
Abstract
Lipomas are benign and slow-growing neoplasms that typically develop in the subcutaneous tissue. They rarely occur in the upper aerodigestive tract. Oropharyngeal lipomas are rare. They represent 0.5% of all neoplasms of the head and neck. We present a case of a 43-year-old female with a polypoid mass in the base of the left palatine tonsil. The patient underwent a left tonsillectomy and a resection of the mass. The pathological diagnosis was tonsillar lipoma. We describe the clinical characteristics and the management of this rare case. Palatine tonsillar lipoma is a rare benign tumor with an unusual recurrence rate, and an excellent prognosis.
Case Report
A 43-year-old female, with any particular history, has consulted for dysphagia evolved over 2 months. She is neither an alcohol nor tobacco consumer. On examination, a regular and polypoid mass about 1 cm × 1.5 cm was noted in the oropharynx. On indirect laryngoscopy, the mass was pedicled to the base of the left palatine tonsil.
Computed tomography (CT) scan showed a regular mass at the base of the left palatine tonsil with fat density [−21 Hounsfield (HU) units] and with no contrast enhancement. Its measures 10 mm × 8 mm × 10 mm (Figure 1). This lipoma protrudes into the oropharynx, maintaining a distance from the base of the tongue, as well as from the epiglottis, aryepiglottic fold, and vallecula.
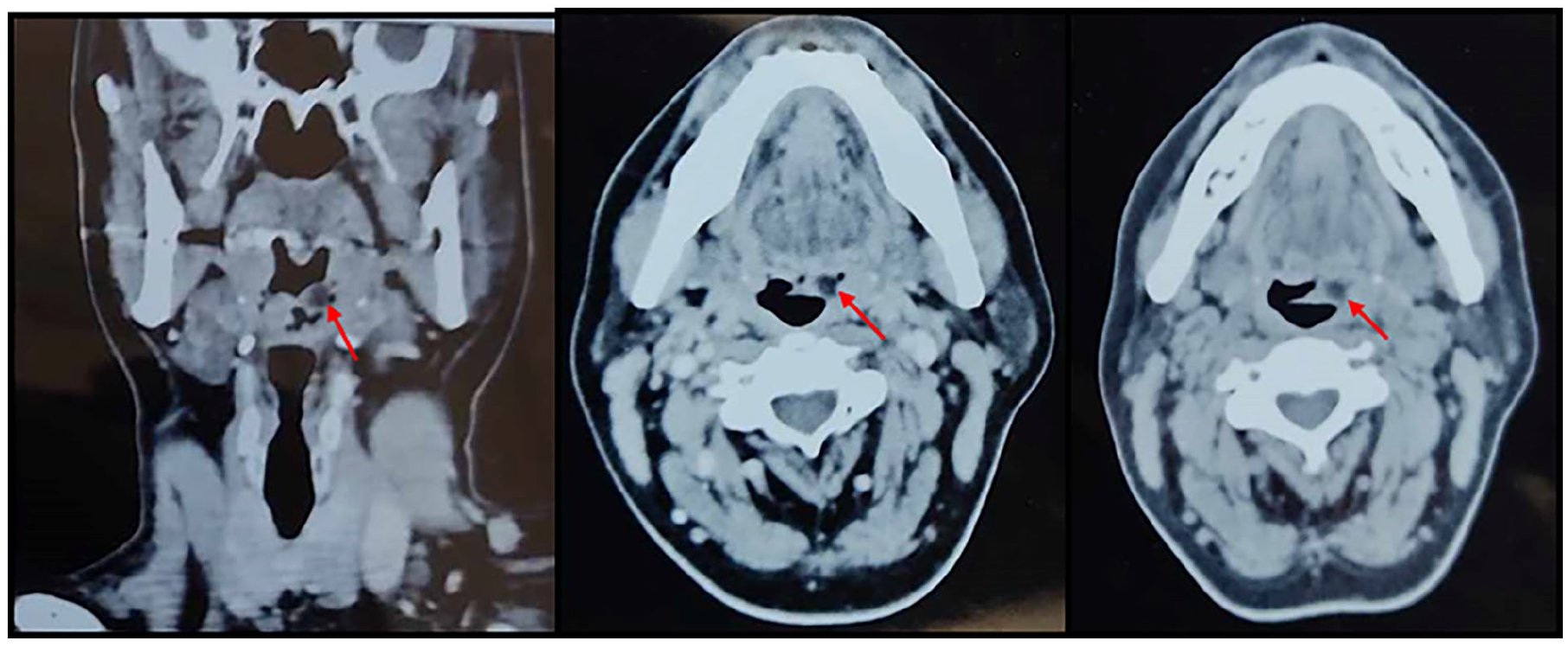
Enhanced CT scan showing a mass on the left side of the oropharynx (red arrow) and attached to the surface of the left tonsil. No obvious enhancement was found. The mass exhibited an enhancement value of −21 Hounsfield units.
The patient underwent a left tonsillectomy and a resection of the mass (Figure 2). The surgery proceeded smoothly without any notable incidents.

Bilateral tonsils were enlarged in degree II enlargement, and the mass (blue arrow) arising from the base of the left tonsil palatine.
The histopathological examination revealed fibro-angio-lipoma of the oropharynx. The lesion exhibits a polypoid appearance covered by acanthotic and keratotic squamous epithelium. The core of the polyp consists of a proliferation of ectatic vessels with thin walls, surrounded by abundant connective tissue associated with a regular adipocytic component.
The palatine tonsil was without anomalies and no signs of malignancy was observed.
After 1 year follow-up, no evidence of recurrence was noted.
Discussion
Lipomas are benign tumors composed of an abnormal collection of mature adipose cells. 1 They typically manifest in subcutaneous tissues but are infrequent in the aerodigestive tract. Lipomas of the tonsillar/oropharyngeal space are very rare with only few cases described in literature and their overall incidence is between 1% and 4.4% of all benign oral lesions.1,2 Benign tumors of the palatine tonsil are rare, comprising approximately 25%, while malignant tumors constitute 75% of palatine tonsil tumors.1,3
Although malignant transformation is infrequent, degeneration in larger sized lipomas is described.4,5
The etiopathogenesis of oropharyngeal lipomas is not yet clear.1,4 Trauma, hereditary, fatty degeneration, infection, infarction, and chronic irritation can lead to their development.1,4
These tumors can occur in individuals at various ages. 3 They typically manifest in patients after 30 years of age, although they may also be congenital. 2 The clinical presentation of oropharyngeal lipoma is variable and it is typically discovered incidentally. 6 Depending on their location, lipomas can pose life-threatening risks. 2 They can present as a painful or painless mass that can lead to dyspnea our sleep apnea. It can manifest as cough, foreign body sensation, dysphagia, dysphonia, or angina.4,6 Our patient had dysphagia.
Tonsillar lipomas predominantly originate from the body of the tonsil but can also develop from the inferior pole as well as the peritonsillar space. 6
Imaging plays an important role in the diagnosis and evaluation of oropharyngeal lipomas and provide important information for treatment planning. 5 The CT scan can diagnose a lipoma due to its typical characteristic feature, homogeneous, nonenhancement, and low attenuation measuring between 65 and 125 HU. 2 Magnetic resonance imaging (MRI) is better than CT because of its excellent resolution in studying soft tissues and tumor extension. 2
The definitive and exact diagnosis of oropharyngeal lipoma relies on histological examination. 3 Lipomas can be categorized based on additional mesenchymal elements integral to the tumor. 6 The various variants include fibrolipomas, myxoid lipoma, angiolipoma, angiomyolipoma, spindle cell lipoma, chondroid lipoma, myolipoma, chondrolipoma, and osteolipoma with fibrolipomas. 6 It is characterized by mature adipocytes with fibrovascular connective tissue septae, along with tonsillar lymphoid tissue at the periphery (stained with hematoxylin and eosin). 3 Benign lesions are positive for S100 and negative for MDM2. 4
Surgical resection is the baseline treatment for lipomas of the oropharynx. Concerning tonsillar lipoma, tonsillectomy with the excision of the lesion has been described as the most common treatment option, while surgical excision of the lipoma, without tonsillectomy, has rarely been described in the literature.6,7 For lipomas located elsewhere in the oropharyngeal region, the extent of the procedure depends on the size and specific location of the tumor. 2 Endoscopic removal is recommended, although for larger masses, an external approach may be necessary. 2 A transoral approach is preferable to the external approach due to the typically well-encapsulated nature of lipomas, allowing for complete excision to be achieved. 8 Various techniques have been employed for transoral resection, including cold dissection and resection, monopolar resection, mechanical stapler, and laser excision. 5
Conclusion
Oropharyngeal lipoma is a rare and benign tumor. Surgical resection is the reference treatment due to the potential risk of airway obstruction and malignant transformation.
Footnotes
Acknowledgements
All authors: Approved the final version and have the agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy
Author Contributions
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases.
Consent for Publication
Written informed consent to publish the patient’s clinical details and clinical images was obtained from the patient.