
Abstract
Introduction
Sinonasal malignant melanoma (SMM) is a type of malignant melanoma that occurs in the head and neck. It has a low incidence, high malignancy degree, rapid development, wide invasion, easy metastasis, and local recurrence.1,2 The symptoms are atypical, making early diagnosis challenging. At the time of diagnosis, the cancer is often in the middle and late stages, making complete surgical resection difficult. Due to the complex anatomy of the tissues and organs surrounding the nasal cavity and sinuses, the treatment is relatively challenging, and the prognosis is poor. 3 In the past, traditional surgical resection methods like lateral nasal incision or maxillary resection were utilized for tumor removal, along with comprehensive treatments like radiotherapy and/or chemotherapy. 4 The average 5 year disease-free survival rate was approximately 26%, 5 and the curative effect was unsatisfactory. In recent years, nasal endoscopic skull base surgery has been widely used in clinical practice, representing a significant advancement compared to traditional treatment approaches. The visual field under the endoscope is clear and magnified, making it convenient to locate the primary site and invasion range of the tumor during the operation. This clarity is conducive to completely resecting the tumor while preserving the surrounding tissues and organs as much as possible, resulting in a good curative effect.6,7 In this study, the clinical records of 47 patients with SMM were retrospectively analyzed to explore the application of endoscope-assisted tumor resection in the traditional surgical treatment of SMM. This study aimed to leverage the benefits of both techniques and offer valuable clinical insights for achieving maximal tumor removal.
Materials and Methods
General Information
The study was conducted at the Department of Otorhinolaryngology—Head and Neck Surgery at the Third People’s Hospital of Yunnan Province. In studies involving human participants, all procedures complied with the ethical standards of the institutional and/or national research committees, the 1964 Declaration of Helsinki, its later amendments, or similar ethical standards. The study was approved by the review board of the Third People’s Hospital of Yunnan Province (202001BA070001-079). The clinical data of 47 patients with SMM admitted from October 2000 to June 2020 were retrospectively analyzed. The ages ranged from 32 to 74 years, with an average age of 56.2 ± 9.2 years, including 28 males and 19 females. All the lesions were mainly located in the unilateral nasal cavity and sinuses. Computed tomography (CT) scans revealed positive cervical lymph node metastasis in level II and III in 4 cases.
Clinical Signs and Symptoms
The main symptoms of the patients included varying degrees of unilateral nasal obstruction, blood in the nasal discharge, facial swelling and pain, and hyposmia. Among the patients in this study, 21 cases originated in the nasal cavity (9 cases in the middle meatus, 5 cases in the nasal septum, 5 cases in the inferior turbinate, and 2 cases in the nasal roof), and 16 cases originated in the sinuses (9 cases in the ethmoid sinus, 4 cases in the floor of the frontal sinus, and 3 cases in the sphenoid sinus). The tumor invaded the maxillary bone in 7 cases and extended to the orbital fascia in 4 cases. Four cases had a history of surgery for nasal polyps, and the postoperative pathological diagnosis confirmed nasal polyps.
Pathological Examination
All patients underwent pathological examination, and multiple immunohistochemical markers were assessed in conjunction with clinical manifestations, imaging examinations, and pathological findings to confirm the diagnosis. The commonly used immunohistochemical markers were HMB45, melan-A, S-100, and Ki67. 8
Surgical Treatment
The SMM patients selected for surgery had tumors confined to the nasal cavity and paranasal sinuses, with or without local surrounding invasion (such as the orbit or skull base), without extensive skull base, intracranial, or extranasal invasion and destruction, and without distant metastasis. They may or may not have had cervical lymph node metastasis and were able to tolerate surgery. All patients underwent surgery under general anesthesia. According to the American Joint Committee on Cancer (AJCC) 2010 edition SMM staging system 9 and the location of the lesion, different surgical methods were employed based on the tumor’s location and extent. Doctors in the same surgical group were randomly divided into 2 groups, the traditional surgery group (direct vision, no microscope), and the endoscope-assisted traditional surgery group, based on surgical methods.
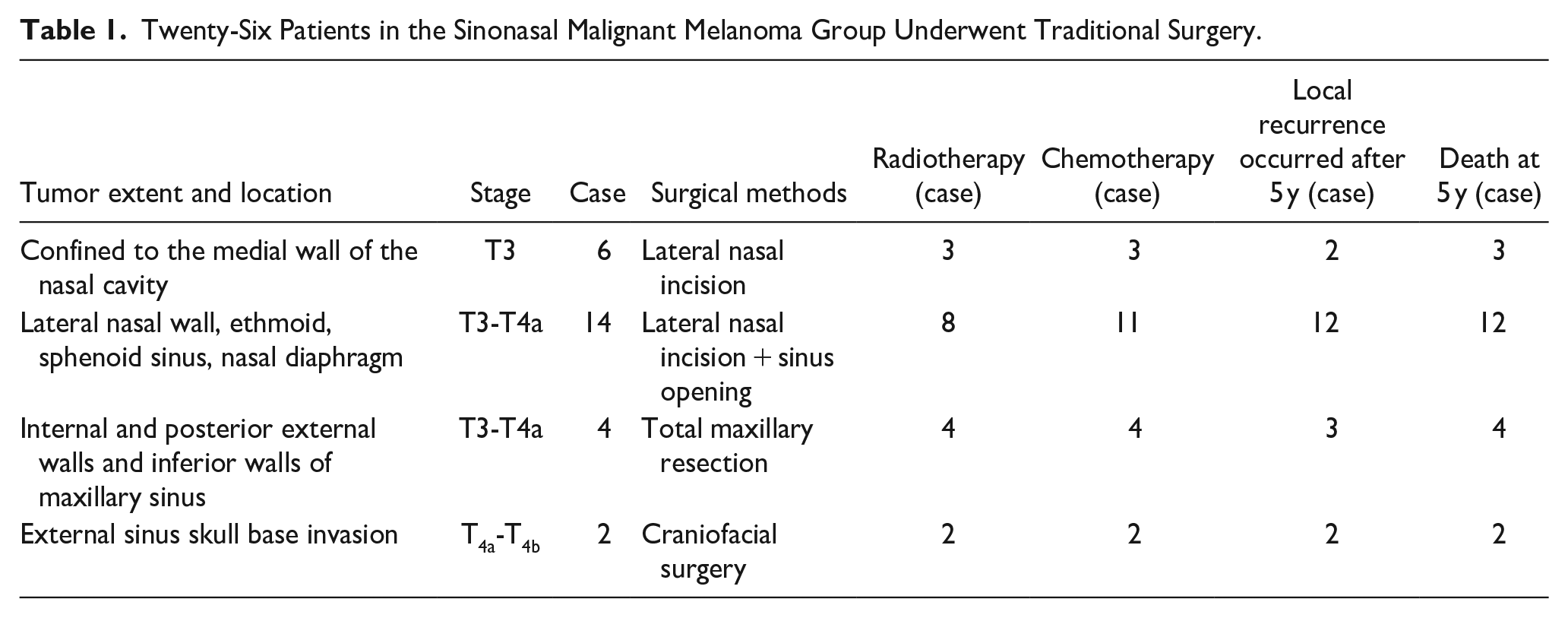
In the traditional surgery group: 6 cases confined to the medial wall of the nasal cavity; 14 cases located in the medial wall of the nasal cavity, ethmoid sinus, sphenoid sinus, and nasal septum (T3-T4a) were treated with traditional or flexible lateral rhinotomy; 4 cases located in the inner, posterolateral, and inferior wall of the maxillary sinus (T3-T4a) underwent maxillary or extended resection; 2 cases with external skull base invasion of the paranasal sinuses (T4b) underwent nasal incision combined with craniofacial neurosurgery. In all patients, the tumor was removed while ensuring a safe margin, and any suspicious tissue was excised and frozen during the operation. After the negative margin was identified, the wound was repaired, and the operation was successfully completed. The distance from the tumor margin was 1.5 to 2.0 cm, and the deep part, including muscle, mucosa, and muscle, was resected together. If there was bone destruction, extensive bone resection was performed. 10 Four cases of T4a underwent neck dissection.
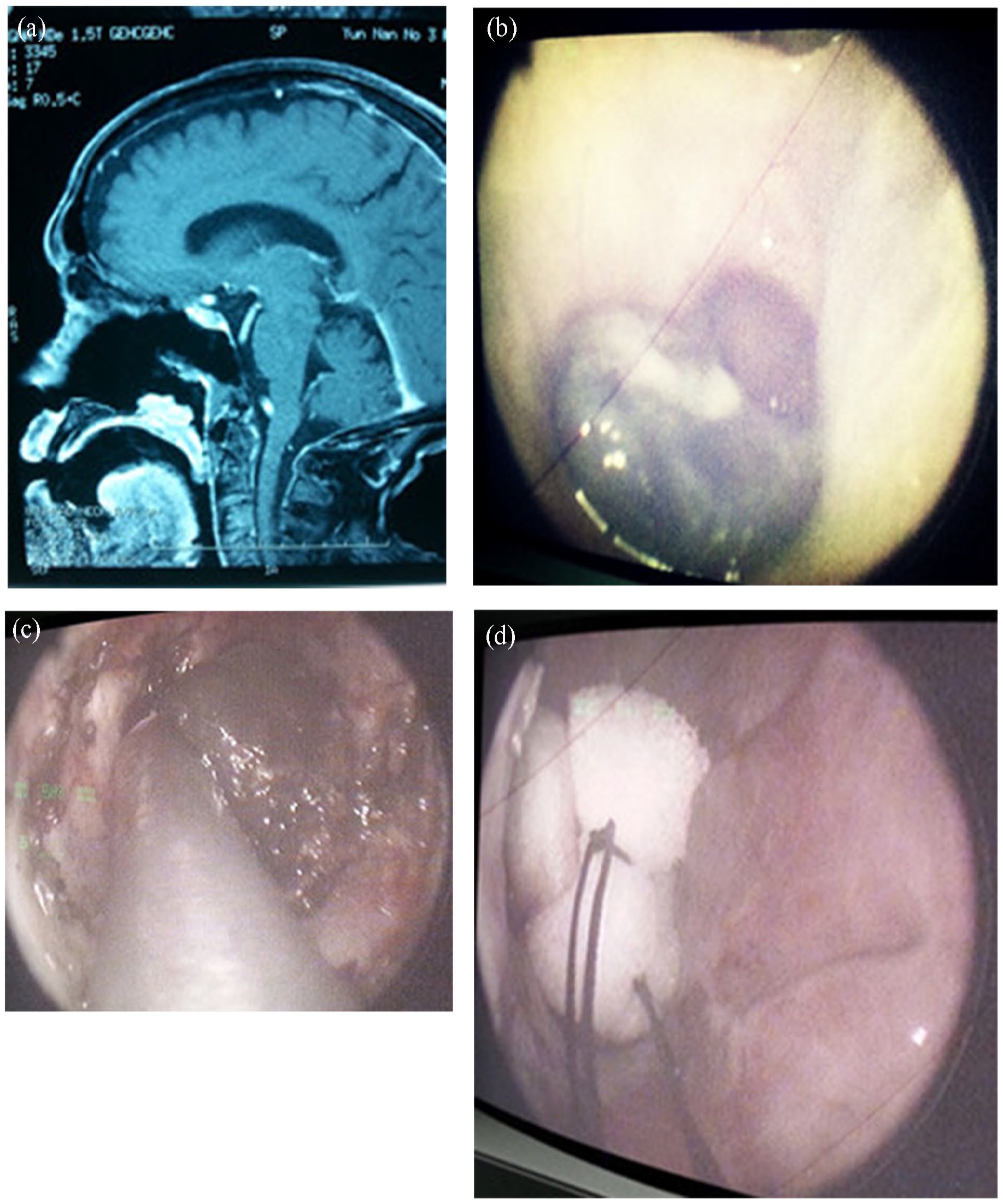
In the endoscope-assisted traditional surgery group, traditional surgery was performed first based on the tumor’s location (4 cases of lateral nasal incision, 13 cases of lateral nasal incision or sinus opening, 3 cases of total maxillary resection, 1 case of external skull base invasion of paranasal sinuses, and craniofacial surgery). After the excision of large tumors in the aforementioned cases, the hidden deep parts of the middle nasal meatus, the superior nasal meatus, olfactory cleft, ethmoid roof lamina cribrosa, pterygopalatine fossa, nasopharynx, frontal recess, orbital lamina, and orbital fascia were meticulously observed and treated using bright vision through the nasal endoscope. If there was a mass, further resection and polishing were performed, and the necessary repairs were carried out. Four cases limited to the medial wall of the nasal cavity underwent a simple endoscopic resection. Neck dissection was performed in 4 T4a cases. Figures 1 and 2 show surgical images of 2 cases where traditional surgery was combined with nasal endoscopic techniques.
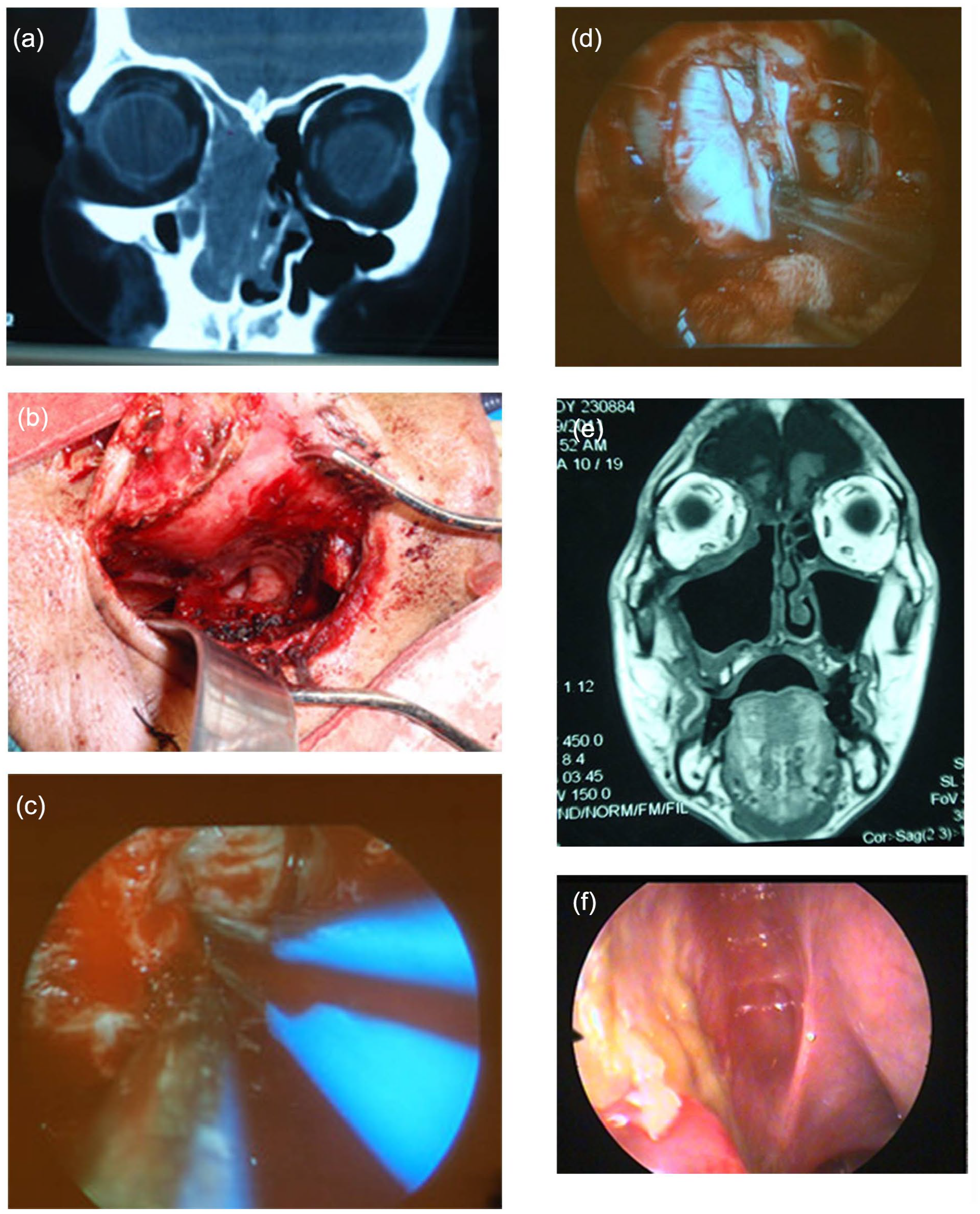
T3 sinonasal malignant melanoma (traditional lateral rhinotomy combined with nasal endoscopic technique and skull base repair). (a) Preoperative CT scan. (b) Lateral rhinotomy procedure. (c) Skull base defect on the ethmoid roof during endoscopic surgery. (d) Reconstruction of the skull base defect under a microscope. (e) MRI scan at 3 months post-surgery. (f) Internal view of the skull base post-surgery. CT, computed tomography; MRI, magnetic resonance imaging.
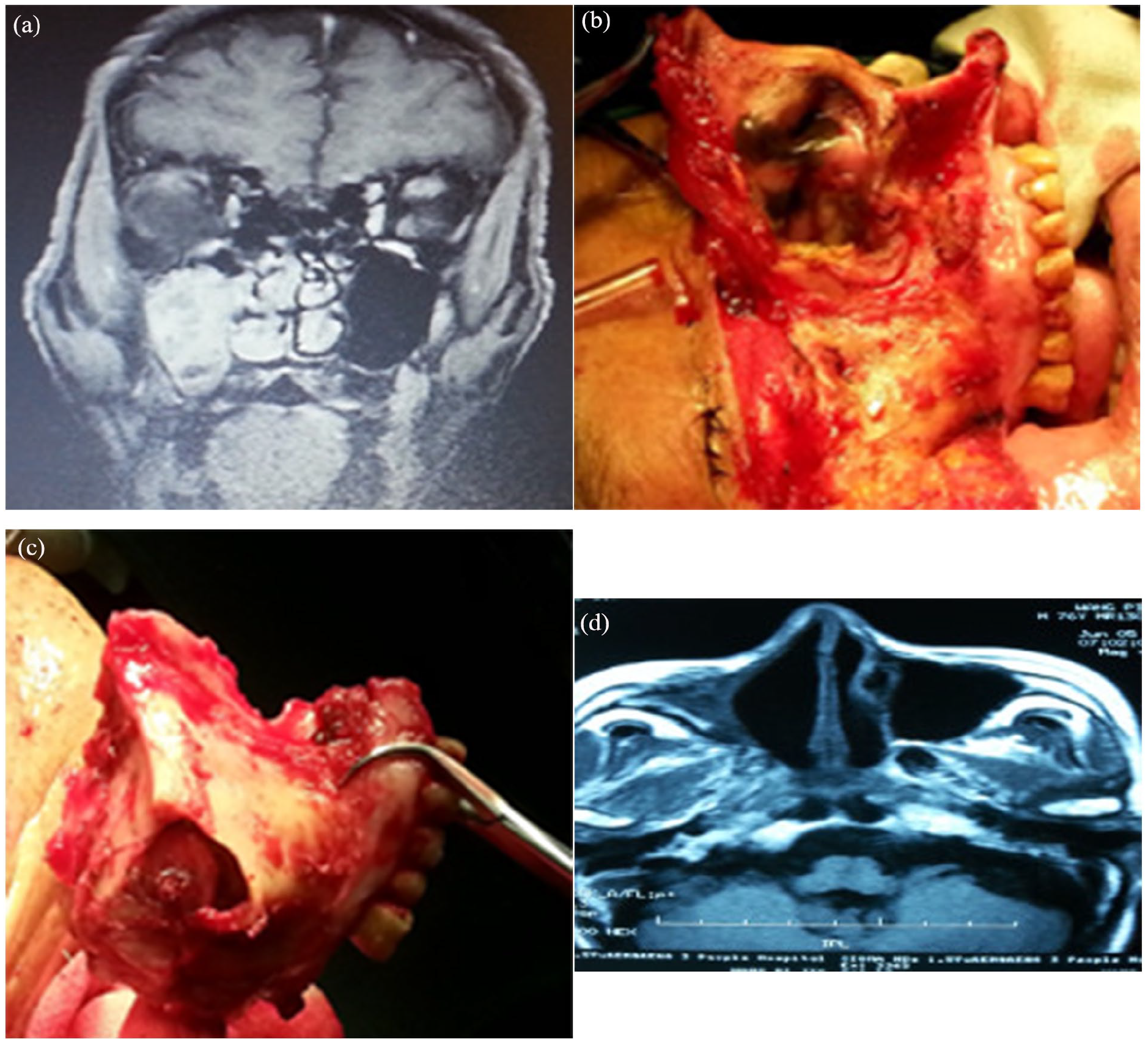
Sinonasal malignant melanoma in the maxillary sinus and nasal cavity (maxillectomy combined with nasal endoscopic technique). (a) Preoperative MRI. (b) Condition of lesions during the operation. (c) The maxilla and tumor were removed. (d) MRI was performed 6 months after the surgery. MRI, magnetic resonance imaging.
After surgery, some patients received adjuvant radiotherapy, chemotherapy, and immunotherapy. In the traditional group, 20 patients received postoperative chemotherapy and biological therapy, while 17 patients received radiotherapy. In the endoscopic-assisted group, 18 patients received postoperative chemotherapy and biological therapy, while 15 patients underwent radiotherapy with a total dose of >50 Gy/6 to 7 weeks. The most common chemotherapy regimen involved administering azenamine at a dose of 250 mg/m2 through intravenous infusion of chloroethonide or cyclohexonide. Interferon 300,000 to 600,000 units should be used 5 to 10 times.
Statistical Methods
SPSS 13.0 software was used to analyze the statistical data, and the chi-square test was employed to analyze the count data. The statistical results showed that P < .05, indicating a significant difference.
Results
Results of Pathological Examination
The results of the pathological examination and immunohistochemistry showed that all 47 patients in this study had malignant melanoma, with 3 cases being nonpigmented malignant melanoma. Figure 3 displays the immunohistochemical characteristics of SMM.
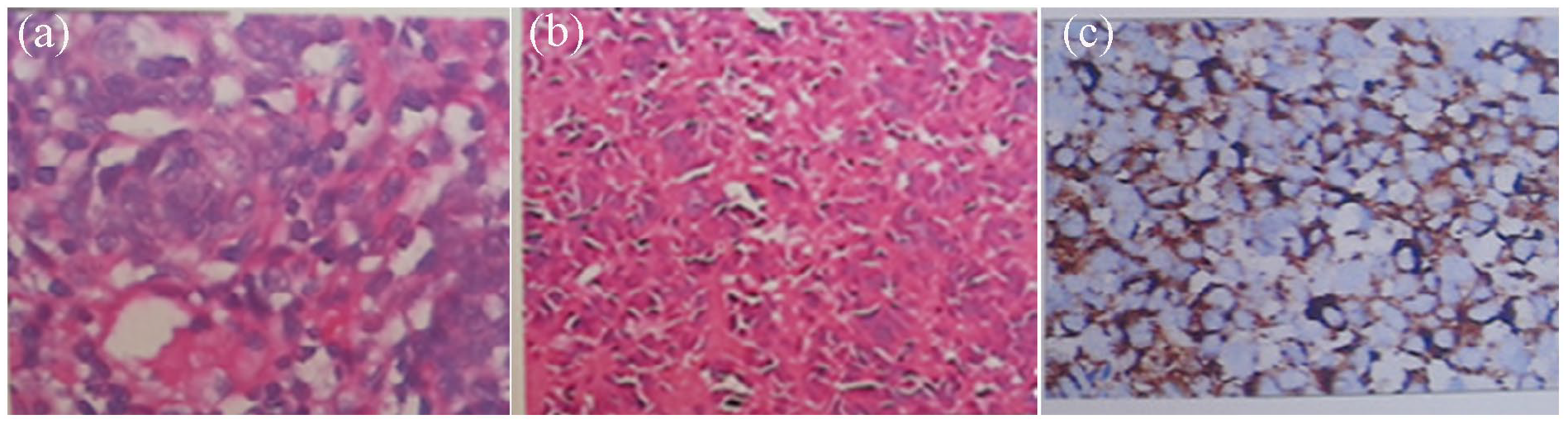
Sinonasal malignant melanoma immunohistochemical characteristics. (a) The tumor cells were oval, with large hyperchromatic nuclei and red nuclei containing pigment, using the decenucleation pigment method (+). (b) The tumor cells contained pigment, and vimentin, S-100, and HMB4 were positive in all cases. (c) S-100 (++), HMB45 (+), Ki-67 (+) 40%, HE ×100.
Results of Surgery Treatment
Treatment in the traditional surgery group (Table 1) versus the endoscope-assisted traditional surgery group (Table 2) was as follows:
Twenty-Six Patients in the Sinonasal Malignant Melanoma Group Underwent Traditional Surgery.
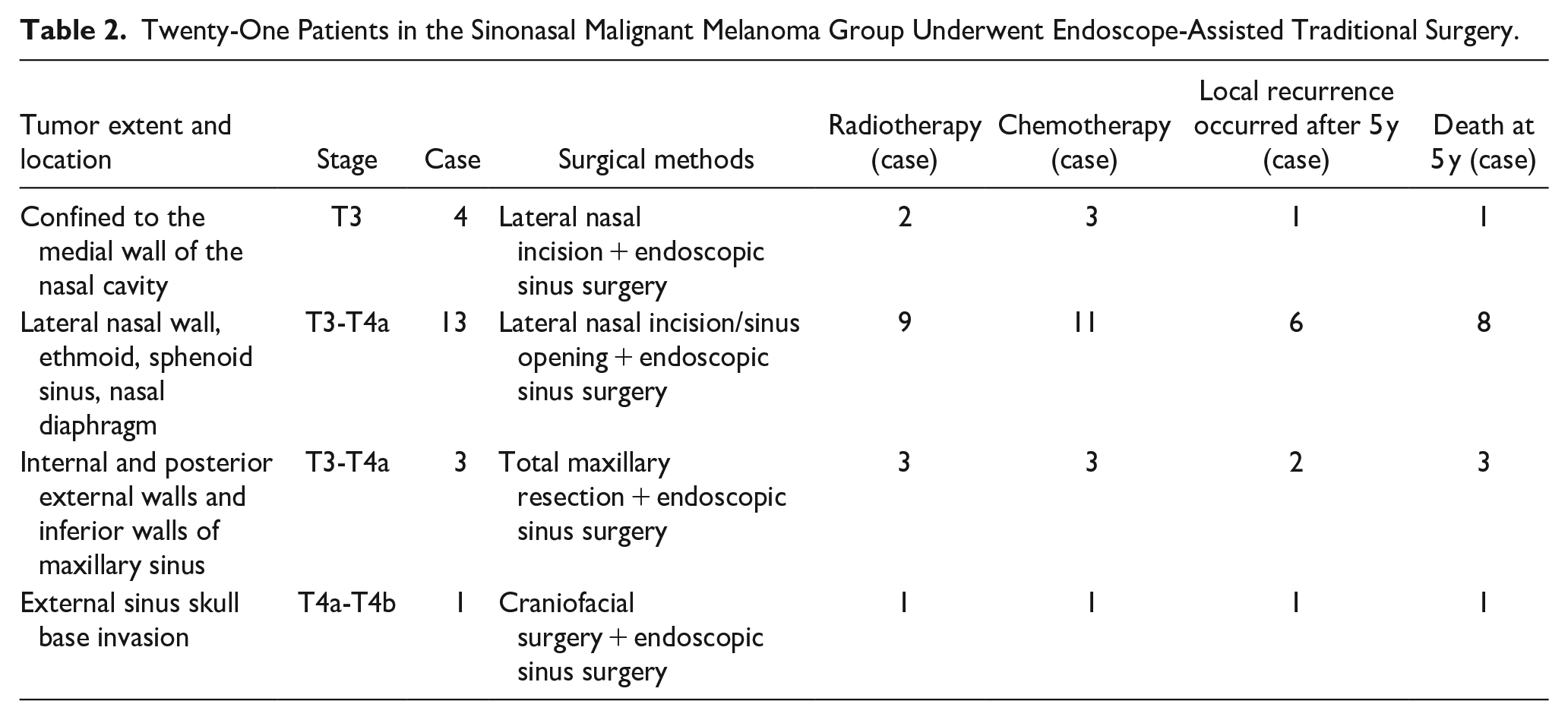
Twenty-One Patients in the Sinonasal Malignant Melanoma Group Underwent Endoscope-Assisted Traditional Surgery.
Statistical Results
In the traditional surgery group, the 3 year local recurrence rate was 57.6% (15 out of 26 patients), with 15 patients dying within 3 years, resulting in a survival rate of 42.3% (11 out of 26 patients). The 5 year local recurrence rate was 73.1% (19 out of 26 patients), with 6 patients who experienced local recurrence undergoing local resection. Twenty-one patients died within 5 years: 5 patients had intracranial spread and metastasis, 4 had lung metastasis, 7 died after discontinuing treatment due to local recurrence and spread, 3 died from other distant metastasis and other diseases, and 2 were lost to follow-up. The survival rate was 19.2% (5 out of 26 patients).
In the endoscope-assisted traditional surgery group, the 3 year local recurrence rate was 23.8% (5 out of 21 patients), with 9 patients dying within 3 years (3 patients died of intracranial recurrence and metastasis within 12 months, while 6 patients died of local recurrence and systemic multiple metastases), resulting in a survival rate of 57.1% (12 out of 21 patients). The local recurrence rate was 47.6% (10 out of 21 patients) at the 5 year follow-up. Four out of 7 patients with local recurrence were followed up after a simple endoscopic local resection. Four patients died after 2 years, resulting in a survival rate of 38.1% (8 out of 21 patients).
The 3 year local recurrence rate was 57.6% in the traditional surgery group and 23.8% in the endoscope-assisted traditional surgery group, χ2 = 5.4558, P = .020 (P < .05), and the difference was statistically significant, the endoscope-assisted traditional surgery group had a lower 3 year local recurrence rate. The 3 year survival rate was 42.3% in the traditional surgery group and 57.1% in the endoscope-assisted traditional surgery group, χ2 = 1.0231, P = .312 (P > .05), and the difference in 3 year survival was not significant between the 2 groups.
The 5 year local recurrence rate was 73.1% in the traditional surgery group and 47.6% in the endoscope-assisted traditional surgery group, χ2 = 4.4052, P = .036 (P < .05), and the difference was statistically significant, the endoscope-assisted traditional surgery group had a lower 5 year local recurrence rate. The 5 year survival rate was 19.2% in the traditional surgery group and 38/1% in the endoscope-assisted traditional surgery group, χ2 = 4.3085, P = .038 (P < .05), and the difference was statistically significant, the endoscope-assisted traditional surgery group had a higher 5 year survival rate.
Therefore, there were significant differences in the local recurrence rates at 3 and 5 years, as well as the 5 year survival rate, between endoscope-assisted traditional surgery and traditional surgery in the treatment of SMM. This indicates that the 2 different surgical methods had a significant impact on the local recurrence and survival rates of SMM.
The Postoperative Follow-Up Was Reviewed
After the operation, the surgical sites of all patients healed successfully, and there were no occurrences of cerebrospinal fluid leakage. There were 12 patients with mild diplopia without intracranial infection, and 8 patients with epiphora. Postoperative follow-up included endoscopic and/or CT/magnetic resonance imaging (MRI) examinations to detect local recurrence at the surgical site, chest X-rays, abdominal ultrasounds, and head and/or CT/MRI examinations to detect distant metastasis. The tissue from the suspected local recurrence was removed and sent for pathological examination. The follow-up findings and treatment are shown in Figure 4.
Local recurrence was detected during the follow-up and was treated with endoscopic resection. (a) MRI recurrence was observed 2 years after the surgery. (b) Internal mirroring recurred 2 years after the surgery. (c) The recurrent lesions were resected using an endoscope. (d) After resection of the recurrent lesion. MRI, magnetic resonance imaging.
The patients were followed up for 3 and 5 years, and local recurrence was primarily found in concealed areas of the nose, the outer wall of the maxillary sinus, the pterygopalatine fossa, the infratemporal fossa, and the nasopharynx. Because the recurrence was sporadic, the number of cases was small, and the local recurrence was not statistically significant. However, it is of guiding significance for us to remove the residual tumor in the hidden parts above as much as possible during the operation and at the postoperative follow-up sites.
Discussion
Incidence of SMM
SMM originates in the dendritic melanocytes of the respiratory mucosa epithelium and stroma of the nasal cavity and paranasal sinuses. The appearance is dark, gray-brown, black rough masses, and there are a few similar polypoid amelanotic melanomas. SMM mainly occurs in middle-aged patients over 45 years old, with a high degree of malignancy. It is rare in clinical practice, accounting for less than 1% of all melanomas and less than 5% of nasal and paranasal sinus tumors. 11 The onset of the disease is insidious, and the symptoms are atypical, such as nasal obstruction or epistaxis, which can easily result in clinical misdiagnosis. 12 The lesions mainly affected the mucosa and submucosa of the nasal cavity and paranasal sinuses. Bone invasion and destruction may occur during the development of the lesions. In the late stage, the lesions may invade the external nose, orbit, skull base, cervical lymph nodes, and distant metastases. 10 CT and MRI do not have specific manifestations, but they can effectively show the location of the lesion, surrounding bone destruction, and invasion of adjacent important structures. This information is crucial for the surgeon to understand the extent of the surgery and safeguard important organs. 13
Treatment Options for SMM
Surgical treatment
According to the location and scope of the tumor, different surgical methods should be adopted to remove the lesion and attempt to preserve and restore local function.
Lateral rhinotomy, partial maxillectomy, total maxillectomy, extended maxillectomy, combined craniofacial approach resection, and midface flip surgery are traditional surgical methods for the removal of nasal malignant tumors.14-16 These procedures allow for relatively complete and large resection of the tumor while avoiding extrusion and tearing of the tumor. Postoperative facial scars can affect appearance and lead to increased intraoperative bleeding. In addition, deep and hidden areas may be difficult to access. 17
Under the nasal endoscope, the vision is clear, and the tumor growth site can be carefully explored. The nasal meatus, the sieve roof, the olfactory cleft, the pterygopalatine fossa, the frontal recess, the orbital lamina, the orbital fascia, the skull base, the meninges, and other hidden deep parts can be accurately polished. Suspicious parts can also be precisely resected and repaired simultaneously.18,19 However, endoscopic surgery alone is not effective for hemostasis and cannot completely remove the tumor. At present, we only use it for relatively localized lesions. 20
In this study, 47 patients were mainly treated with surgery, followed by postoperative adjuvant radiotherapy, chemotherapy, immunotherapy, and other comprehensive treatment. 21 We first performed traditional surgery to remove the large mass, and then carefully explored the hidden deep part using a nasal endoscope. If there was residual mass, we could use plasma and electrokinetic instruments under an endoscope to track and remove it. If necessary, a portion of the suspicious orbital lamina, orbital fascia, skull base, and dura mater could be excised and repaired simultaneously. Among them, 2 cases were treated with partial resection of the dura, 3 cases with reconstruction of the skull base (using muscle or fascia), 4 cases with partial resection of the orbital fascia and orbital fat, 4 cases with positive results on frozen section, and 16 cases with plasma or electric drill to remove or sand the hidden part to observe whether there were satellite lesions or skip growth lesions that must be removed. Traditional surgery is difficult to observe and deal with the above areas, combined with endoscopy can better deal with lesions.
The retrospective study by Lombardi et al found no increased risk of death with endoscopic resection as compared with more extensive surgical approaches. 22 Miglani et al found that endoscopic surgery performed by an experienced team in patients with SMM resulted in comparable survival and better local control compared with open surgery. 23 International Consensus Statement on Allergy and Rhinology: Sinonasal Tumors proposes that for tumors that may not be completely removed through endoscopic methods, open surgical approaches remain crucial. The choice should be based on patient factors and surgical team experience, but in many cases, endoscopic methods are associated with shorter recovery times and lower complication rates. 24 Therefore, we recommend utilizing traditional surgical techniques in conjunction with nasal endoscopic technology to completely remove the tumor while preserving the function of the surrounding tissues and organs as much as possible, offering complementary advantages.
Comprehensive treatment
Surgery is an important method for treating SMM. At the same time, the biological characteristics of SMM must be taken into account, and specific comprehensive treatment should be adopted. Melanoma is not sensitive to radiotherapy. Some studies have shown that radiotherapy can enhance the local control rate and decrease the recurrence rate, but it has not significantly improved the 5 year survival rate.25,26 Chemotherapy is mainly used as adjuvant therapy such as azacytidine, nitrosourea, and cisplatin, and biological immune agents such as interferon and interleukin can be used at the same time. Chemotherapy alone has no significant benefit for SMM patients and is not recommended as a single treatment. 27 In recent years, gene-targeted therapy, immunotherapy, and neoadjuvant therapy have also made promising progress.28-30 At present, comprehensive treatment methods such as chemotherapy, radiotherapy, and biological immunity, based on extensive and complete resection of the tumor, are preferred. 31
Conclusion
With the continuous improvement of endoscopic technology, the development of various instruments, and repair methods, we are more confident and secure in the complete removal of tumors. However, the low incidence of SMM and the relatively small sample size, the prognosis is influenced by the site of occurrence, depth of invasion, stage of the lesion, presence of distant metastasis, biological characteristics, and other factors. Although there are significant differences in the 3 and 5 year local recurrence rates and 5 year survival rates between endoscope-assisted traditional surgery and traditional surgery in this study, indicating that endoscope-assisted traditional surgery can more effectively remove local lesions and reduce local recurrence rates, the 5 year survival rate of the 2 groups remains low, and the overall efficacy is still unsatisfactory. In future research, we need to increase the sample size, conduct in-depth research from multiple factors and centers, and continually summarize the experiences and lessons learned. This will help us explore more effective treatment options for SMM.
Footnotes
Acknowledgements
None.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study was conducted at the Department of Otorhinolaryngology—Head and Neck Surgery at the Third People’s Hospital of Yunnan Province. In studies involving human participants, all procedures complied with the ethical standards of the institutional and/or national research committees, the 1964 Declaration of Helsinki, its later amendments, or similar ethical standards. The study was approved by the review board of the Third People’s Hospital of Yunnan Province (202001BA070001-079).