
Abstract
Cystic lymphangioma is a rare benign congenital malformation of the lymphatic system. It usually presents in childhood and rarely in young adults. Its management lacks consensus, and its prognosis varies depending on the location. We report a case of cervical cystic lymphangioma in a young adult with chronic left lateral cervical swelling. Examination revealed a high jugulocarotid swelling, non-pulsatile, and transilluminable. Radiographic exploration suggested a cystic lymphangioma. Histopathology confirmed the diagnosis. The patient underwent a sclerotherapy session, followed by surgical excision. Our case illustrates a rare presentation of cervical cystic lymphangioma in a young adult and aims to increase awareness of this rare entity and provide literature insights into its diagnosis and treatment in adult patients.
Introduction
Cystic lymphangioma is a benign congenital malformation that affects mainly the pediatric population and is rare in adults. 1 It is an ubiquitous malformation, but the preferred site is the cervicofacial level. The diagnosis of cystic lymphangioma remains histological, treatment is not consensual, and it is significantly affected by its classification and location. This can range from cases where the condition spontaneously regresses without any treatment to cases where, even with comprehensive treatment, severe complications and sequelae occur.1-3 We report a case of cervical cystic lymphoma in a middle-aged female.
Case
This concerns a 20-year-old patient with no notable medical or surgical history, who presented to our service for a progressively evolving left lateral cervical swelling over the past 3 years, without associated signs of ENT, no general condition alteration, nor episodes of superinfection or trauma. Examination revealed a high jugulocarotid swelling measuring 5 cm on its longest axis with a soft, non-pulsatile, painless, and transilluminable consistency. No others lymph nodes sites were palpable and the rest of the ENT examination was unremarkable.
An ultrasound revealed a poorly defined left lateral cervical mass with anechoic content infiltrating between adjacent structures. A cervical computed tomography scan demonstrated a left retromaxillary cystic mass without a well-defined cystic wall, unseptated, measuring 40 × 26 mm axially and 57 mm in height, suggestive of a cystic lymphangioma. Additional magnetic resonance imaging showed a left lateral cervical mass with cystic signal characteristics and smooth wall margins, conforming to adjacent structures without invasion, extending from the skull base to C7 with extensions into the pre-styloid parapharyngeal space and infratemporal fossa (Figure 1).
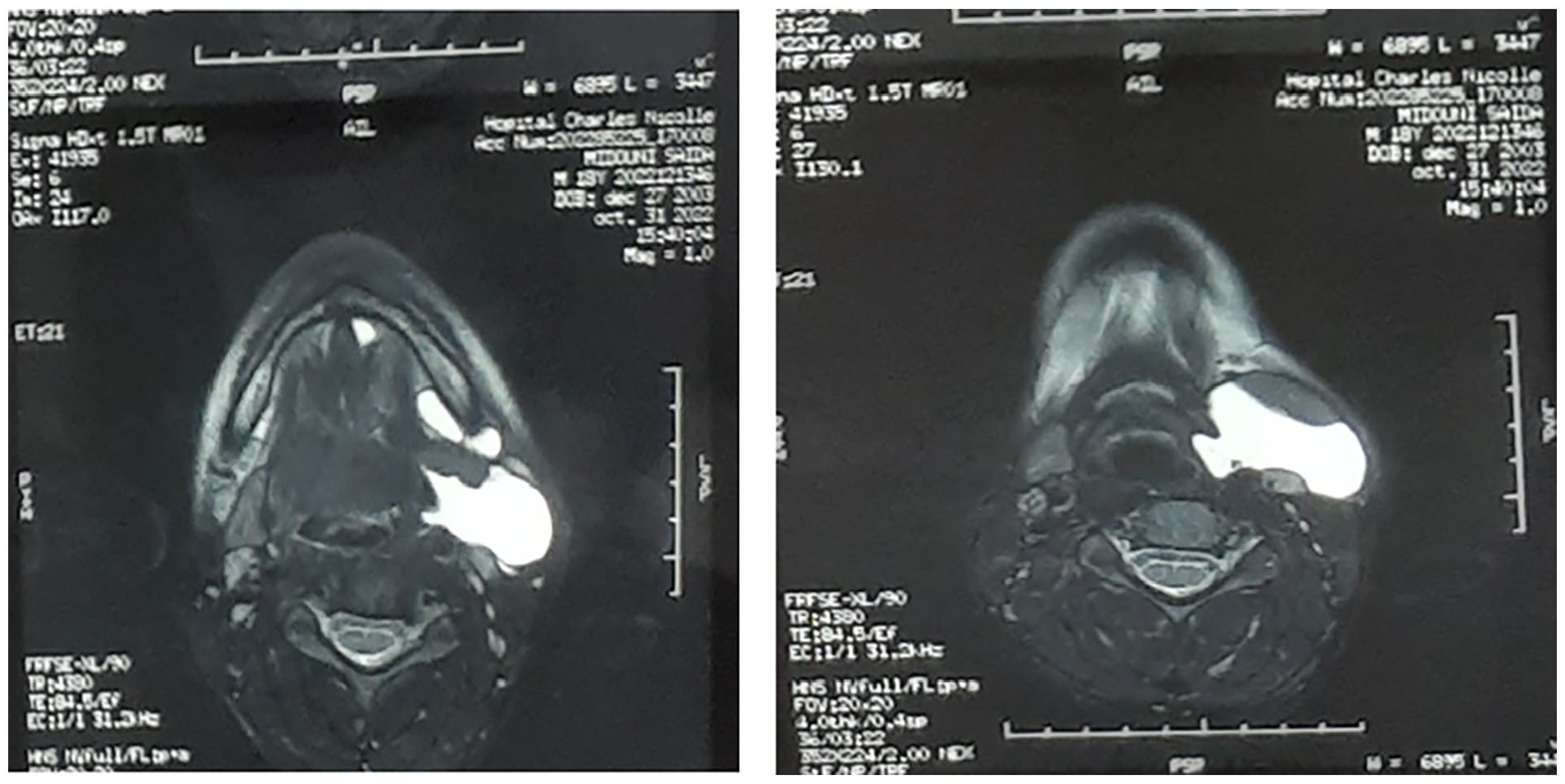
Axial sections of a magnetic resonance imaging showing a left lateral cervical mass with cystic signal without invading the adjacent structures.
The patient underwent a single session of sclerotherapy with a 50% partial regression of the mass. However, she declined further sclerotherapy attempts, leading to the decision to perform surgical excision with informed consent. Intraoperatively, the mass extended to the oral floor with extensions to the parotid and laryngeal regions. Complete excision was achieved (Figure 2) and the postoperative course was uneventful. The final histopathological examination confirmed the diagnosis.
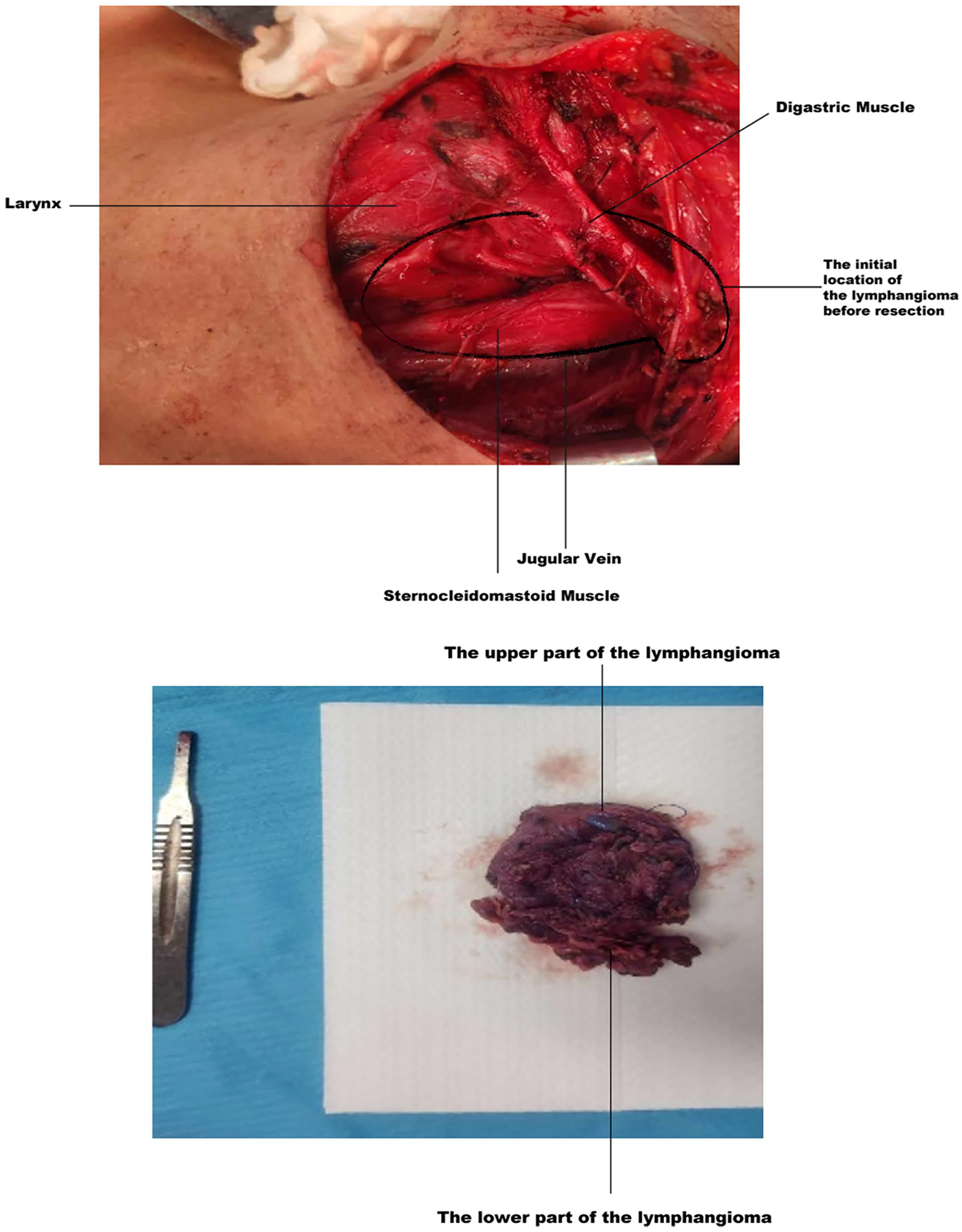
Location of lymphangioma after resection.
Discussion
Cystic lymphangioma is a rare benign congenital dysplasia of the lymphatic vessels, affecting 1 in 6000 to 1 in 4000 births, with 80% to 90% of cases diagnosed before the age of 2 years.1,2 Its discovery in adulthood is rare; however, it can occur at any age due to the progressive nature of its evolution. 3 In our case, the lymphangioma appeared in young adulthood (20 years). Cystic lymphangioma is most often unilateral, with no reported sex or side predominance in the literature, both for children and adults.1,2 It is a ubiquitous malformation. The preferred site is at the cervicofacial level (75%). 4 Other locations have been described in the literature, including abdominal location (10%) (retroperitoneal), 5 colic, splenic, 6 thoracic, especially axillary (20%) 7 and exceptionally pelvic (spermatic cord) 8 or in the limbs. 9 To date, the literature has reported fewer than 150 cases of cervical cystic lymphangioma in adults. Our case presented cervical cystic lymphangioma without thoracic extension or multiple abdominopelvic localization, as described in the Tunisian series by Ghammem et al. 10
The etiopathogenesis of cystic lymphangioma is elucidated by 2 main theories that explain the various clinical and radiological aspects of this malformation. The theory of mechanical obstruction to the drainage of lymphatic sacs into veins after trauma, infection, or neoplasia explains the formation of cystic hygroma. The second theory, known as congenital theory, is currently the most accepted, suggesting that these lymphatic lesions are the result of the sequestration of lymphatic tissues at an early stage of embryogenesis. 8
For our patient, congenital theory appears to be implicated due to slow evolution and the absence of a history of trauma or previous infectious episodes. Cystic lymphangiomas are characterized by a wide range of clinical presentations, ranging from simple aesthetic discomfort or eating difficulties to life-threatening symptoms (acute respiratory distress) for lingual, oropharyngeal, hypopharyngeal, and laryngeal locations. These locations are rare in adults, where asymptomatic forms are predominant. Wang et al. reported 71.43% of asymptomatic cases. 13
The International Society for the Study of Vascular Anomalies has established a classification of lymphatic malformations based on different clinical aspects. 11 It categorizes classic cystic lymphangioma into 3 distinct types: macrocystic or cystic hygroma (1 cm in diameter), preferably located in the posterior cervical triangle and being the most common form; microcystic or cavernous (diameter <1 cm), preferably located in the tongue, salivary glands, and buccal floor; and finally, the capillary form representing the rarest form. 12
Imaging plays a crucial role in the treatment of cystic lymphangioma. Ultrasound helps suggest the diagnosis and guide potential sclerotherapy. Magnetic resonance imaging serves as the gold standard, allowing the evaluation of invasion in adjacent structures and guiding potential therapeutic interventions, showing a mass with hypointensity T1 and hyperintensity T2 that does not improve with gadolinium injection, characteristic of lymphangioma. 13
Furthermore, the diagnosis of cystic lymphangioma remains histological. Histologically, the classic cystic lymphangioma is rich in cystic content rich in lymphocytes, macrophages, and proteins, distinguishing it from other lymphatic malformations, notably generalized lymphatic anomaly and kaposiform lymphangiomatosis. 14
Various therapeutic approaches are available to treat this malformation. However, management is not consensual, making it challenging to identify predictive clinical or radiological criteria for the success of each treatment. 15 Thus, in 2015, Balakrishnan et al. suggested establishing a series of objective criteria to evaluate the impact of a lymphangioma, organize the therapeutic approach, and facilitate monitoring of the lymphangioma’s evolution over time or in response to treatment. Sclerotherapy is preferred as the initial treatment for macrocystic forms. Although surgery is reserved as first-line treatment in case of contraindication to sclerotherapy, it is inefficacy for multiseptated forms or when histological confirmation is required. Given its infiltrating nature that does not adhere to classical dissection planes, lymphangioma excision is not complete in the majority of cases.16,17
Laser and radiofrequency represent the treatment of choice for microcystic forms. 18
In terms of systemic treatment, sirolimus is the first-line molecule for extensive forms not accessible by other therapeutic means.
A significant recurrence rate is observed after treatment, with approximately 22% to 27% after surgery and about 57% after sclerotherapy. 17 No therapeutic method consistently achieves satisfactory results and the therapeutic response varies for the same treatment. This variability may be due to the diversity of the molecular biological background of cystic lymphangioma. 1
Some recent studies have shown that abnormal expression of the VEGF-C molecule in lymphatic endothelial cells may contribute to the pathogenesis of lymphangioma, and neuropilin-2 (Nrp2) is essential in VEGF-C-induced lymphangiogenesis. In recurrent lymphangiomas, VEGF-C and Nrp2 are positively regulated, suggesting that targeting VEGF-C/Nrp2 could be an effective therapeutic approach. Other signaling pathways are also being studied and these molecular biological mechanisms are not well understood. Therefore, it is essential to deepen our understanding of the pathogenesis of lymphangioma to design more effective diagnostic and treatment strategies. 1
Conclusion
In summary, our case report underscores the rarity of cervical cystic lymphangioma in young adults and emphasizes the importance of accurate diagnosis and complete surgical excision for optimal management. More research is needed to refine the treatment approaches and outcomes in this demographic.
Footnotes
Data Availability
Data used during this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study is exempted from ethical approval at our institution.
Consent
Written informed consent was obtained from the patient for the publication of their clinical details and images.