
Abstract
Introduction
Surgery is the most common treatment for chronic suppurative otitis media (CSOM), cholesteatomas, and some forms of adhesive otitis media (AdOM); minimally invasive approaches are becoming increasingly popular, tympanoplasties with or without cholesteatoma can be performed endoscopically. During endoscopic tympanoplasty, processing strategies for the tip of the malleus handle and its surrounding tissues have attracted research attention. Nejadkazem et al examined the incidence of intratympanic membrane cholesteatoma in patients after tympanoplasty and found that insufficient obliteration of the squamous epithelium resting on the malleus handle can lead to cholesteatoma formation.1,2 Kutluhan et al observed that, despite careful de-epithelialization, epithelium may remain and thus suggested that the tip of the malleus handle be resected to prevent cholesteatoma development following tympanoplasty. 3 Although some studies have addressed this problem, there are few relevant reports. In this study, we examined whether tissue around the tip of malleus handle likely contains epithelial remnants and should thus be resected. The auditory results were analyzed postoperatively to evaluate the curative effect.
Methods
Patients
This was a prospective analysis of clinical data from 197 patients [113 females (58%) and 84 males (42%)] who underwent endoscopic tympanoplasty at the EENT Hospital of Fudan University from June 2022 to May 2023. All patients underwent preoperative video-otoscopy with image recording, pure-tone audiometry, and temporal bone high-resolution computed tomography. All intraoperative specimens of the malleus handle tip were sent for pathological examination of the presence of residual squamous epithelium (Figure 1). Secretions from the tympanum were examined for pathogen detection.
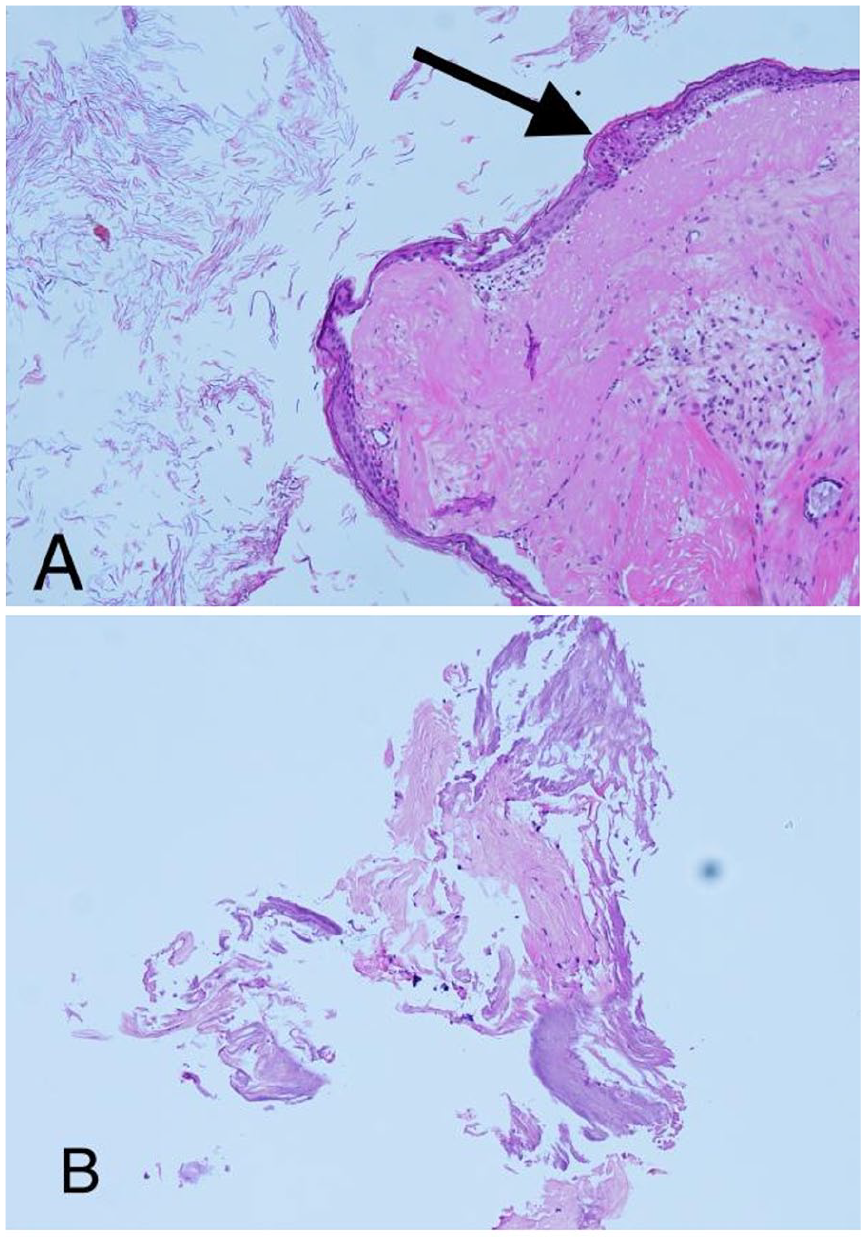
(A) Postoperative histopathology reveals the presence of squamous epithelium remnants around the tip of the malleus handle. (B) No squamous epithelium remnant remains around the tip of the malleus handle.
The Eye & ENT Hospital of Fudan University approved the study protocol (code 2020133). Written informed consent was obtained from all patients.
Inclusion Criteria
The patients were operated on by a single surgeon with 10 years of experience and who served as deputy director of otorhinolaryngology. All tympanoplasties were performed endoscopically. Preoperative pure-tone audiometry was used to confirm conductive deafness. For all patients with acquired cholesteatomas, COM, or AdOM whose conservative treatments had not been effective. All patients included in the study had complete data.
Exclusion Criteria
We excluded patients with ossicular chain destruction and the malleus could not be preserved, those with cholesteatomas with large lesions (>EAONO/JOS stage 1 4 ), and those with incomplete clinical data.
Dornhoffer Criteria 5
Type I retraction involves mild retraction of the tympanic membrane and is often noted in patients with mild Eustachian tube dysfunction or serous otitis media that is resolving. Type II retraction is characterized by tympanic membrane retraction to the incus or stapes; this is known as myringo-incudo-stapediopexy. Type III retraction is an extension of type II retraction but with involvement down to the promontory. Finally, type IV retraction is a continuation of type III retraction, but the full extent or depth cannot be adequately visualized by micro-otoscopy.
Surgical Technique
All surgeries were performed in patients under general anesthesia and consisted of a fully endoscopic transcanal approach. The ear canal was infiltrated with local anesthetic (1% lidocaine with 1:100,000 adrenaline). The edges of the perforation were refreshed by the removal of 1 to 2 mm of scar tissue. An incision was made in the skin of the external auditory canal (EAC) in the 2 to 5 anticlockwise or 10 to 7 clockwise position lateral to the annulus. The skin of the EAC was raised to the level of the fibrous annulus, by lifting the annulus out from its bony sulcus, entering the middle ear, and conserving the chorda tympani nerve (CTN). When the EAC was narrow and the fibrous annulus thus not completely exposed, we first elevated the tympanomeatal flap and then expanded the EAC by removing its bulges. We then cut the lateral ligament of the malleus, the mucosa of the Prussak space, part of the anterior annulus, and the mucosa on the side of the malleus handle down to the bony surface using a pick or a sickle knife. We then meticulously denuded the flap along the mucosal cut in the direction of the malleus handle using alligator forceps. After meticulous elevation of the tympanomeatal flap, the tissue around the tip of the malleus handle was thoroughly removed and then investigated histopathologically for the presence of remnant squamous epithelium. According to the lesion in the tympanum, if necessary, atticotomy and/or posterosuperior canal wall curettage were performed, with the secretions sent for pathogen examination. Then the tympanic lesion was removed. According to the activity of and damage to the ossicular chain, a corresponding ossicular chain reconstruction was performed. Gel foam infiltrated with dexamethasone was used to fill in the tympanum, and the tragus cartilage-perichondrium complex to repair the tympanic membrane. Then the tympanic membrane flap was repositioned, and the ear canal was filled with gel foam. The mean duration of surgery was 48.23 ± 13.62 minutes, and the mean duration of tissue removal around the tip of the malleus handle was 4 ± 1.32 minutes (Figure 2).
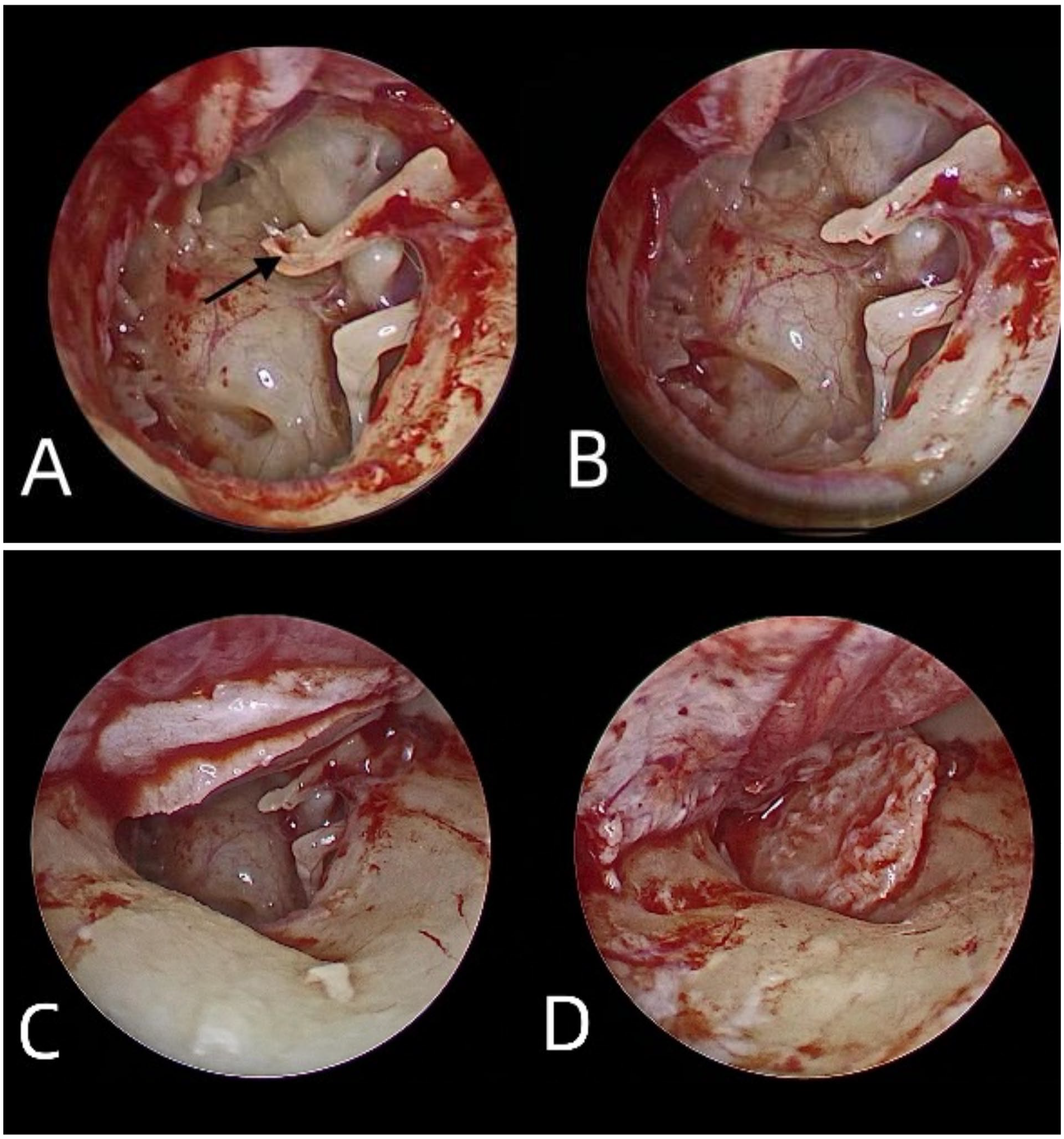
(A) After meticulous elevation of the tympanomeatal flap, remnant tissue around the tip of the malleus handle is exposed. (B) Remnant tissue around the tip of the malleus handle is completely removed, followed by (C, D) tympanic membrane repair using the tragus cartilage-perichondrium complex.
Postoperative Follow-Up
All patients were followed up 3 weeks after surgery. A postoperative pathological evaluation of the tissue around the tip of the malleus handle was performed to determine the presence of squamous epithelium. We assessed the correlations of the presence of epithelial remnants with exposure of the malleus handle and microbial infection of the middle ear. Preoperative/postoperative air conduction (AC), bone conduction (BC) threshold, air-bone gap (ABG: 0.5, 1, 2, 4 kHz) were analyzed to evaluate surgical outcomes.
Statistical Analysis
SPSS Statistics 27.0 software (IBM SPSS) was used for data analysis. Data meeting a normal distribution are expressed as means ± standard deviations. A paired t test was used to compare preoperative and postoperative data. Categorical variables were compared using a chi-square test or Fisher’s exact probability test. A P value <.05 was considered to indicate statistical significance.
Results
Patient Characteristics
The patients ranged in age from 5 to 74 years, with a mean age of 43 years. The diagnosis was CSOM in 159 patients, AdOM in 21, and stage I acquired cholesteatomas in 17 (Figure 3).
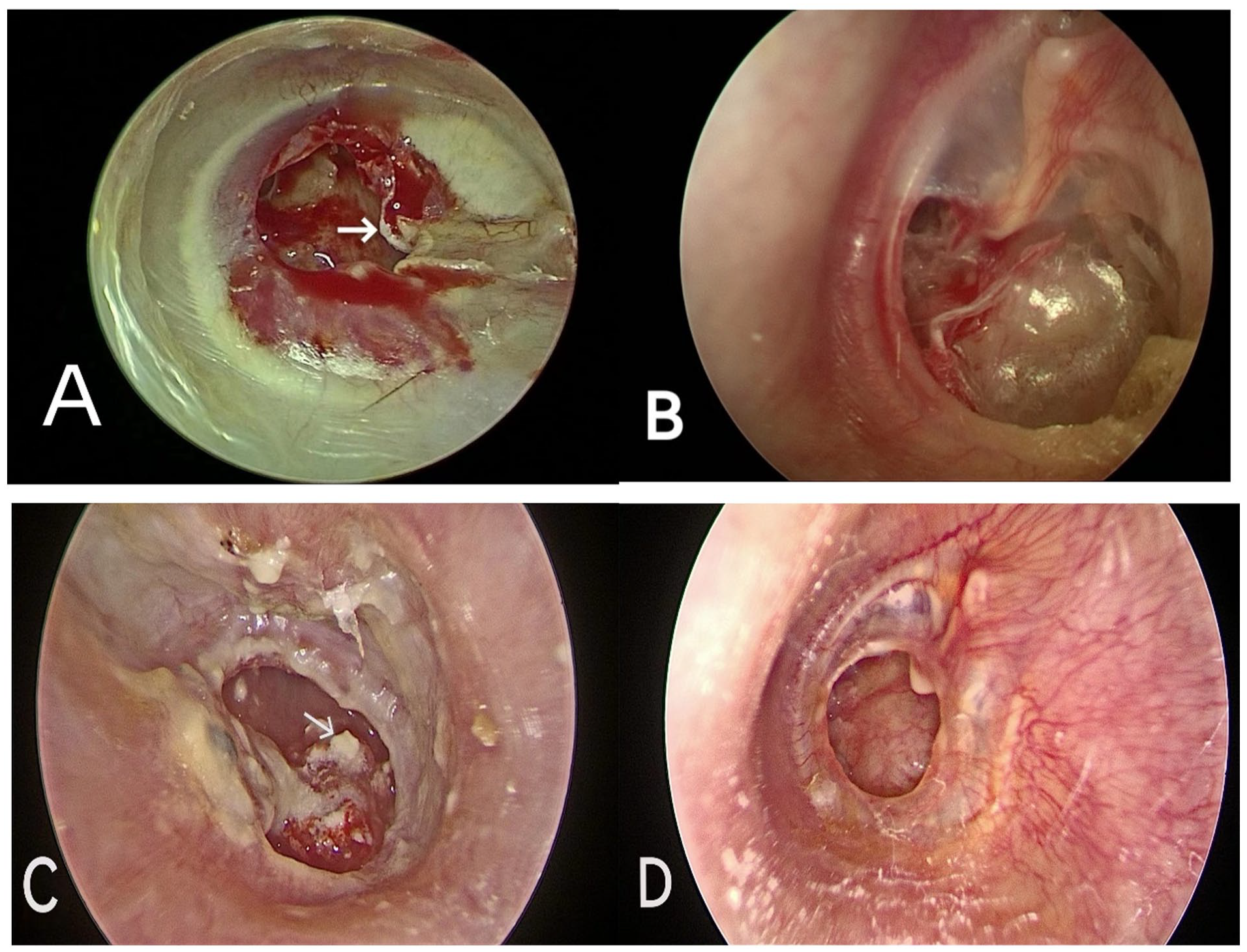
(A) An accumulation of keratinizing stratified squamous epithelium at the edge of the perforation identified during the postoperative histopathological examination. Cholesteatoma epithelium in a patient with secondary acquired cholesteatoma (stage I). (B) Adhesive otitis media. (C) Chronic otitis media with severe tympanic sclerosis. (D) Simple chronic otitis media without tympanic sclerosis or an accumulation of keratinizing stratified squamous epithelium at the edge of the perforation.
Comparison of the Surgical Side and Tympanum Condition Between Patients With and Without Remnant Squamous Epithelium
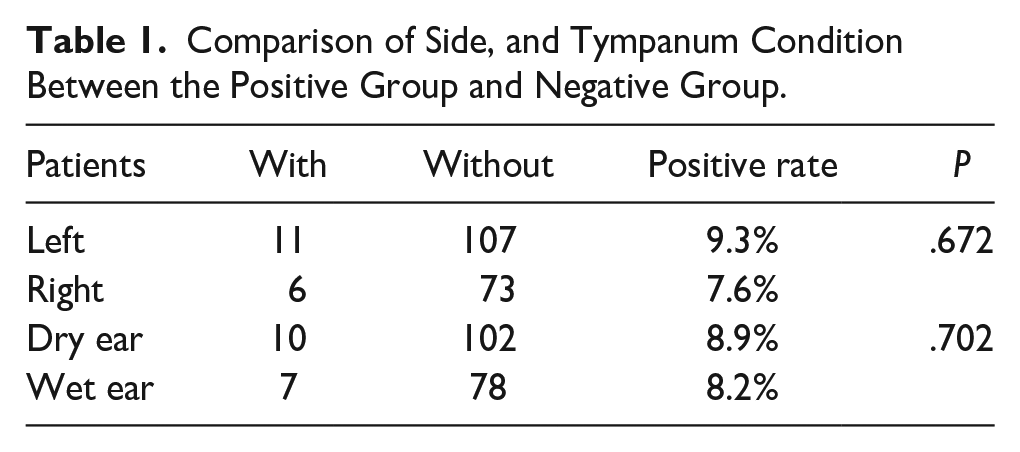
There was no significant difference in the surgical side (P = .672) or tympanum condition (P = .702) between patients with and without remnant squamous epithelium (Table 1).
Comparison of Side, and Tympanum Condition Between the Positive Group and Negative Group.
Detection Rate of Squamous Epithelium in Patients With AdOM, Acquired Cholesteatoma, and CSOM in Cases With and Without an Exposed Malleus
There was a statistically significant difference in the detection rate of squamous epithelium between the 3 groups; this was significantly higher (P < .001) in patients with acquired cholesteatoma than in those with AdOM or CSOM (Table 2). Although the rate was not significantly associated with exposure of the malleus handle (P = .06), as a result of 17 patients with acquired cholesteatoma were all in group 1 (exposed malleus handle), the detection rate was higher in this group than in group 2 (nonexposed malleus handle).
Comparison of the Detection Rate of Squamous Epithelium in Patients With AdOM, Acquired Cholesteatoma, and CSOM.
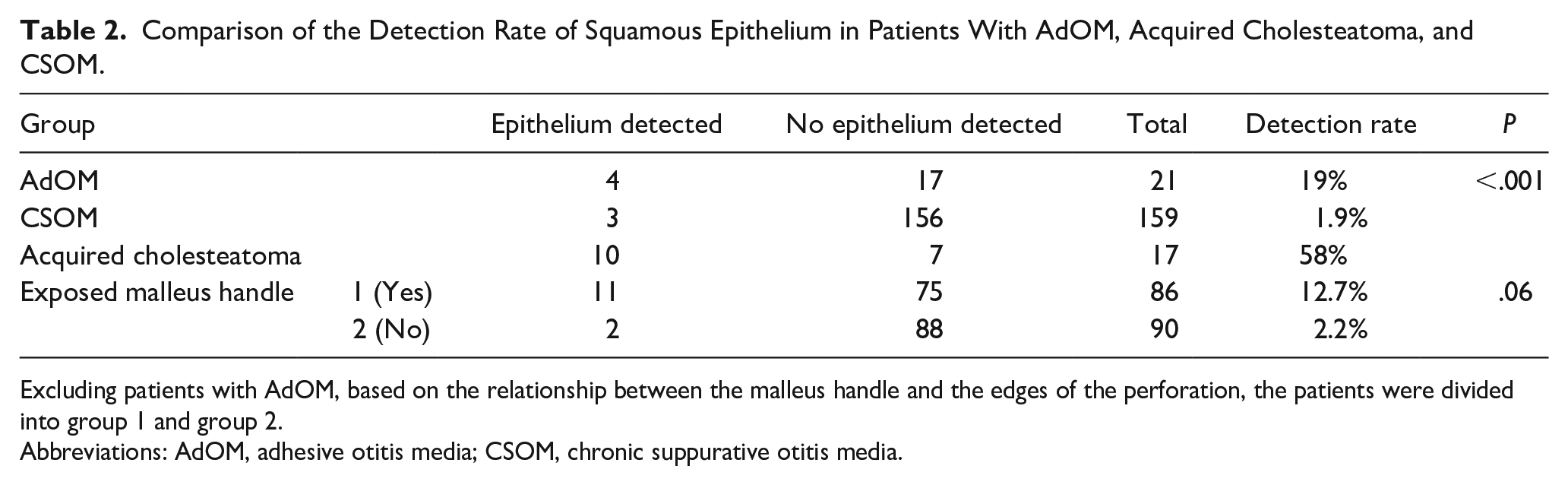
Excluding patients with AdOM, based on the relationship between the malleus handle and the edges of the perforation, the patients were divided into group 1 and group 2.
Abbreviations: AdOM, adhesive otitis media; CSOM, chronic suppurative otitis media.
Detection Rate of Squamous Epithelium at Different Stages of AdOM (Dornhoffer Criteria)
Squamous epithelium was detected in patients of all AdOM stages, and the detection rate did not differ significantly among the groups (P = .505, Table 3).
Detection Rate of Squamous Epithelium at Different Stages of AdOM (Dornhoffer Criteria).

Correlation Between the Presence of Squamous Epithelium and Microbial Infection of the Middle Ear
None of the 17 patients in whom residual squamous epithelium on the tip of the malleus handle was detected had evidence of middle ear infection (Table 4).
Detection Rate of Squamous Epithelium Depending on Microbial Infection of the Middle Ear.

Preoperative Versus Postoperative Mean ABG, BC, and Mean AC
The preoperative and postoperative PTA values differed significantly (Table 5). Specifically, the postoperative mean BC (P = .003), AC (P < .001), and ABG (P < .001) improved compared to the preoperative values.
Comparison of Preoperative and Postoperative Pure-Tone Audiometry (0.5, 1, 2, 4 kHz) Findings.
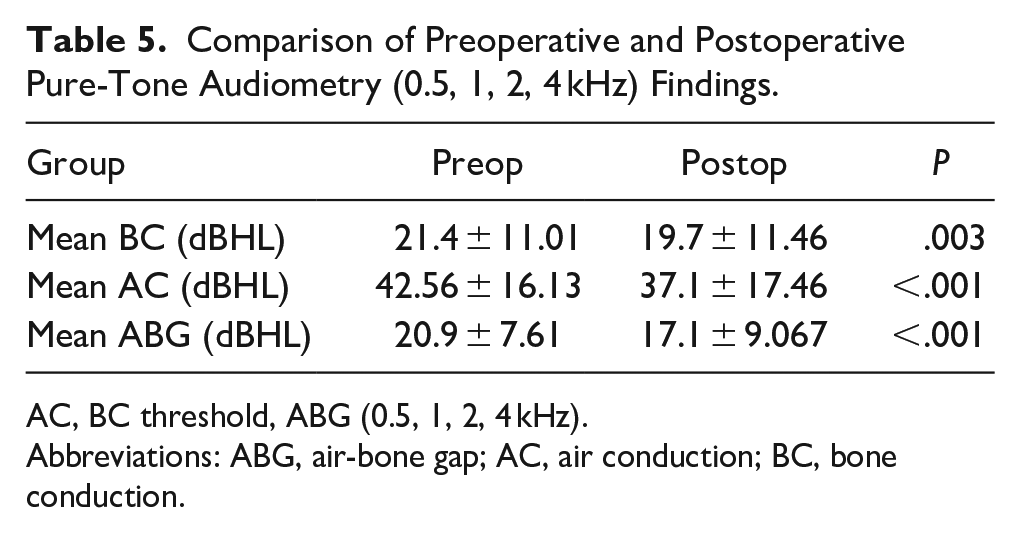
AC, BC threshold, ABG (0.5, 1, 2, 4 kHz).
Abbreviations: ABG, air-bone gap; AC, air conduction; BC, bone conduction.
Discussion
Although microsurgery is the traditional surgical technique for the treatment of chronic otitis media, endoscopic approaches are becoming increasingly adopted, given their advantage of “looking around corners.” The advantages of microsurgery include a magnified and illuminated surgical field, the ability to use both hands during surgery, binocular vision, and good depth perception. 6 By contrast, in middle ear endoscopic surgery, only one hand can be used for the surgical maneuvers and depth perception is poor. 7 As a result, in endoscopic surgery, more time is needed to resect the tissue around the tip of malleus handle, and the risk of severe perturbation of the ossicular chain is high.
Migration of the squamous epithelium of the tympanum into the middle ear through a perforation in the tympanum can lead to acquired secondary cholesteatoma. 8 The epithelium frequently enters the middle ear through the malleus manubrium. Thus, during tympanoplasty, strategies for managing the tissue around the tip of the malleus handle should be considered. Preventing the development of acquired secondary cholesteatoma after tympanoplasty requires determination of whether squamous epithelium remains around the tip of the malleus handle after meticulous elevation of the tympanomeatal flap. If the tissue around the tip of the malleus handle can be retained, this not only reduces the postoperative vertigo and loss of BC caused by the severe perturbation of the ossicular chain but also shortens the duration of surgery.
The postoperative pathology assessments of our patients revealed residual squamous epithelium around the tip of the malleus handle after meticulous elevation of the tympanomeatal flap in 17 of 197 patients: 10 with acquired cholesteatoma, 4 with AdOM, and 3 with CSOM complicated by tympanic sclerosis. The details follow.
The postoperative pathology revealed residual squamous epithelium around the tip of the malleus handle in 10 of 17 patients with acquired cholesteatoma. In all 10 cases, keratinizing stratified squamous epithelium was observed intraoperatively, involving the tendon of the tensor tympani and the inner sides of the malleus handle, associated with destruction of the upper tympanic chamber and ossicular chain. The epithelial migration theory seeks to explain the development of a secondary acquired cholesteatoma; tympanic membrane perforations allow the squamous epithelium of the tympanic membrane to migrate into the middle ear. Therefore, based on the intraoperative presentation, secondary acquired cholesteatoma was diagnosed. 9 In the other 7 patients with acquired cholesteatoma, there was no residual squamous epithelium on the tip of the malleus handle. In 3 of those patients, a retraction pocket had formed in which desquamated keratin epithelium had accumulated in the region of the pars flaccida, resulting in a primary acquired cholesteatoma.4,10 The pathogenesis of primary acquired cholesteatoma has been attributed to a failure of the Eustachian tube that causes negative pressure inside the tympanic cavity, leading to the creation of a retraction pocket. 11 Four patients with cholesteatoma presented with a whitish ovoid or round friable mass located in the anteromedial or posteromedial aspect of the perforated tympanic membrane and not involving the osseous chain. It was thus inferred that, in patients with primary acquired cholesteatomas or an isolated mass, the lesions were not significantly associated with the malleus handle, such that during tympanoplasty there is no need to completely remove the tissue around the tip of the malleus handle.
Rather, among patients with secondary acquired cholesteatomas exhibiting epithelial migration into the tympanum via the perforated edge of the tympanic membrane and manubrium mallei, during tympanoplasty 2 to 3 mm of scar tissue around the edge of the perforation should first be removed; the tympanomeatal flap should then be carefully and meticulously dissected from the malleus handle, followed by a complete removal of the tympanic lesion as well as the tissue around the tip of the malleus handle, to avoid recurrence.
Among the 21 patients with AdOM, 5 had stage II disease, 9 had stage III disease, and 7 had stage IV disease. In 4 of the patients (2 of stage II, 1 of stage III, and 1 of stage IV), the postoperative pathology suggested residual squamous epithelium around the tip of the malleus handle. The difference in squamous epithelium detection rate among the groups was not statistically significant (Table 3). Patients with AdOM frequently present with almost complete adhesion between the thin, retracted, atrophic pars tensa and the medial wall of the middle ear. The malleus handle may be encased in soft tissue debris. The middle ear mucosa may be proliferative, exhibiting granulation and sclerotic foci12,13 that make it very difficult to completely elevate a tympanomeatal flap. Consequently, the absence of squamous epithelium on tissue around the tip of the malleus handle is difficult to confirm. Thus, in patients with AdOM, the tympanomeatal flap should be carefully elevated, and the tissue around the tip of the malleus handle should be thoroughly removed.
Among the 159 patients with CSOM, 83 had tympanic membrane perforation without exposure of the malleus handle, 2 of whom had residual squamous epithelium around the tip of the malleus handle. In another 76 patients with tympanic membrane perforation and malleus handle exposure, 1 patient had residual squamous epithelium around the tip of the malleus handle. In these 3 patients, tympanic sclerosis was confirmed intraoperatively and it was suspected that small amounts of keratinizing squamous epithelium were attached to the edge of the tympanic membrane perforation, tympanic cavity, and/or to the tip of the malleus handle, potentially leading to acquired cholesteatoma. 14 The other 156 patients had no intraoperative signs of tympanic sclerosis and were considered to have simple chronic otitis media.
There were no significant differences in the postoperative detection rate of squamous epithelium around the tip of the malleus handle regardless of tympanic membrane perforation with the exposure of the malleus handle (P = .06, Table 2). Thus, for patients with CSOM without obvious sclerosis of the tympanic membrane and cavity and without an accumulation of squamous epithelium at the edge of the tympanic membrane perforation, that is, with simple chronic otitis media, regardless of tympanic membrane perforation and exposure of the malleus handle, tissue around the tip of the malleus handle can be retained during tympanoplasty. However, in patients with chronic otitis media and severe tympanic sclerosis, the tissue around the tip of the malleus handle should be completely removed.
Among our patients, the detection rate of squamous epithelium was significantly higher in those with acquired cholesteatoma than in those with AdOM or CSOM (P < .001, Table 2). Thus, compared to such patients, it is more important to thoroughly remove tissue around the tip of the malleus handle in those with secondary acquired cholesteatoma, and to resect the osteon eroded by the lesion.
In addition, surgical side and dry or wet ear conditions did not affect the detection rate of residual squamous epithelium around the tip of the malleus handle (Table 1). In this research, 68 of the 197 patients had a bacterial and/or fungal infection in the middle ear. One hundred twenty-nine of the 197 patients without detection of microbe in the middle ear, including 17 with squamous epithelium retention (Table 4). We infer that residual squamous epithelium around the tip of the malleus handle was not significantly associated with microbial infection of the middle ear, and that middle ear infection did not necessarily trigger migration of the squamous epithelium.
A comparison of preoperative and postoperative PTA results revealed an improvement in mean AC, mean BC, and mean ABG (Table 5), thus supporting tympanoplasty as an effective surgical technique to improve hearing loss in patients with different types of otitis media.15,16 However, other studies have shown that an inexperienced surgeon may cause excessive vibration of the ossicular chain during removal of the tissue around the tip of the malleus handle, leading to physical trauma to the ossicular chain and thus reduced BC. 17
Conclusion
Following tympanoplasty in patients with secondary acquired cholesteatoma, AdOM, or CSOM with severe tympanic sclerosis, residual squamous epithelium around the tip of the malleus handle was detected at a relatively high rate and was completely removed after careful and meticulous elevation of the tympanomeatal flap. In patients with simple chronic otitis media, that is, without tympanic sclerosis or an accumulation of keratinizing stratified squamous epithelium at the edge of the perforation, the tissue around the tip of the malleus handle can be retained, with the advantages of a shorter operation time and protection of the inner ear against physical trauma to the ossicular chain, in turn preventing a reduction in BC.
Footnotes
Acknowledgements
The authors thank the anesthetists and nursing team for their cooperation during surgical procedures. The authors also thank the audiologists for their assistance with pre-and postoperative audiological assessments.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (NSFC; grant nos. 82271166, 81970880 to DR) and Natural Science Foundation of Shanghai (grant no. 22ZR1410100 to DR). No conflicts of interest exist.
Ethics Approval Statement and Patient Consent Statement
The study protocol was approved by the Ethics Committee of the Eye, Ear, Nose, and Throat Hospital, Fudan University (approval number: 2020133). The patients’ consent for the clinical trial has been assigned before the operation.