapedial joint area and do not present with the usual bulky, round cholesteatoma mass. For this reason, they are not readily appreciated on otoscopic examination or imaging and risk going undiagnosed for years, causing progressive damage to the ossicular chain. These patients undergo middle ear exploration, and the diagnosis of cholesteatoma is made intraoperatively. This study aims to describe the clinical course, treatment, and embryological origin of this unique variation of cholesteatoma.
Materials and Methods
Data Collection and Statistical Analysis
This study was approved by the University of California, San Diego, and institutional review board of the Rady Children’s Hospital (#200319). The IIC cases were identified and reviewed retrospectively. Inclusion criteria consisted of pathologically diagnosed IICs, surgically treated by the department of pediatric otolaryngology—head and neck surgery at Rady Children’s Hospital, San Diego, between 2014 and 2020. Recorded outcome measures included demographics, clinical and imaging features, surgical findings, and hearing assessments. Statistical analysis was conducted using Microsoft Excel.
Hearing Assessment
Preoperative and postoperative hearing was assessed using pure tone audiometry with mean residual air-bone gap, based on the difference between air and bone conduction thresholds at 250, 500, 1000, 2000, 4000, and 8000 Hz. Additional audiologic data included speech reception threshold decibels (dB), word recognition percentage, immittance, and otoacoustic emissions.
Surgical Technique
Surgical approach was selected based on CT findings, hearing test results, and integrity of the ossicular chain. Surgical procedures started with endoscopic transmeatal exploratory tympanotomy. Following dissection and removal of the cholesteatoma, an ossiculoplasty was performed either during the same operation or during a second-look procedure. Tissue was sent for microscopic pathologic evaluation in all cases.
Results
Clinical Characteristics
Five patients were diagnosed with IIC (3, 60% female). Mean age of first presentation was 10.7 years (range 5.5-16.0), and mean age of surgical intervention was 12.1 years (range 6.6-17.7). Lesions were right sided in 4 (80%) of 5 cases. All patients presented with unilateral, progressive conductive hearing loss; 1 patient also reported intermittent tinnitus. Patients underwent binocular microscopic otologic examination by the senior author with confirmed bilaterally intact and normal tympanic membranes with clear middle ears. None had any previous, significant otologic history. All patients had passed the newborn hearing screening as well as hearing screenings at school and at their pediatrician’s office. There were no intracranial complications, vertigo, or facial paralysis. Table 1 summarizes individual demographic and clinical characteristics. From the time of surgery, the average length of follow-up was 3.3 years (range 3 months to 5.3 years). There was no residual or recurrent disease.
Patient Demographics at Presentation and Clinical Data.
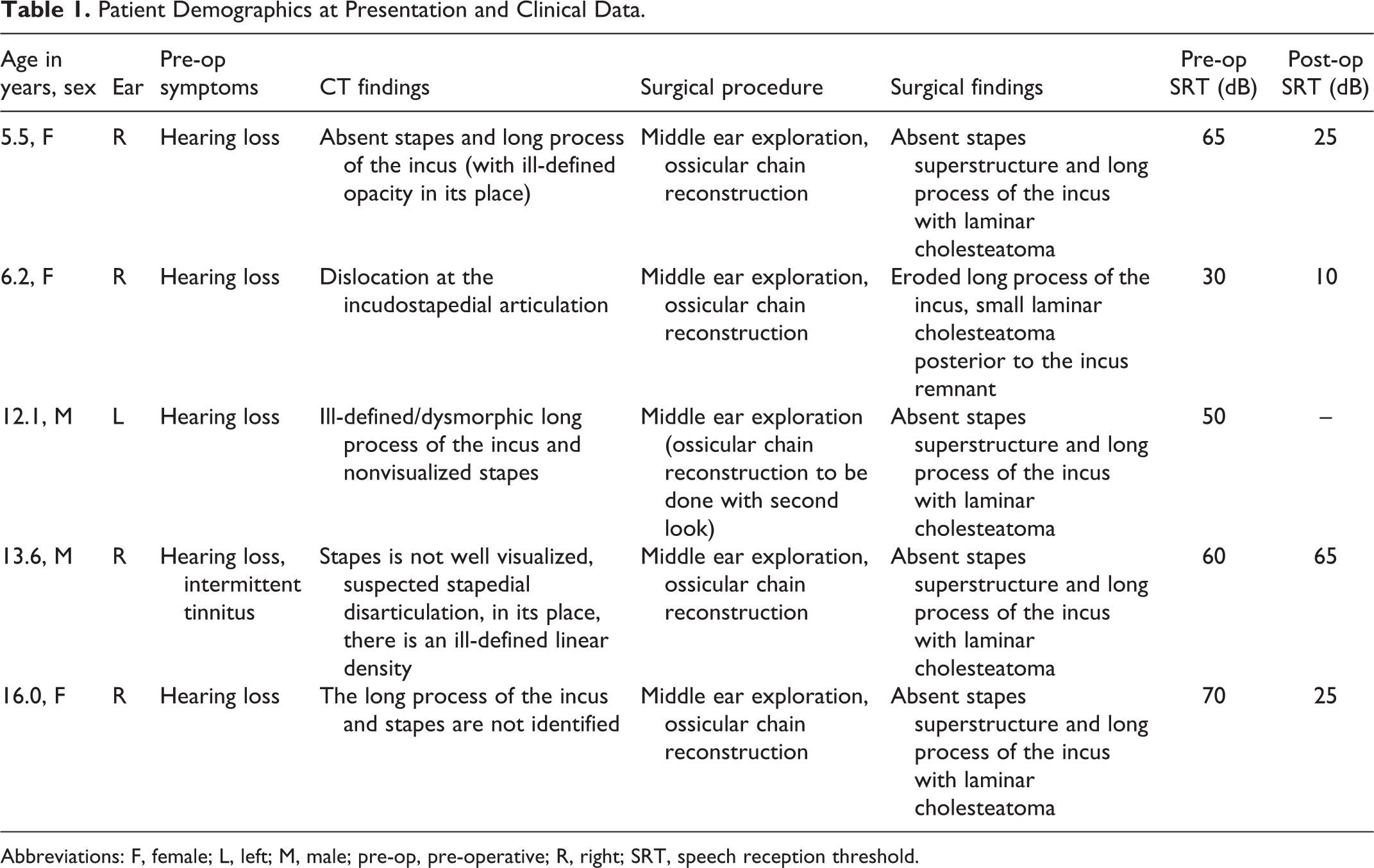
Abbreviations: F, female; L, left; M, male; pre-op, pre-operative; R, right; SRT, speech reception threshold.
Imaging Features
Computed tomography scans of the temporal bone in all patients revealed ossicular abnormalities involving the incus and stapes. Four patients had an absent or poorly defined stapes, 4 had an absent or dysmorphic/eroded incus (particularly affecting the long process), and 1 had incudostapedial disarticulation (see Figure 1). The typical expansile soft-tissue mass in the middle ear or mastoid seen in other cholesteatomas 10 was absent in all cases, representing a defining feature of these cases of IICs.
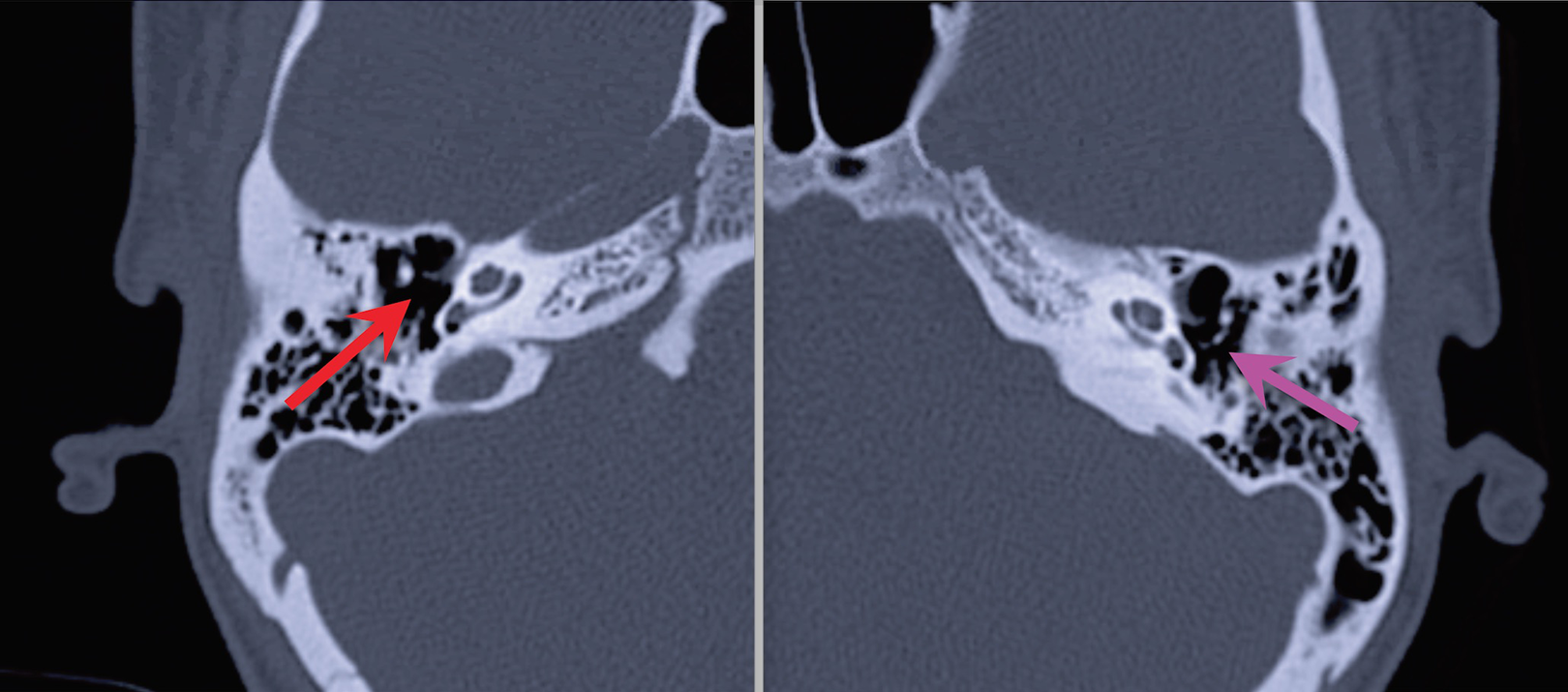
Computed tomography scans of 2 patients with isolated incudostapedial cholesteatoma. The red arrow shows the absence of the stapes superstructure and long process of the incus (no expansile soft-tissue mass is seen in the middle ear). The pink arrow shows the incudostapedial joint on the normal side.
Surgical Findings
All 5 patients underwent endoscopic middle ear exploration and had intact and healthy tympanic membranes on examination, without any retractions or myringosclerosis. Intraoperatively, they were found to have abnormal/eroded ossicles with a thin layer of cholesteatoma adjacent to the ossicles and/or lying over the posterior mesotympanum (Table 1). The cholesteatoma was dissected and removed in all cases. Four of 5 patients underwent ossiculoplasty (either in the same procedure or during a second-look); 1 patient has yet to undergo a second-look with possible ossicular chain reconstruction. Intraoperatively, tissue was consistent with cholesteatoma in all cases. On pathology, all tissue specimens demonstrated keratinous debris, confirming the diagnosis of cholesteatoma. Pathology results were consistent between all cases. Although grossly, IIC lesions appeared small and laminar, pathology results did not differ from more bulky, standard cholesteatoma. The malleus was present and intact in all cases. One patient’s intraoperative cholesteatoma is shown in Figure 2.
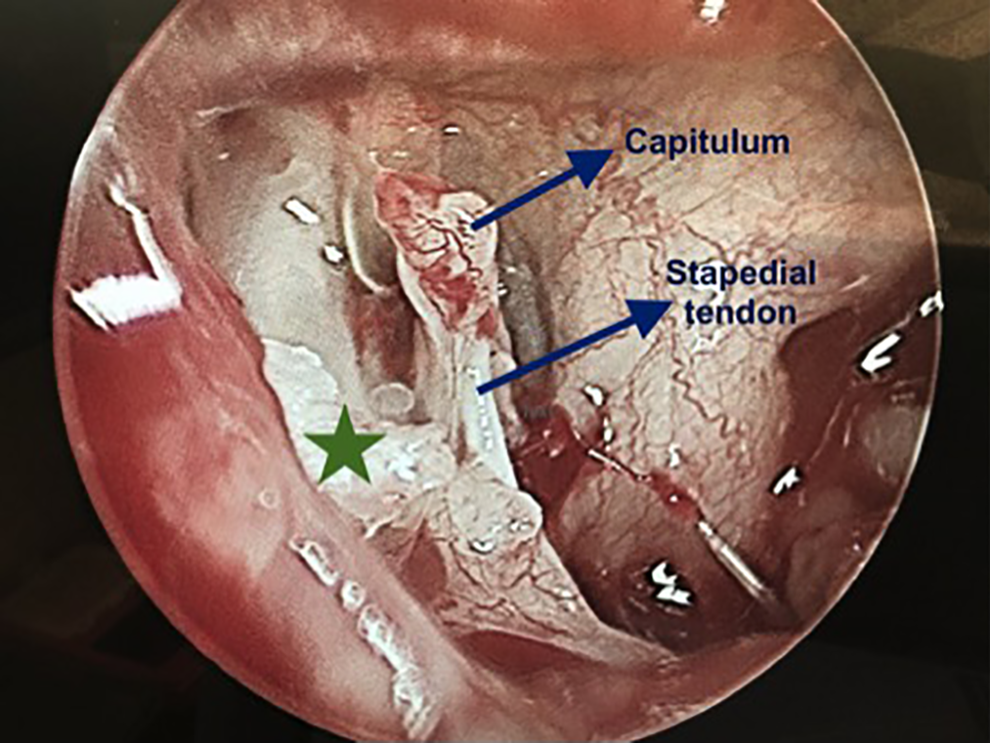
Intraoperative image demonstrating an absent (eroded) long process of the incus and a small laminar cholesteatoma (green star) over the bony canal of the facial nerve extending over the pyramidal process/stapedial tendon.
Hearing Assessments
All patients presented with moderate-to-severe unilateral conductive hearing loss. The average preoperative speech reception threshold was 55 dB (range 30-70 dB) and improved to a mean of 31 dB (range 10-65) postoperatively in the 4 patients who underwent ossicular chain reconstruction (Table 1). Postoperatively, 3 of 4 patients experienced significant hearing improvement. Word recognition percentage was only modestly affected by the pathology and subsequent reconstruction (preoperative range 88%-100% and postoperative range 92%-100%). Preoperatively, otoacoustic emissions were absent in all patients, and immittance results either demonstrated normal middle ear function (3/5 patients) or hypercompliance of the tympanic membrane (2/5 patients).
Discussion
Isolated incudostapedial cholesteatomas represent a variety of an already rare diagnosis, but demonstrate a specific pattern of erosion unique among other cholesteatomas. 11 In contrast to the more common presentation of a pearl-like mass, these IIC lesions are isolated to the incudostapedial region with limited but critical destruction of the ossicular chain. This ossicular destruction does not reflect advancement of a large mass lesion, but instead of a relatively confined pathology. 12 By the nature of their anatomic location, IICs remain out of view on otoscopy, making them particularly challenging to diagnose. They also differ in presentation from traditional posterosuperior cholesteatomas, which are more easily diagnosed on CT by an expansile soft-tissue mass. In contrast, IICs reveal erosion/abnormality of the ossicular chain with no soft-tissue mass on CT scan. The lack of significant otologic history among all patients as well as a fully intact, normal tympanic membrane on examination make the possibility of microscopic congenital, keratinous abnormality with later growth the most likely pathophysiologic mechanism, although the etiology cannot be confirmed with complete certainty.
Presentation and Symptomatology
Reports in the literature suggest that congenital cholesteatomas present on average around 4 to 5 years of age, 13 -15 with Gilberto et al 11 more recently reporting 6.58 years in a meta-analysis of 1469 congenital cholesteatomas. One case report describes a presumed IIC diagnosis in a 28-year-old with similar imaging and clinical features to those in our study. 16 The 5 patients described here presented between 5.5 and 16.0 years (average of 10.7 years), showing that IICs may have a slightly later age of presentation with a wide age range that includes young adults. This can be due to the paucity of symptoms and normal examination, which can delay the diagnosis. Congenital cholesteatomas tend to demonstrate a male predominance of approximately 3:1. 11,13,15,17 The cases reviewed here did not mirror that pattern (3/5 female), but the relatively small sample size makes it difficult to draw formative conclusions about the gender representation in IICs. Similarly, the right-sided predominance seen in this series (4/5 patients) is unlikely to reflect any true laterality predilection.
All of the patients in this series presented with unilateral moderate-to-severe conductive hearing loss with normal otoscopy (1 also reported intermittent tinnitus). In most recent congenital cholesteatoma case series (eg, Cho et al or Mostafa et al) as well as meta-analyses (Gilberto et al), authors note that the diagnosis is most commonly incidental, although patients can present with hearing loss, discharge, or facial paralysis and have a history of otitis media. 11,17 -19 Because the ossicular chain is affected early in the pathologic progression, damage to the ossicles and subsequent hearing loss may be the first indicators of IIC. Newly diagnosed isolated hearing loss in children with unremarkable audiologic history and normal otoscopy, combined with a CT scan showing abnormalities and discontinuity of the ossicular chain, should alert physicians to the possibility of this diagnosis. 16
The CT scans were critical in guiding the diagnosis for all patients in this series. Despite the subtlety in identifying ossicular abnormalities, CT scans remain the imaging study of choice for investigating conductive hearing loss when other etiologies have been ruled out. 20 Here, imaging revealed various levels of dysmorphology/erosion of the incus and stapes in all patients, some with the appearance of absent stapes superstructure and/or absence of the long process of the incus. Although this can be characteristic of congenital ossicular malformation, all patients had previously passed hearing tests at school or via their primary care physician. The erosion or dysmorphology of the incus and/or stapes helps explain the isolated symptom of unilateral hearing loss seen in this patient series. A defining feature of IIC seems to be the conspicuous lack of soft-tissue mass usually seen in other congenital cholesteatomas. Instead, IIC presents with a thin cholesteatoma, which erodes the ossicular chain but is not obvious on CT scan. To rule out a congenital cholesteatoma, physicians should recommend a middle ear exploration in pediatric patients with this clinical history, examination, and imaging findings.
Surgical Treatment and Outcomes
All patients underwent endoscopic middle ear exploration via the transmeatal approach. Ossicular chain reconstruction was performed in 4 of 5 patients, and 1 patient has yet to undergo second-look and ossicular chain reconstruction. Surgical approaches for cholesteatomas have always varied based on the location and extent of the lesion. 21 As described in Nelson et al, 19 when the lesion involves the posterosuperior quadrant, the operation is often a canal wall up tympanomastoidectomy followed by a second look for lesion control. However, this description refers more to lesions that have extended into the mastoid, rather than to the small lesions that originate in the incudostapedial location. Isolated incudostapedial cholesteatomas can be easily treated by a transmeatal endoscopic approach, as the disease is small. This approach offers excellent visualization and complete removal of the IIC, which allows for the ossicular chain reconstruction during the same surgery in most cases. This approach worked well for all patients, except for one who experienced an extrusion of the total ossicular replacement prosthesis. Postoperative audiogram outcomes in patients appear promising, with 3 of 4 showing substantial improvement in hearing (and 1 patient yet to undergo ossiculoplasty). Future research can help determine characteristics that portend a favorable outcome after reconstruction as well as the nature of recurrence with this diagnosis.
Embryologic Origin
The rare anatomical location of these lesions makes the origin of IICs uncertain. Without significant otologic history and no sign of previous perforation or retraction pocket of the tympanic membrane, acquired disease is less likely. It has been experimentally shown in mice that the middle ear epithelia have a dual origin. 8 The epithelia of the auditory tube, together with the epithelium covering the auditory bulla and the lateral areas of the middle ear, derive from the endodermal epithelium of the first pharyngeal pouch. 8,9,22 However, the rest of the epithelium covering the middle ear cavity is of neural crest origin. 8,9 Errors in either the mesenchymal-to-epithelial transition during mesenchyme resorption or disruptions in the union of the 2 tissue types offer possible explanations for a nidus of cholesteatoma seen at the stapes, incus, and incudostapedial junction. However, the precise origin remains uncertain and further research is needed to clarify.
Strengths, Limitations, and Future Directions
This study uniquely details the presentation, imaging characteristics, surgical treatment, and functional audiologic outcomes specific to patients diagnosed with IIC. Although posterior cholesteatomas have been more frequently reported in recent literature, this study details the findings and clinical course of IIC and provides a hypothesis as to its pathologic origin. The biggest limitation of this study is the small number of patients with this diagnosis. In the future, we hope to have a more extended follow-up of clinical outcomes.
Conclusion
Isolated incudostapedial cholesteatoma is a unique presentation of cholesteatoma that, due to their specific anatomic location of destruction, can present with the isolated finding of unilateral conductive hearing loss. Physicians should keep this diagnosis in mind when a pediatric patient presents with new unilateral conductive hearing loss, normal otoscopy, noncontributory otologic history, and a CT scan showing disruption of the ossicular chain with no expansile soft-tissue mass. Better understanding of this pathologic variation can promote earlier diagnosis and accurate counseling as well as treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.