
Abstract
Keywords
Introduction
The chorda tympani nerve (CTN) innervates the taste sensation region in the anterior two-thirds of the tongue and sublingual and submandibular salivary glands. Among CTN injuries caused by surgical procedures, the most common occurs during middle ear surgery. 1 This injury causes taste disturbance, including taste alteration and/or dryness of the mouth, numbness, and/or burning of the tongue, as well as other related symptoms.2,3 The incidence of CTN injury after endoscopic tympanoplasty is lower than that after microscopic surgery. 4 However, the incidence of taste disturbance varies depending on the surgical approach, surgical technique, and time of assessment. Moreover, the incidence of taste disturbance after middle ear surgery is often underestimated. 5 The full-thickness tragus cartilage graft and elevated tympanomeatal flap techniques have always been adopted in type I endoscopic myringoplasty. However, the incidence of early postoperative taste disturbance (EPTD) was high in our study. We analyzed the possible reasons for this and modified the surgical technique. Modified surgery patients were included in the test group, and those previously receiving conventional surgery were included in the control group. In this study, grouping and other factors that may affect EPTD were included in univariate and multivariate analyses. We aimed to explore the effect of modified surgery on EPTD and guide future surgery.
Materials and Methods
This was nonrandomized controlled study with a prospective test group and a retrospective control group. Adult patients (≥18 years old) with chronic otitis media, perforation of the drum, active ossicular chain during intraoperative exploration, and no preoperative taste disturbance, were included. Control group: The full-thickness tragus cartilage graft was placed close to the bony annulus to ensure drum integrity (Figure 1(a)) (Supplemental material video 1). Sixty-two patients were included in this group from August 29, 2020 to April 22, 2021. Modified surgery group (test group): The cartilage graft was not in contact with the posterior-superior bony annulus and the inferior-posterior of the scutum (Supplemental material video 2). The surgeon ensured that the cartilage did not compress the point where the CTN entered the tympanic cavity and minimized direct contact between the graft and CTN. The integrity of the drum was ensured by the perichondrium (Figure 1(b)). Sixty-two patients were included in the modified surgery group from April 26, 2021 to November 30, 2021.
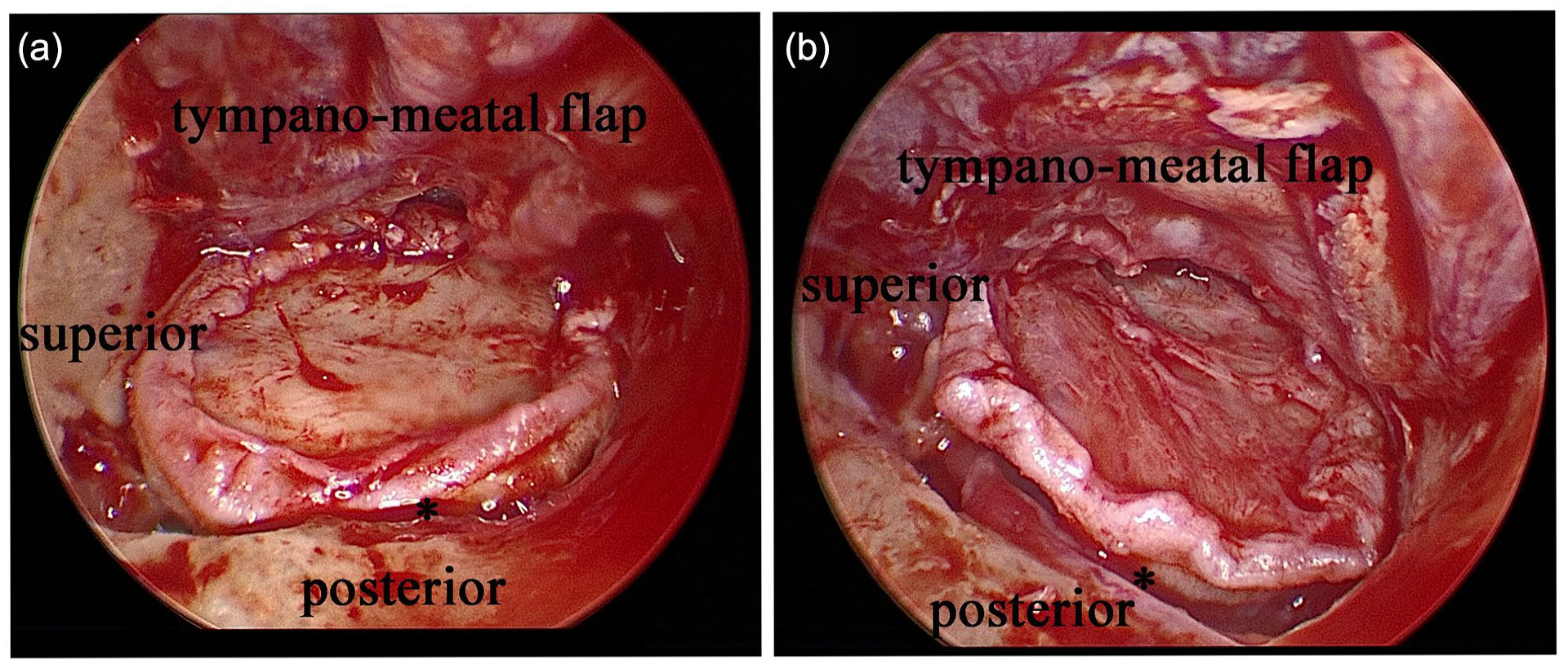
(a) The full-thickness tragus cartilage graft is placed as close to the bony tympanic annulus as possible to ensure drum integrity in the control group. Asterisk shows distance between graft and bony annulus. (b) Cartilage graft is not placed in contact with posterior-superior bony annulus and inferior-posterior of the scutum in the modified group. Asterisk shows distance between graft and bony annulus.
This study was registered in the Chinese Clinical Trial Registry (ChiCTR 2100042247). The study protocol was approved by the Ethics Committee of the hospital (approval number: 2020134).
Surgical Procedure
Under the 0° endoscope, the tympanomeatal flap was elevated transcanally from 11 o’clock to 6 o’clock in the external auditory canal (left ear). The posterior malleolar ligament was protected when no lesions were found around the CTN. After the middle ear cavity had been entered, lesions were cleared, ossicular chain activity was checked, patency of the eustachian tube was assessed, and the cavity was flushed with saline. The cartilage graft was measured and trimmed (see Measurement of cartilage graft size). The graft was placed in an appropriate position, the tympanic cavity was packed with gelfoam, the tympani-meatal flap was restored, and the external auditory canal was packed with gelfoam.
Variables Definition
Dependent variables: EPTD, early postoperative taste disturbance. Taste disturbance included taste alterations, dryness of the mouth, and/or tingling, numbness, and/or burning of the tongue. Taste alteration is the primary symptom. If the patient had any of the above symptoms, they were considered to have EPTD. Independent variables: (1) manipulated CTN or not: When lesions were found around the CTN, the nerve was involved due to the clearance of the lesions, but the CTN was preserved by dissection; (2) size of the cartilage graft; (3) vertical and anteroposterior diameters of the bony annulus [computed tomography (CT) measurements]; (4) a postoperative air-bone gap (ABG) with pure-tone average ≤20 dB was considered a good hearing result; (5) the positions where the CTN enters the tympanic cavity are classified as “posterior-superior area” (9-12 o’clock in the right ear, 12-3 o’clock in the left ear), and “posterior-inferior area” (6-9 o’clock in the right ear, 3-6 o’clock in the left ear); (6) in the posterior-superior area, part of the CTNs runs below the bony annulus (exposed), while the other part runs inside the annulus(unexposed). The degree of taste recovery was classified as follows: (1) not recovered at all, (2) partial recovery, and (3) no taste disturbance.
Taste Test and Questionnaire for Taste
The patients underwent the taste tests and taste questionnaires before surgery and on the first day after surgery. Taste test method: A pipette was used to drop the taste test reagents 1-1.5 cm from the tip of the tongue on both sides of the midline. First, the surgical side (the order of the 4 flavors was random), and then the nonsurgical side (the order of the taste reagents was randomized again). Concentration and preparation methods of taste test solution: (1) Acid: 7.5 g citric acid per 50 ml; (2) Sweet: 17.115 g sucrose per 50 ml; (3) Bitter: 0.0764 g quinine sulfate per 50 ml; (4) Salty: 2.922 g sodium chloride per 50 ml. The taste test reagent for the follow-up was dissolved in sterile distilled water. The taste scores of sour, sweet, bitter, and salty taste ranged from 0 to 10 points. A score of 0 points meant that the taste was utterly absent, and 10 points meant that the taste was normal.
We received taste questionnaires from 124 patients (62 in the control group and 62 in the test group), while only 91 patients completed the taste test (47 in the control group and 44 in the test group).
Measurement of Cartilage Graft Size
The full-thickness cartilage was photographed and measured using a ruler during surgery, as shown in Figure 1(c). AB is the vertical diameter of the cartilage, and CD is the anteroposterior diameter of the cartilage. The photographed pictures were imported into image J (National Institutes of Health, Maryland, USA) and the line segments AB, CD, and scale EF were measured. The calculation methods were vertical diameter: AB/EF(cm), and anteroposterior diameter: CD/EF(cm), and the results were retained to two decimal places.
CT Scan and Bony Tympanic Annulus Measurement
Each patient’s temporal bone CT scan was obtained using a 128-channel multidetector SOMATOM Definition Edge CT scanner (Siemens Inc., Munich, Germany). Scanning was performed from the lower margin of the external auditory canal to the upper margin of the petrous bone. Initial axial sections of 0.6 mm thickness were obtained. According to the transverse axial images, oblique sagittal images of the bony tympanic annulus were obtained using multiplanar reconstruction (MPR) postprocessing technology. The vertical and anteroposterior diameters were measured using the images. Images were displayed and measured on a three-dimensional viewer system for Digital Imaging and Communications in Medicine (Kodak, Carestream GCRIS2.1, New York, USA). The specific reconstruction and measurement methods were as follows:
The figure showed MPR standardized processing and measurement of the bony tympanic annulus. Reconstruction method (right ear as an example ): The sagittal position was selected as the target image (Figure 2(a)), and AB was the vertical diameter of the bony tympanic annulus. Point A was the malleus cutting point, which could be used as the identification mark of the upper end of the tympanic annulus. The perpendicular bisector (CD) of line AB was the anteroposterior diameter.
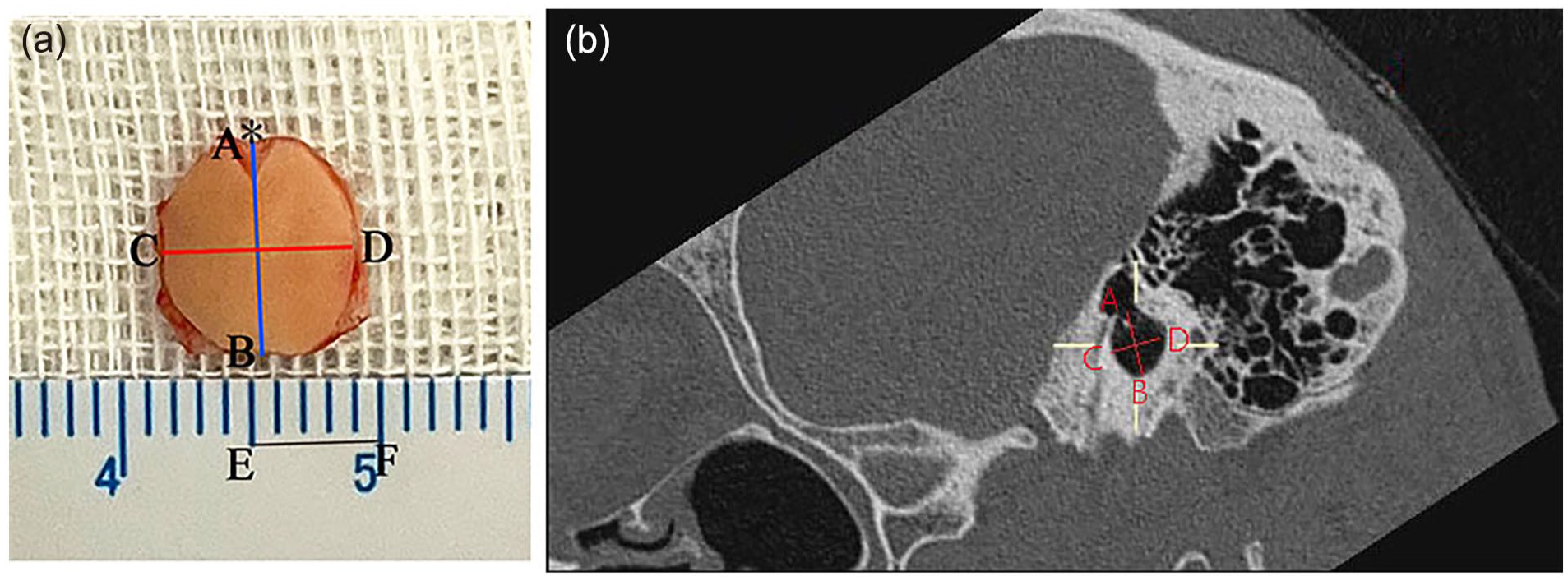
(a) Trimmed graft with perichondrium. Notch (to accommodate short process of malleus) is the upper end of the graft (as asterisk shows). (b) AB passes along the axis of the malleus handle and is the vertical diameter of the bony tympanic annulus; CD passes perpendicular to AB and is the anteroposterior diameter of the tympanic annulus. AB, vertical diameter of cartilage; CD, anteroposterior diameter of cartilage; EF, scale.
Statistical Analysis
An independent sample t-test was used to compare normally distributed variables between the 2 groups. The Wilcoxon rank-sum test and chi-squared test were used to compare ordered and categorical variables between the 2 groups, and the Wilcoxon matched-pair signed rank test was used to compare the results of the taste test. Multivariate analyses were performed using a binary logistic regression model. Statistical significance was set at P < .05. IBM SPSS for Windows (version 22.0, IBM Corp., Armonk, NY, USA) was used for all analyses.
Results
Baseline Comparisons Between the Modified Surgery and Control Groups
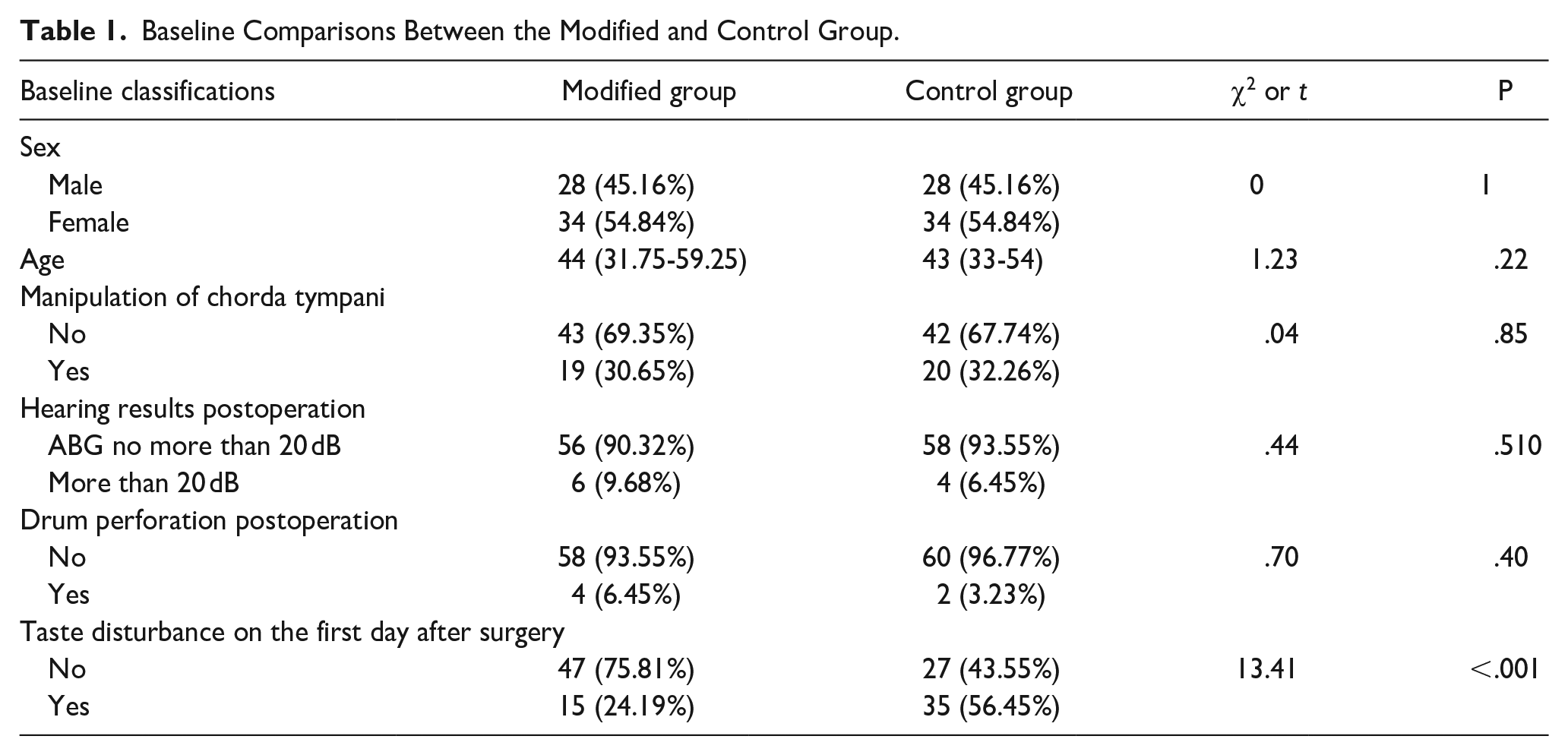
One hundred and twenty-four patients were included in the study, and 62 patients were included in each group, with an average age of 44.77 ± 13.15 years. No statistical difference was found in age or sex (t = 1.23, P = .22; χ2 = 0, P = 1) between the control and modified surgery groups. The proportions of CTN manipulation during surgery were 32.26% and 30.65% in the control and modified groups, respectively (χ2 = .04, P = .85). Good hearing results (ABG ≤ 20 dB) were achieved in both the control and test groups (93.55% vs 90.32%, χ2 = .44, P = .510). The closure rates were 96.77% and 93.55% in the control and modified groups, respectively (χ2 = .7, P = .40) (Table 1).
Baseline Comparisons Between the Modified and Control Group.
Taste Test Before and After Surgery
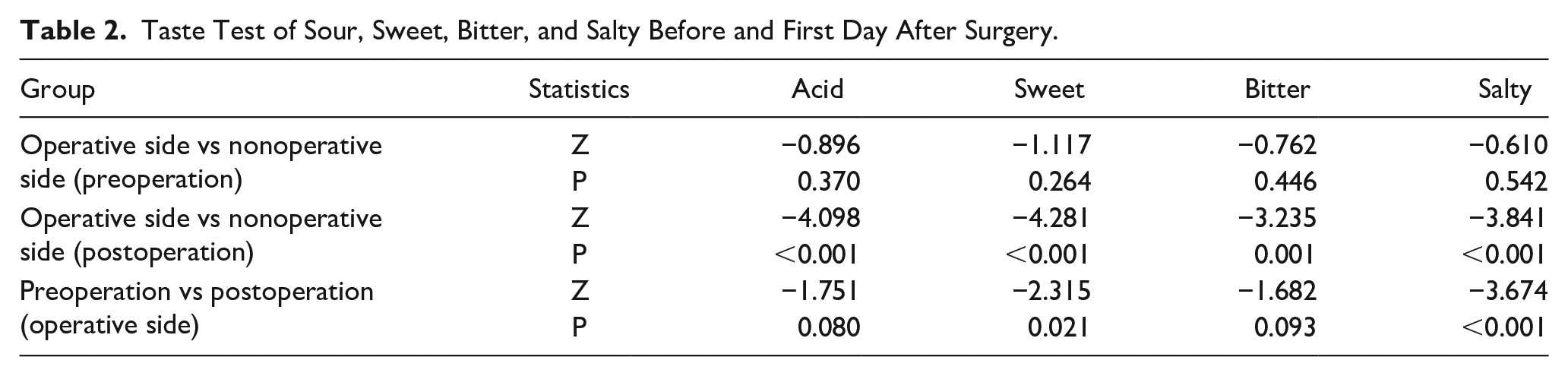
Ninety-one patients completed the 4 sections of the taste test (sour, sweet, bitter, and salty), with 47 people in the control group and 44 in the test group before and on the first day postsurgery. There were no significant differences between the operative and nonoperative sides in the 4 types of taste scores before surgery (Ps > .05). On the first day after surgery, there was a significant difference in the sour, sweet, bitter, and salty taste scores between the operative and nonoperative sides (Ps < .05). There was no difference in acid and bitterness scores on the operative side before and after surgery (Ps > .05); however, a significant statistical difference in sweet and salty scores was observed (Ps < .05) (Table 2.).
Taste Test of Sour, Sweet, Bitter, and Salty Before and First Day After Surgery.
Univariate and Multivariate Analysis of EPTD
The incidence of EPTD was significantly lower in the modified surgery group (24.19%) than in the control group (56.45%) (χ2 = 13.41, P < .001) (Figure 3). CTN manipulation during surgery resulted in a higher incidence of EPTD than in surgery without nerve manipulation (53.85% vs 34.12%, χ2 = 4.32, P = .049) (Figure 3).
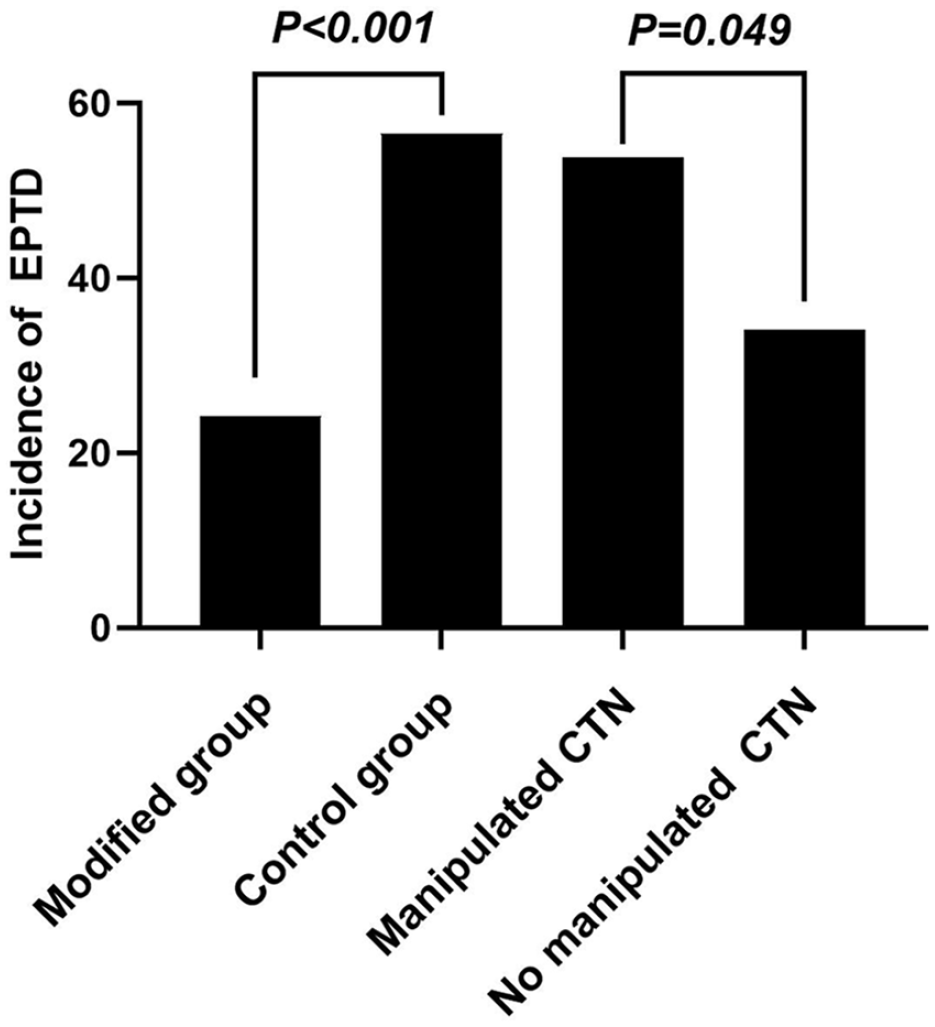
Comparisons of the incidence of EPTD between the modified and control groups and between the manipulated and nonmanipulated CTN groups. CTN, chorda tympani nerve; EPTD, early postoperative taste disturbance.
The entry point to the tympanic cavity and course in the middle ear of the CTN did not affect the incidence of EPTD (Figure 4). The positions where the CTN enters the tympanic cavity are classified as “posterior-superior area” (9-12 o’clock in the right ear, 12-3 o’clock in the left ear), and “posterior-inferior area”(6-9 o’clock in the right ear, 3-6 o’clock in the left ear). The positions’ difference does not affect the incidence of EPTD (χ2 = .187, P = .665). Besides, in the posterior-superior area, part of the CTNs runs below the bony annulus (bs), while the other part runs inside the annulus. This nerve course difference doesn’t affect the incidence of EPTD (χ2 = .542, P = .461).
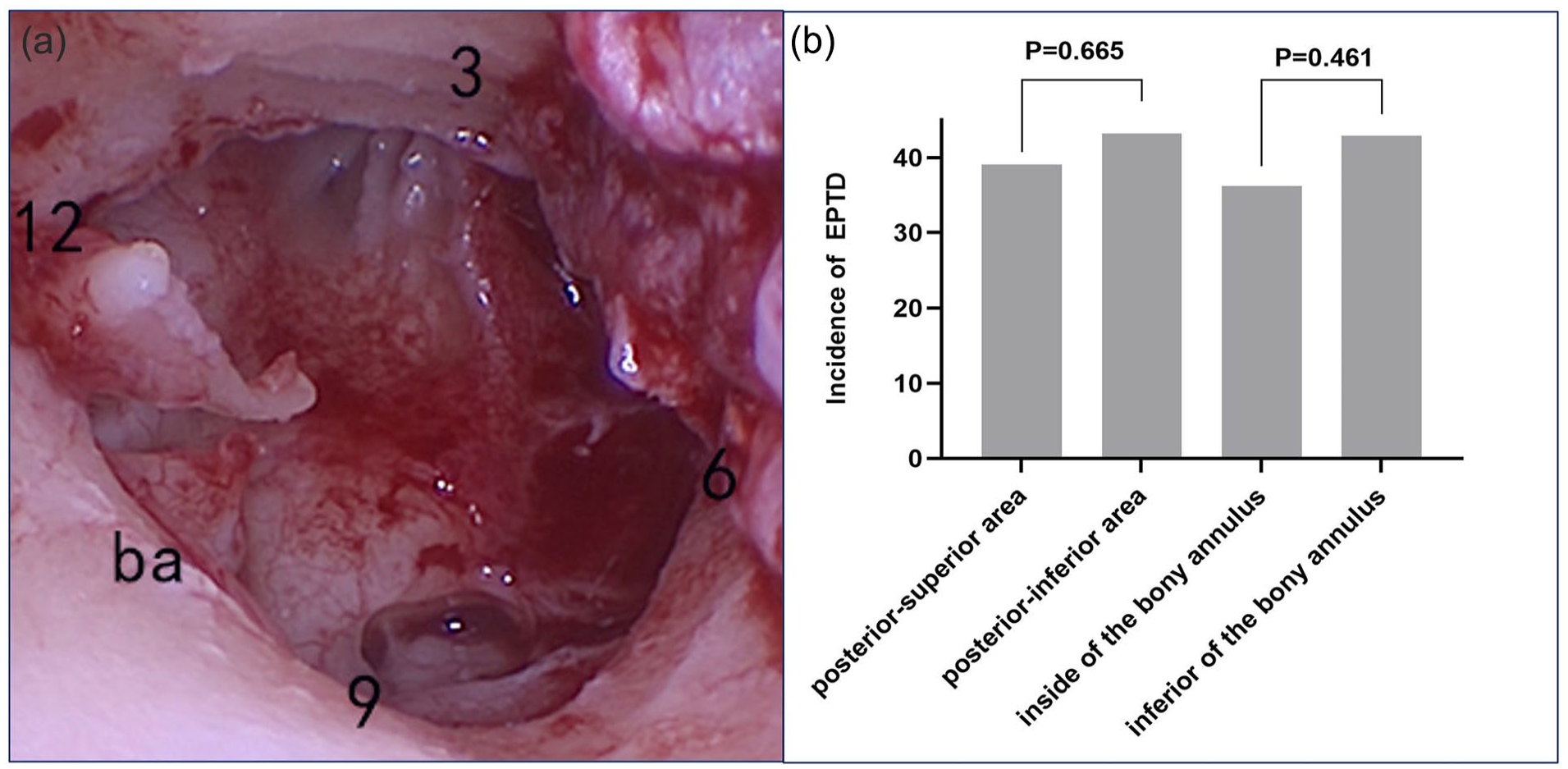
The entry point to the tympanic cavity and course in the middle ear of the chorda tympani nerve did not affect the incidence of early postoperative taste disorders (EPTD). (a). shows the right ear, the annulus above the short process of the malleus is defined as 12, and 3, 6, and 9 points are marked in a clockwise direction. The left ear is also marked in the same way. The positions where the CTN enters the tympanic cavity are classified as “posterior-superior area” (9-12 o’clock in the right ear, 12-3 o’clock in the left ear), and “posterior-inferior area” (6-9 o’clock in the right ear, 3-6 o’clock in the left ear). (b) (left) indicates that the entry point difference does not affect the incidence of EPTD. In addition, in the posterior-superior area, part of the CTNs runs below the bony annulus (ba) (exposed), while the other part runs inside the annulus(unexposed). Figure b (right) indicates that the nerve course difference does not affect the incidence of EPTD.
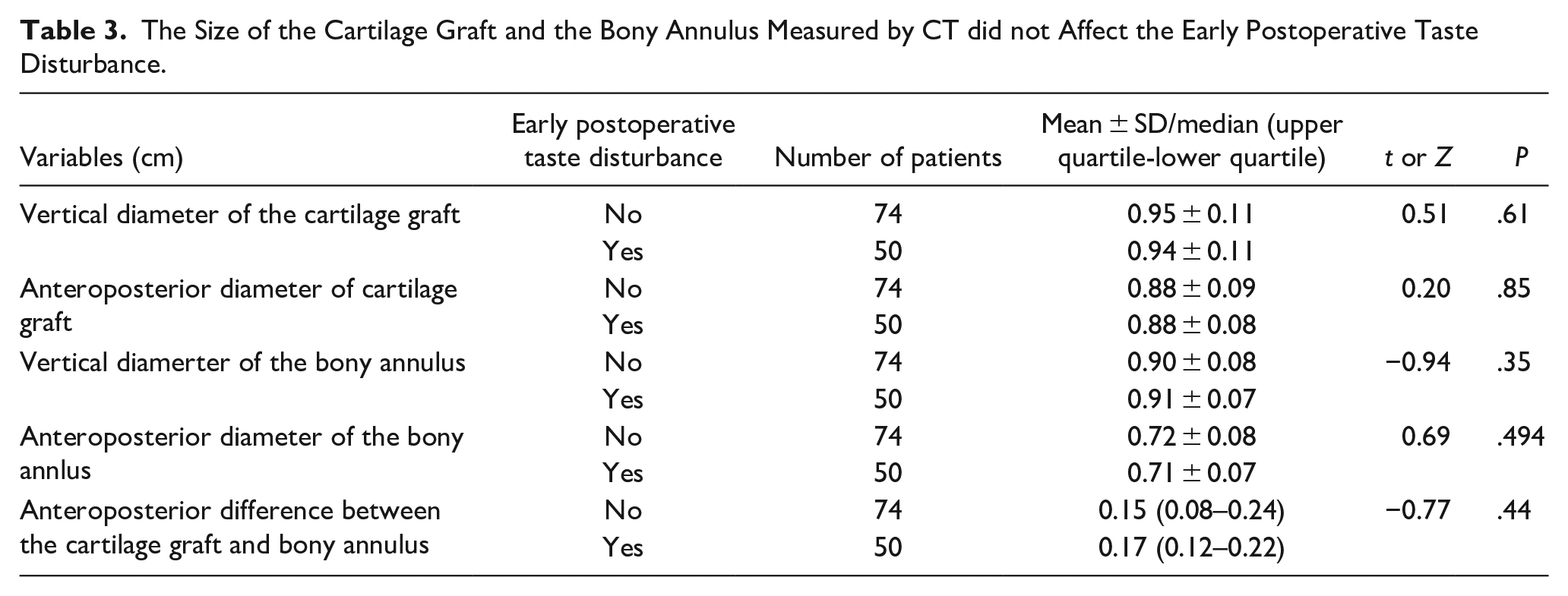
In addition, the vertical and anteroposterior diameters of the cartilage graft and bony tympanic annulus measured by temporal CT (see Methods) did not affect the incidence of taste disturbance (Ps > 0.05) (Table 3).
The Size of the Cartilage Graft and the Bony Annulus Measured by CT did not Affect the Early Postoperative Taste Disturbance.
The factors affecting EPTD were included in the multivariate analysis (Table 4). The possibility of taste disturbance in the control group was 4.24 times higher than that in the modified surgery group after surgery (P < .001); surgical CTN manipulation was also an independent risk factor, and its possibility of taste disturbance was 2.43 times higher than that without nerve involvement during surgery.
Multivariate Analysis of Factors Affecting the Early Postoperative Taste Disturbance.
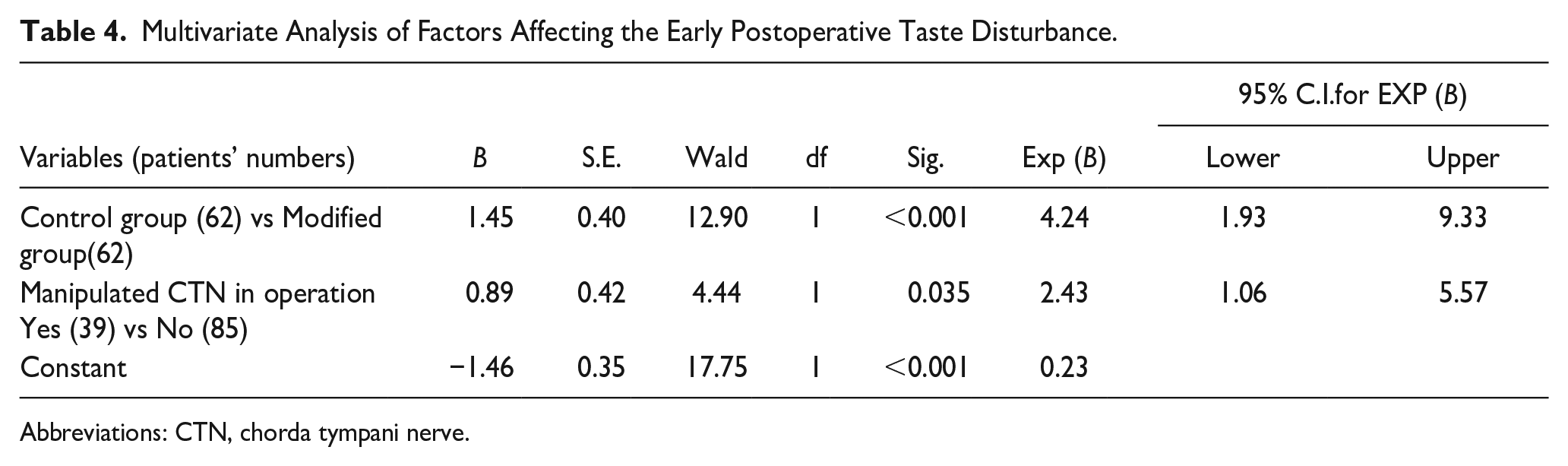
Abbreviations: CTN, chorda tympani nerve.
Prognosis of Taste Disturbance
Taste recovery was followed up at 1 and 3 months postsurgery. At 1 month follow-up, the proportions of unrecovered, partially recovered, and no taste disturbance in the modified surgery group were 9.68%, 12.90%, and 77.42%, respectively; in the control group, the proportions were 27.42%, 19.35%, and 53.23%, respectively, which were significantly better in the modified group than in the control group (Z = −2.95, P = .003). At 3 months postsurgery, the proportions of unrecovered, partially recovered, and no taste disturbance in the modified surgery group were 4.84%, 11.29%, and 83.87%, respectively; in the control group, the proportions were 11.29%, 16.13%, and 72.58%, respectively. No significant statistical difference was found between the two groups (Z = −1.57, P = .12).
In addition, surgical manipulation of CTN resulted in a lagged recovery of taste disturbance compared to that without the involvement of the nerve (Z = −2.74, P = .006) even 3 months postsurgery. The proportions of unrecovered, partially recovered, and no taste disturbance were 17.95%,17.95%, and 64.10% in the manipulated CTN group and 3.53%,11.76%, and 84.71% in the nonmanipulated CTN group, respectively.
Recommended Cartilage Graft Size
In general, the incidence of early taste disturbance in the test group was significantly lower than that in the control group. Taste disturbance gradually recovered in both groups over time. The size of the cartilage graft did not affect the incidence of EPTD, but an appropriate cartilage size can ensure easier placement of the graft and integrity of the postoperative drum while preserving adequate space between the cartilage and bony annulus. In this study, the anteroposterior diameter of the cartilage graft in the modified surgery group was 0.85 ± 0.07 cm; the upper and lower diameter were 0.92 ± 0.09 cm. A 1-2 mm perichondrium was preserved around the cartilage edge.
Discussion
Main Results
The modified surgical technique effectively reduces EPTD in type I endoscopic tympanoplasty. The subjective taste disturbance recovered over time, and no significant difference was found between the control and modified groups at 3 months follow-up. However, the recovery from taste disturbance in patients with manipulated CTN lagged significantly at 3 months compared with patients without manipulated CTN. In addition, this study recommends a suitable size for the cartilage graft; the anteroposterior diameter of the cartilage graft in the modified group was 0.85 ± 0.07 cm, and the upper and lower diameters were 0.92 ± 0.09 cm. A 1-2 mm perichondrium was preserved around the cartilage edge.
Modified Technique to Reduce Injury to CTN
The incidence of EPTD was significantly lower in the modified surgery group (24.19%) than in the control group (56.45%). The multivariate model also confirmed that the appropriate space between the cartilage graft and bony annulus was an independent risk factor for EPTD. First, when the CTN is compressed by the cartilage graft, nerve stretch may occur, resulting in functional disability of the nerve. 1 A stretched CTN leads to more symptoms. 2 Animal experiments suggest that nerve stretching can destroy nerve microcirculation. 6 Second, the anatomical diversity of the CTN increases the difficulty of the operation. Exposure of the CTN increases the possibility of injury during surgery and increases the probability of compression of the CTN by the graft. After leaving the mastoid facial nerve, the CTN runs in the posterior canaliculus, while 54.5% of the posterior canaliculus has a bone or complete defect, and the exposed CTN is easily compressed by the cartilage graft. 7 The CTN enters the tympanic cavity from the posterior canaliculus through the chordal eminence. In total, 90.9% of patients had chordal eminence, but the degree of prominence varied.7,8 The intact chordal eminence prevents graft compression directly to the point of nerve entry into the middle ear cavity. Additionally, when the CTN is on the inner side of the bone of the posterior scutum, the nerve is not easily injured. Third, the longer the CTN is free in the middle ear cavity, the more vulnerable it is to injury. For example, when the CTN enters the middle ear cavity from the external auditory canal, lateral to the annulus,9,10 the cartilage graft compresses the nerve directly; when the CTN enters the middle ear cavity at the posterior-inferior point of the annulus,7,11 the CTN in the middle ear cavity is susceptible to injury. However, the CTN in front of the malleus handle runs medial to the anterior malleolar ligament9,10 and is usually not exposed in type I tympanoplasty; therefore, it is seldom injured.
Manipulated Chord Tympanic Nerve
In this study, the multivariate analysis model confirmed that intraoperative manipulation of the CTN was an independent risk factor for EPTD. In middle ear surgery, transection, stretching, ischemia, thermal injury, overdissection, and drying of the CTN during surgery are the causes of nerve injury. 1 Although 100% of the CTN was preserved during dissection in this study, the incidence of EPTD in the manipulated CTN group remained as high as 53.85%. Other studies have also confirmed that preservation of the CTN during surgery still has a high incidence of postoperative taste disturbance.3,8 Different surgical techniques and assessment time points may lead to variations in the prevalence of postoperative taste disturbances. Although the degree of CTN injury does not predict postoperative taste disturbance, the persistence of the taste disturbance symptoms may be correlated with the degree of injury. 12 In addition, chronic otitis media inflammation will not only cause ultra-structural changes 11 and functional damage 13 of the CTN but also cause fibrous thickening of its surrounding connective tissue 14 and even the formation of granulations. CTN often runs in the thickened posterior malleolar ligament, and the inflammatory tissue around the ligament affects the exploration of the ossicular chain. When these inflammatory tissues around the CTN are removed, the manipulation inevitably causes the CTN stretch. Thirty-six percent of the CTN follows alongside the long process of the incus at the inferior third, 7 and it is prone to injury when lesions around the ossicular chain are cleared.
The Taste Recovery Over Time
Taste disturbances in the control and modified surgery groups recovered gradually over time, which is consistent with previous reports.12,15 In the first and second months after surgery, the taste disturbance rate in the modified group was significantly lower than that in the control group in our study. However, no significant difference in taste disturbance rate was found between the 2 groups 3 months after surgery. Second, intraoperative manipulation of the CTN caused a lag in the recovery from postoperative taste disturbance. The manipulation of CTN leads to worse taste severity scores than those with intact and severed CTN. 3 Although subjective taste disturbance can gradually recover over time, the electrogustometry taste threshold is still significantly increased even 3 years after surgery, and subjective taste recovery precedes the electrogustometry taste threshold. 16 In addition, morphological evidence of taste recovery has been reported. The proportion of regenerated CTN and taste buds has been discussed previously.17,18
Limitations of the Study
Finally, it is essential to note the limitations of this study. Herein, CTN injury during surgery was mainly evaluated by subjective symptoms, but chemical taste disturbance and electrogustometry taste threshold were not assessed. Second, the relationship between the different anatomical classifications of the CTN and postoperative taste disturbance was not examined. Third, this study was a retrospective control group which may induced bias. This analysis will be refined in future studies.
Conclusion
The modified surgical techniques and avoidance of excessive manipulation of the CTN can significantly reduce the incidence of EPTD and accelerate the taste recovery rate.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241271635 – Supplemental material for Taste Disturbance After Endoscopic Tympanoplasty with Tragal Cartilage Graft and Improvement Strategies
Supplemental material, sj-docx-1-ear-10.1177_01455613241271635 for Taste Disturbance After Endoscopic Tympanoplasty with Tragal Cartilage Graft and Improvement Strategies by Yi-Bo Huang, Xin-Da Xu, Jihan Lyu, Yan-Mei Wang, Xiao Fu, Meng-Ye Ma, Binjun Chen, Min-Fang Sun and Dong-Dong Ren in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
The authors thank the anesthetists and nursing team for their cooperation during surgical procedures. The authors also thank the audiologists for their assistance with pre- and postoperative audiological assessments.
Clinical Trial Registration
This study was registered with the Chinese Clinical Trial Registry (ChiCTR 2100042247).
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (NSFC) (Grant Nos. 81771017 and 81970880), Shanghai Natural Science Foundation Program (22ZR1410100), and the Clinical Research Plan of SHDC (SHDC2020CR1049B-001).
Ethics Approval Statement and Patient Consent Statement
The study protocol was approved by the Ethics Committee of the Eye, Ear, Nose, and Throat Hospital, Fudan University (approval number: 2020134). The patients’ consent for the clinical trial has been assigned before the operation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.