
Abstract
A 73-year-old woman having a throat lump sensation and dysphagia for the past several months presented at our otorhinolaryngology outpatient clinic. A physical examination disclosed a protruding subepithelial mass over the right tonsil fossa. The mass was not tender and had no mucosal lesions or signs of active infection. Therefore, we arranged face and neck computed tomography scans, which reported a solitary osseous lesion over the anterior-right aspect of the C1-2 joint. Considering the rarity and unfamiliar anatomy of this disease, we built a 3D-printed model to assist with the surgical rehearsal of the procedure as well as with a preoperation discussion with the patient and her family. We arranged a combined Otolaryngology-Neurosurgery department approach after discussion with the neurosurgeon and successfully removed the lesion without sacrificing the overlying longus capitis muscle. The pathology examination revealed no evidence of malignancy. The final diagnosis was cervical spine solitary osteochondroma. The patient had a complete recovery of both oral cavity and normal swallowing function. No tumor recurred during the 3-year follow-up. On the basis of this case, in-house 3D-printing technology can offer a rapid, reliable model for an interdisciplinary team to use to enhance personalized presurgical planning, thus providing better patient engagement during hospitalization.
Introduction
Osteochondroma, which constitutes 20% to 50% 1 of benign bone tumors, typically presents as a nontender, painless, cosmetic deformity related to a slowly enlarging exophytic mass. These tumors are prominent in males, with most diagnosed during the 20s to 30s and affecting the long bones. Involvement of the spine is rare. 2,3
Cervical osteochondromas have been reported to arise anywhere from C1 to C7 and cause a variety of symptoms, including vocal palsy, neck mass, and compression myelopathy. 2 -4 Here, we report a case of an elderly woman with a cervical spine, solitary osteochondroma who underwent transoral-approach tumor excision with the assistance of 3D printing. This new in-house technology provided a rapid and accountable 3D model of an osseous tumor occurring in an unconventional anatomical area. By demonstrating the model to medical staff, we can improve the quality of presurgical planning and surgical approach selection.
Case Report
A 73-year-old woman with a history of hypertension and diabetes mellitus having a throat lump sensation and swallowing difficulty for the past several months presented at our otorhinolaryngology outpatient clinic. On physical examination, we noted a posterior-right, oropharynx, smooth, nontender, and bulging mass and initially suspected a tonsil tumor (Figure 1). However, the head and neck computed tomography (CT) revealed a large, osseous lesion without an adjacent soft tissue enhanced mass in the anterior-right aspect of the C1-2 joint about 3 cm in size (Figure 2). Therefore, we consulted a neurosurgeon.

A nontender, bulging mass over the posterior-right oropharynx.
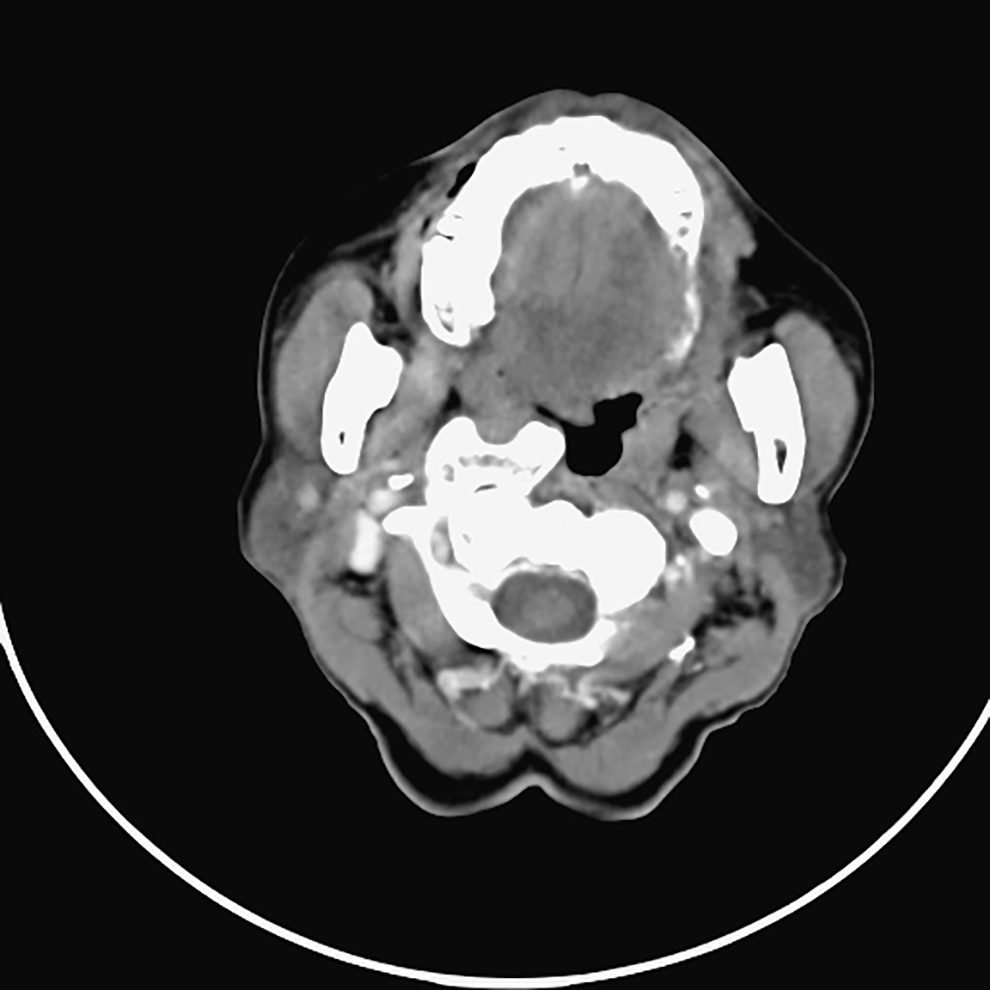
Head and neck computed tomography (CT) revealed a large osseous lesion without an adjacent soft tissue enhanced mass in the anterior-right aspect of the C1-2 joint, with a size about 3 cm.
The C-spine magnetic resonance imaging (MRI) reported a large, solitary osseous or osteochondral body. The patient had no history of prior C-spine trauma or surgery. Considering the rare presentation of this mass, we built a 3D-printed model of the spine and osseous tumor that demonstrated a potentially distorted longus colli or longus capitis muscle (Figure 3).
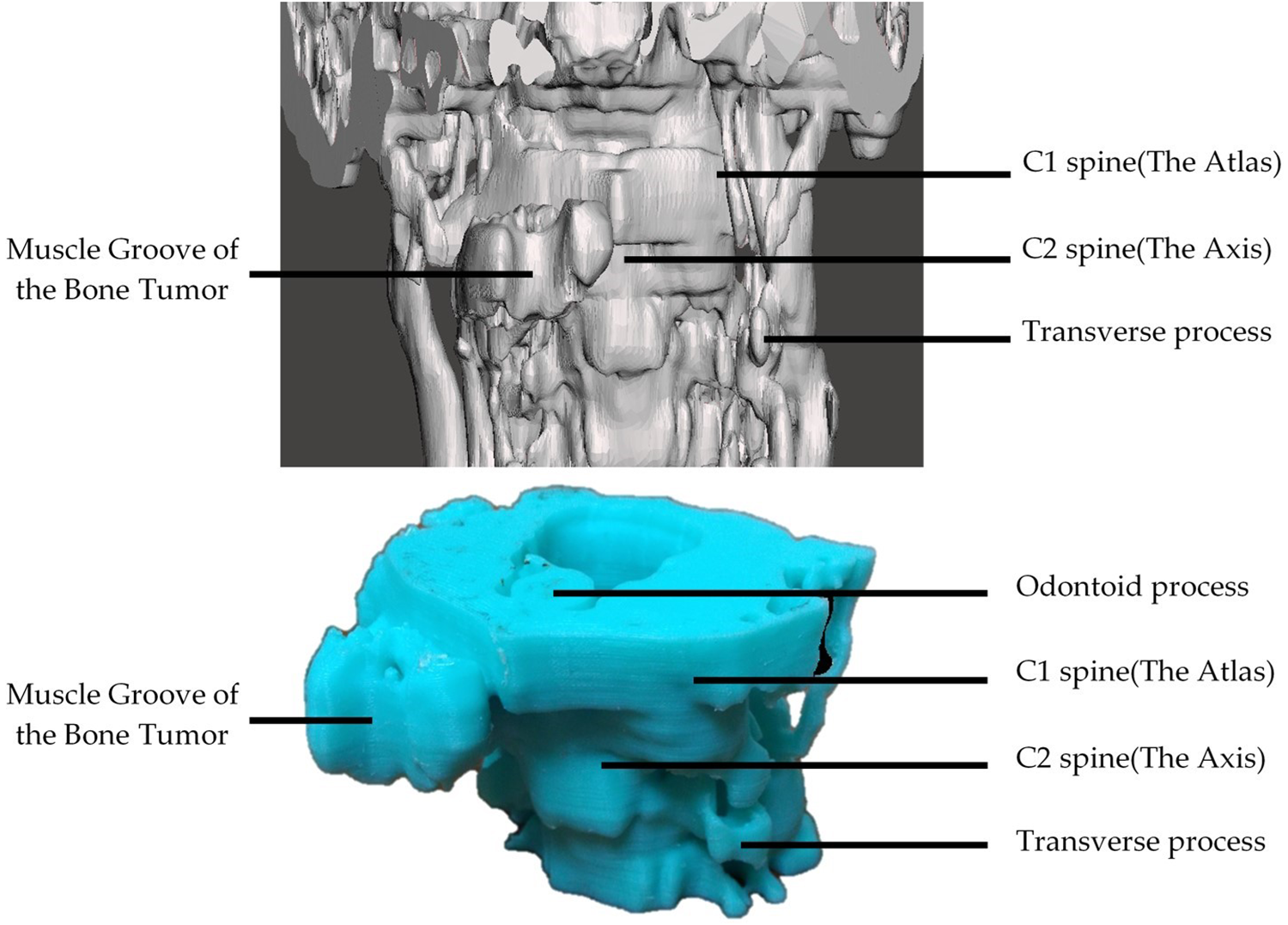
3D-printed model of the spine and osseous tumor demonstrating a potentially distorted longus colli or longus capitis muscle.
We obtained anatomical data from head and neck CT scans with contrast medium, thickness 5 mm, and output as Digital Imaging and Communications in Medicine images. We loaded these images into InVesalius 3.0 (Centro de Tecnologia da Informação Renato Archer; freely available on the Internet) for manual segmentation of the bone and desired tumor part and for output as a single-layer mesh. We then saved the mesh as binary stereolithography (STL) file.
We imported the STL files into the Autodesk Meshmixer software (Autodesk Inc) for further manipulation before printing and loaded them into Kisslicer 1.5, a cross-platform online freeware that generates path information (G-code) from STL, for further fabrication with a D-force 300 V2 3D printer with 1.75-mm polylactic acid. Total printing time was around 3 hours.
Comparing the CT image and intraoperative findings (Figures 4 and 5), the alignment and configuration of the 3D-printed model was highly similar to the actual tumor. The model facilitated more precise surgical planning and treatment strategies among the otolaryngologist, neurosurgeon, and radiologists. Thus, we arranged the transoral removal of the osseous tumor using microscopy and neuronavigation.

The in-office 3D-printed model was highly similar to the actual tumor when compared with the computed tomography (CT) image (sagittal view).
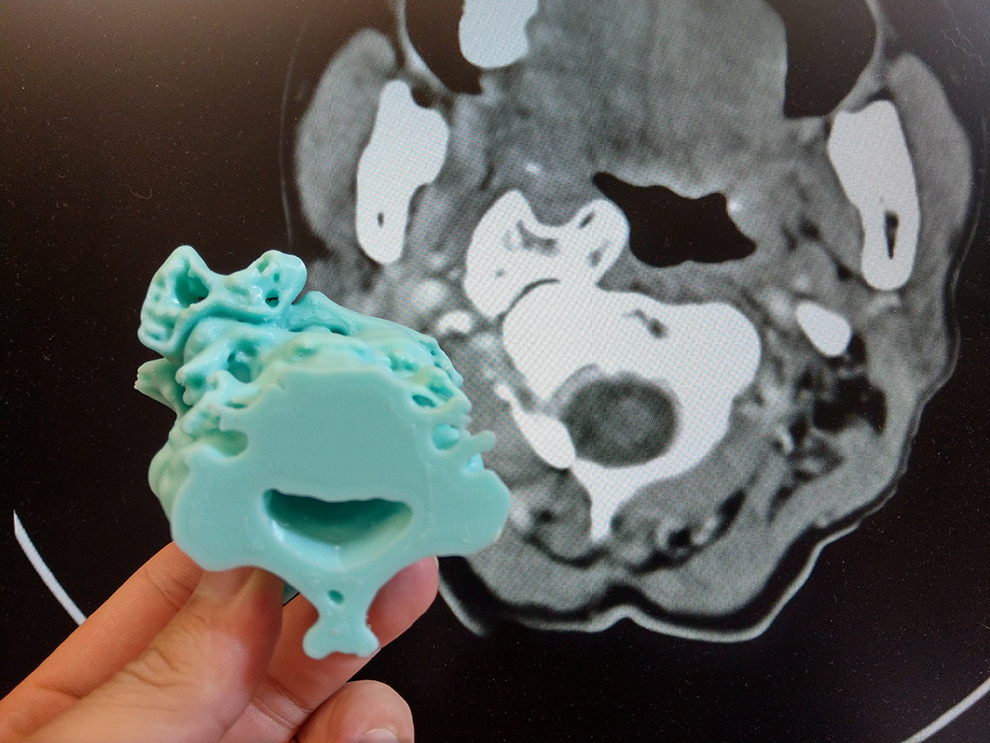
The in-office 3D-printed model was highly similar to the actual tumor when compared with the computed tomography (CT) image (coronal view).
During the surgery, the mucosa of the posterior oropharynx covering the tumor was incised vertically to expose the tumor mass. The right longus capitis was dissected from the tumor toward the lateral side. The osseous tumor mass was removed piece by piece with a high-speed drill and Kerrison rongeur or other disc rongeur under microscopy. After removal of the medial part of the mass, the right longus capitis was dissected toward the medial side to expose the lateral part of the tumor (Figure 6). We also removed the residual tumor piece by piece under microscopy. The pathology examination revealed no evidence of malignancy. The final diagnosis was cervical spine solitary osteochondroma.
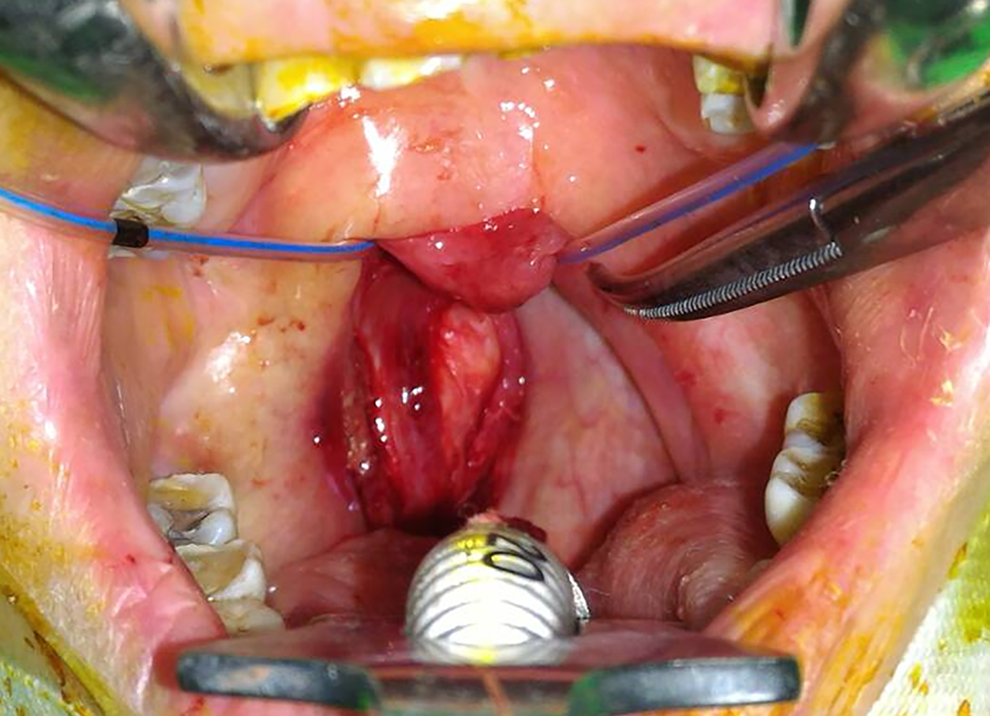
After removal of the medial part of the tumor mass. The right longus capitis was dissected toward the medial side to expose the lateral part of the tumor.
After 1 month of an uneventful recovery, the patient had no residual sensory defects, swallowing dysfunction, lumping, or obstructive sensation. The MRI image 6 months after surgery revealed no local recurrence (Figure 7). The patient encountered neither recurrence nor any complications during her 3-year, outpatient-clinic, follow-up visits.
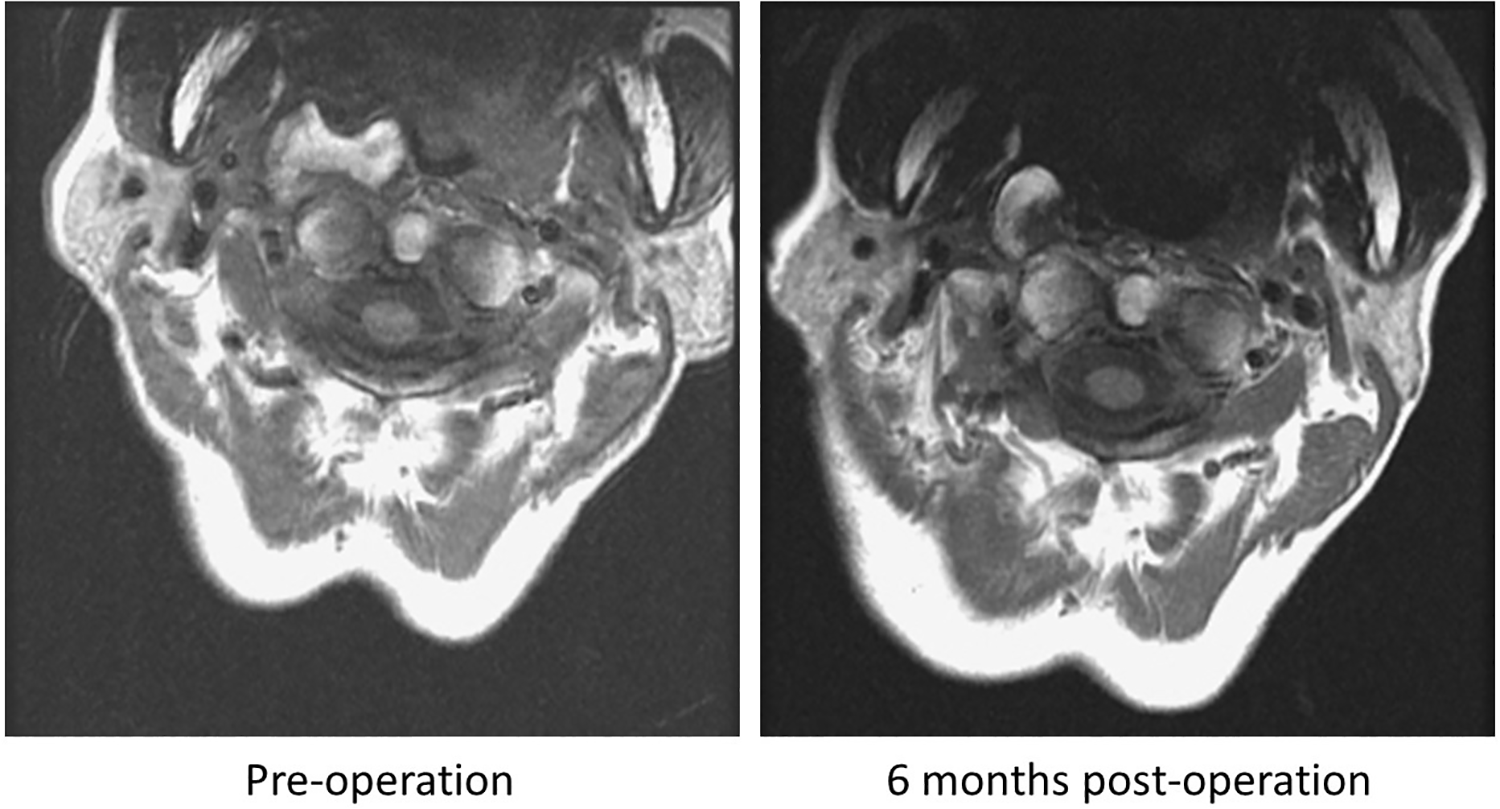
No local recurrence was noted between the preoperative and 6-month postoperative magnetic resonance imaging (MRI) T1 images.
Discussion
Osteochondroma constitutes 10% to 15% of all bone tumors 5 and 20% to 50% 1 of benign bone tumors. These tumors are predominant in males, and most are diagnosed during the 20s to 30s, with mostly affecting the long bones, particularly the femur and tibia. Osteochondroma tumors can be solitary or multiple and are part of an autosomal dominant inheritance disorder known as hereditary multiple exostoses. 3 Spine involvement for solitary osteochondroma is rare, with an incidence of 1.3% to 4.1%. Cervical spine origin is more common (50%) among all spinal osteochondromas, with C2 being the most frequently involved level, followed by C3 and C6. 5
Spinal osteochondromas can be classified into anterior (vertebral body) or posterior (pedicles, lamina, spinous process) types according to the affecting element of the vertebrae, with mostly arising from the posterior elements. Posterior cervical spine osteochondromas usually are asymptomatic but rarely can cause compressive myelopathy, 2 radiculopathy, or torticollis. 6 Anterior cervical spine osteochondromas can cause dysphagia, sleep apnea, respiratory distress, vocal cord paralysis, or Horner syndrome or can present as a pharyngeal mass, as in our patient case. 4,7,8
Asymptomatic lesions can be followed up conservatively. 9 However, resection surgery is preferred if the lesion is symptomatic or if the diagnosis is not definite. Complete excision of the cartilage cap is recommended to avoid recurrence, which occurs in 2% to 5% of lesions, with a mean recurrence time of 5 years. 10,11
Plain radiography is useful to diagnose osteochondromas of the extremities. 1 However, osteochondromas arising from the spine are difficult to diagnose by this method and clinical features alone because of the complicated anatomy of the spine. Because our case presented with a smooth, nontender, bulging mass over the posterior-right oropharynx, it was reasonable for our initial impression to be a tonsil tumor.
Computed tomography and MRI can provide a better evaluation for spinal osteochondromas. 12 Computed tomography can reveal the precise localization of cartilaginous and bony parts of the tumor and show its relationship to the vertebral and intervertebral foramen. 12 Magnetic resonance imaging enables a better evaluation of the spinal cord, nerve root, or adjacent soft tissues. 12 Considering the unconventional location of the osteochondroma in our case and the necessity of en bloc resection to prevent recurrence, we applied 3D-printing technology to assist in the surgical planning for its transoral resection. 1,2
The role of 3D-printing applications in the ENT field is emerging, including building auricular reconstruction frameworks, treating severe tracheomalacia, reconstructing complex tracheal, creating patient-specific mandible templates, performing endoscopic sinus or skull base surgeries, and even evaluating prenatal congenital airway obstruction. 13 -17 Preoperative uses include demonstrating potential anatomy structures, enabling more accurate surgical planning, and educating patients, their families, and other staff about the procedures. It can also be sterilized for intraoperative surgical manipulation.
In this case report, we used a rapid, reliable 3D-printing model to assist with performing a transoral resection of a tumor occurring over an unconventional and complex anatomy area. This in-house technology can offer a direct view of different approaches and personalized presurgical planning, facilitate communication among the interdisciplinary team, and provide better patient safety and engagement during surgery and hospitalization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.