
Abstract
Background:
To optimize the oto-endoscopic treatment of patients with adhesive otitis media (AdOM).
Methods:
In this observational retrospective cohort study, a total of 73 patients (81 ears) diagnosed with AdOM were included. Surgical interventions included insertion of the tympanotomy tube, tympanoplasty, or a combination of both. Follow-up evaluations were carried out at 2 weeks and at 1, 3, 6, and 12 months. Pure tone audiometry was administered between 1 and 3 months post-surgery, and imaging examinations were carried out at 6 months.
Results:
Tympanotomy tube insertion was performed in 11.1% (9 out of 81) of the cases, while tympanoplasty was performed in 79% (64 out of 81) of the cases, and both procedures were performed in 9.9% (8 out of 81). The rate of tympanoplasty increased with the Sade grade. Postoperatively, air conduction hearing and air-bone gap (ABG) in patients classified as Sade grades III to V showed a significant improvement.
Conclusions:
The individualized oto-endoscopic surgery significantly improves hearing outcomes in advanced AdOM (Sade grades III-V), as evidenced by reduced ABG. Patients with varying degrees of AdOM require customized treatment approaches.
Level of Evidence:
4.
Highlights
Tailored Surgical Approaches: The study emphasizes the importance of personalized treatment for patients with adhesive otitis media (AdOM), showcasing various surgical interventions, including tympanoplasty, tympanostomy tube placement, and combination of both, based on the severity of the condition.
Positive Postoperative Outcomes: Findings indicate a significant improvement in hearing outcomes and tympanic membrane (TM) healing in the majority of patients, with a substantial percentage reporting complete recovery from preoperative symptoms such as ear tightness and tinnitus.
Innovative Treatment Strategies: The research explores novel techniques, such as the use of tragal cartilage for TM reconstruction and combination placement of ventilation tubes, which contribute to enhanced healing and reduced risk of re-adhesion in patients undergoing surgery for AdOM.
Introduction
Adhesive otitis media (AdOM) is characterized by retraction of the tympanic membrane (TM) and extensive adhesion of it to the tympanic mucosa, partially or completely closing the tympanic cavity. The fibrous tissue adhesion restricts the movement of the middle ear sound transmission system, hindering middle ear ventilation and drainage. AdOM progression may compromise ossicular fixation or mobility, and trigger fibrosis and/or adhesion of the tympanic wall. Hearing is adversely affected. In more severe cases, AdOM can cause repeated infections and even cholesteatoma.
The TM of AdOM patients is typically intact, some have no clinical symptoms or only aural fullness. Progressive hearing loss, tinnitus, and other symptoms may develop. AdOM may coexist with various forms of middle ear inflammation or emerge as a sequela to such inflammation. 1 Although AdOM is often encountered by otologists, a universally accepted effective treatment remains elusive, AdOM is a challenging refractory disease. The surgical results of AdOM are generally poorer than those of chronic suppurative otitis media because it is difficult to address the Eustachian tube dysfunction associated with AdOM. Careful consideration of the surgical indications for AdOM is required to optimize treatment outcomes.
AdOM is often classified into stages based on the extent of TM retraction and adhesion. Sade et al 2 initially classified the progression of AdOM into 5 stages: I, mild retraction of the TM; II, retraction of the TM to the incus or stapes; III, TM in contact with the promontory without adhesion; IV, TM adherent to the promontory; and V, TM both perforated and adherent to the promontory. Such staging aids the clinician in assessment the severity of AdOM and could guide treatment decisions. However, there is no relevant literature. This study analyzes the utility of various oto-endoscopic treatments for AdOM of different grades. We evaluated symptom improvement, postoperative hearing outcomes, and complications to establish criteria for the selection of different surgical treatments based on different conditions in patients with varying degrees of AdOM.
Study Design and Patients
This was an observational, retrospective cohort study conducted at the Department of Otorhinolaryngology of the Eye, Ear, Nose, and Throat Hospital affiliated with Fudan University. We included 73 patients (81 ears) diagnosed with AdOM who underwent endoscopic treatment between January 2020 and February 2022 (Figure 1).
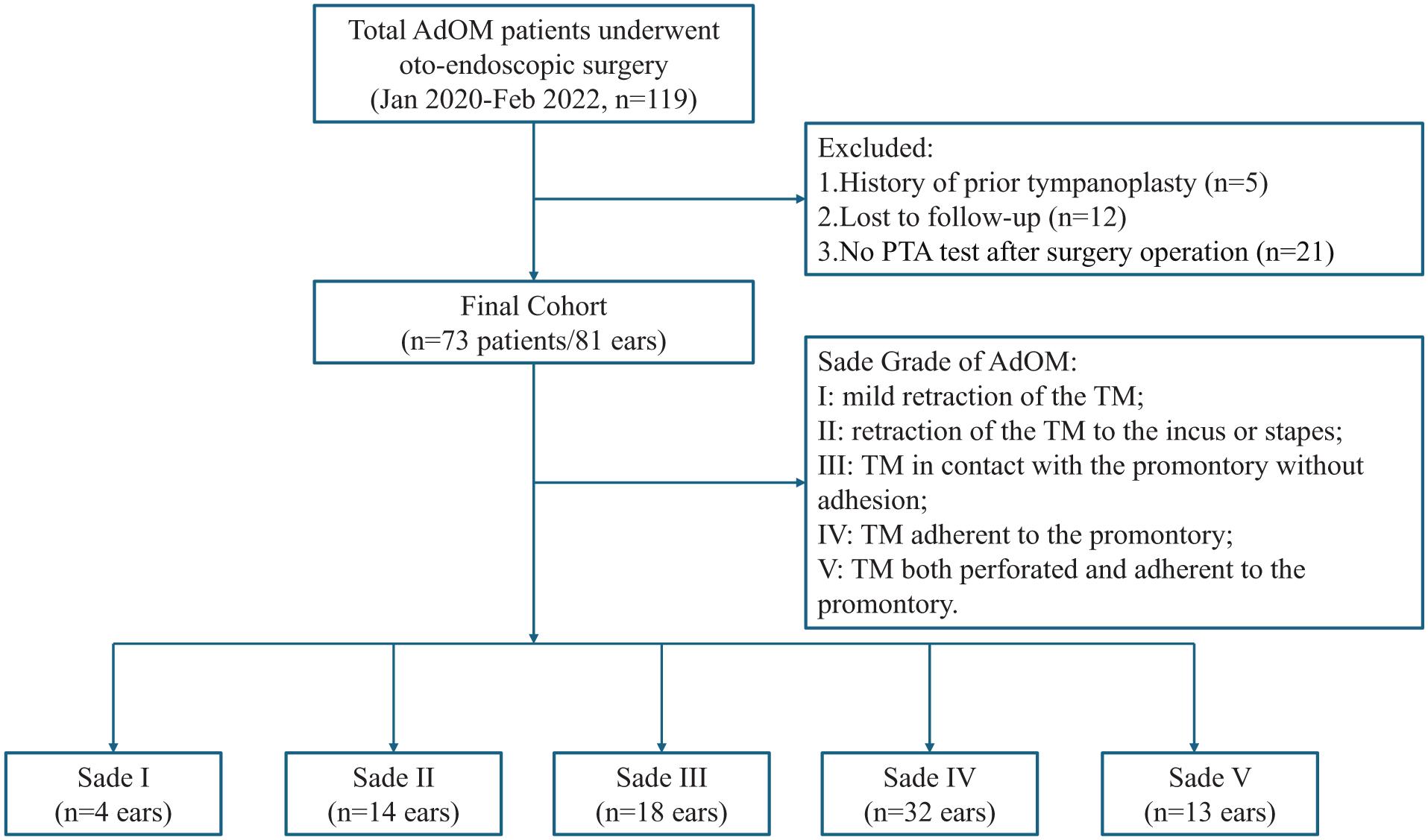
A STORBE flowchart.
Inclusion Criteria: (1) Patients with a confirmed diagnosis of AdOM who underwent endoscopic surgery. (2) Preoperative evaluation including: aural endoscopy, pure tone audiometry, and high-resolution temporal bone computed tomography (HRCT). If a lesion was found in the tympanic cavity, magnetic resonance imaging and diffusion-weighted imaging (MRI + DWI) were performed. The average bone conduction (BC) and air conduction (AC) thresholds across the 0.25 to 4 kHz frequency range were analyzed. And the pure-tone average (PTA) and air-bone gap (ABG) in the expanded speech frequency (0.25-2 kHz) were calculated. (3) A pure tone audiometry evaluation was completed during postoperative follow-up. Exclusion Criteria: (1) Patients who had a history of prior tympanoplasty. (2) Patients who had active lesions in the nose or nasopharynx were excluded. (3) Patients lost to follow-up within the first postoperative year were excluded. The staging of AdOM was based on the Sade grading system. 2
This study was carried out after written informed consent was obtained from the patients, in accordance with the Declaration of Helsinki, and was approved by the Medical Ethics Committee of the Eye and ENT Hospital of Fudan University (approval number: 2023006).
Surgical Techniques
All patients were operated on under general anesthesia by 1 experienced surgeon. The choice of surgical method was based on the PTA data, the preoperative imaging results, the mucosal integrity of the tympanic cavity, and the condition of the pharyngeal tube orifice. The surgical options included insertion of tympanotomy tube (Figure 2), tympanoplasty (Figure 3), or both (Figure 4). Tympanic catheterization was the preferred intervention when the ABG was <25 dB and HRCT revealed no obvious lesion. If ABG was ≥25 dB or HRCT showed a lesion in the middle ear cavity or an ossicular chain injury, tympanoplasty was considered. During tympanoplasty, the integrity of the mucosa of the tympanic cavity and the condition of the nasopharyngeal orifice were examined. Tympanotomy tube insertion was contemporaneous with tympanoplasty if the tympanic orifice of the Eustachian tube was blocked and/or the mucosal of the tympanic cavity loss exceeded 50%; otherwise, tympanoplasty was performed alone (Figure 5).
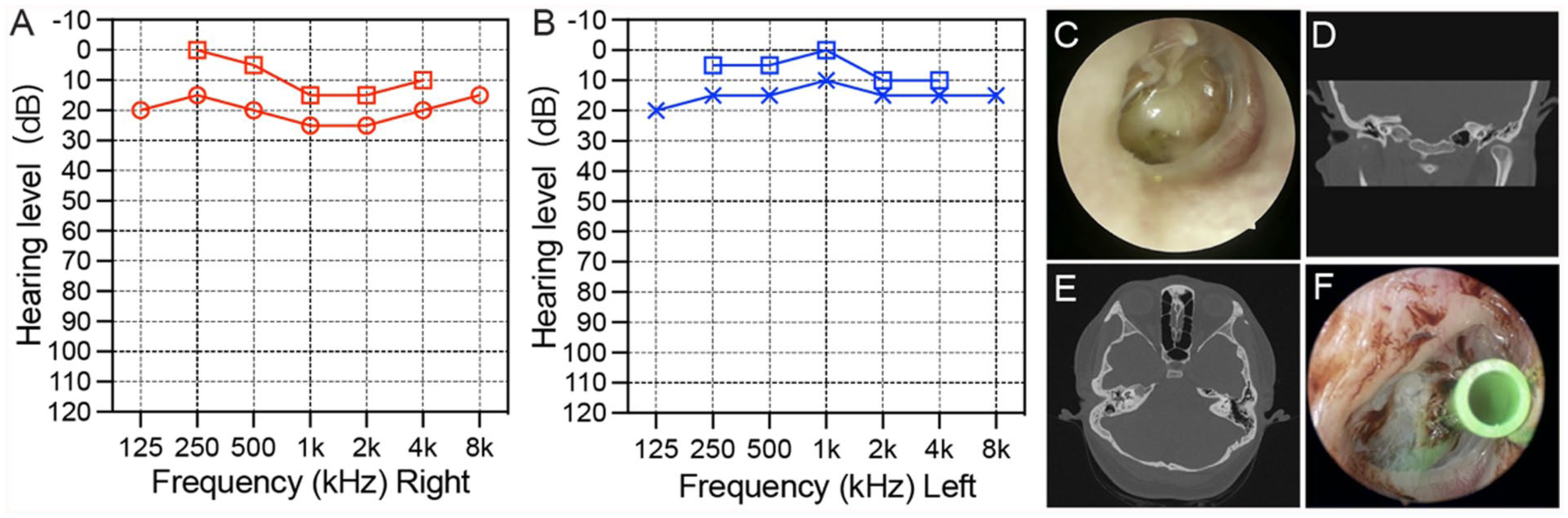
The patient was a 32-year-old woman who complained of tightness and hearing loss in right ear for more than 2 years. (A, B) The audiogram showed mild hearing loss in the right ear. (C) Endoscopic examination of the right ear revealed fluid in the tympanic cavity with TM contacting to the promontory without adhesion. (D, E) CT scan of the temporal bone showed chronic mastoiditis and soft tissue lesions in the right middle ear cavity. (F) Tympanotomy tube insertion in right ear. CT, computed tomography; TM, tympanic membrane.
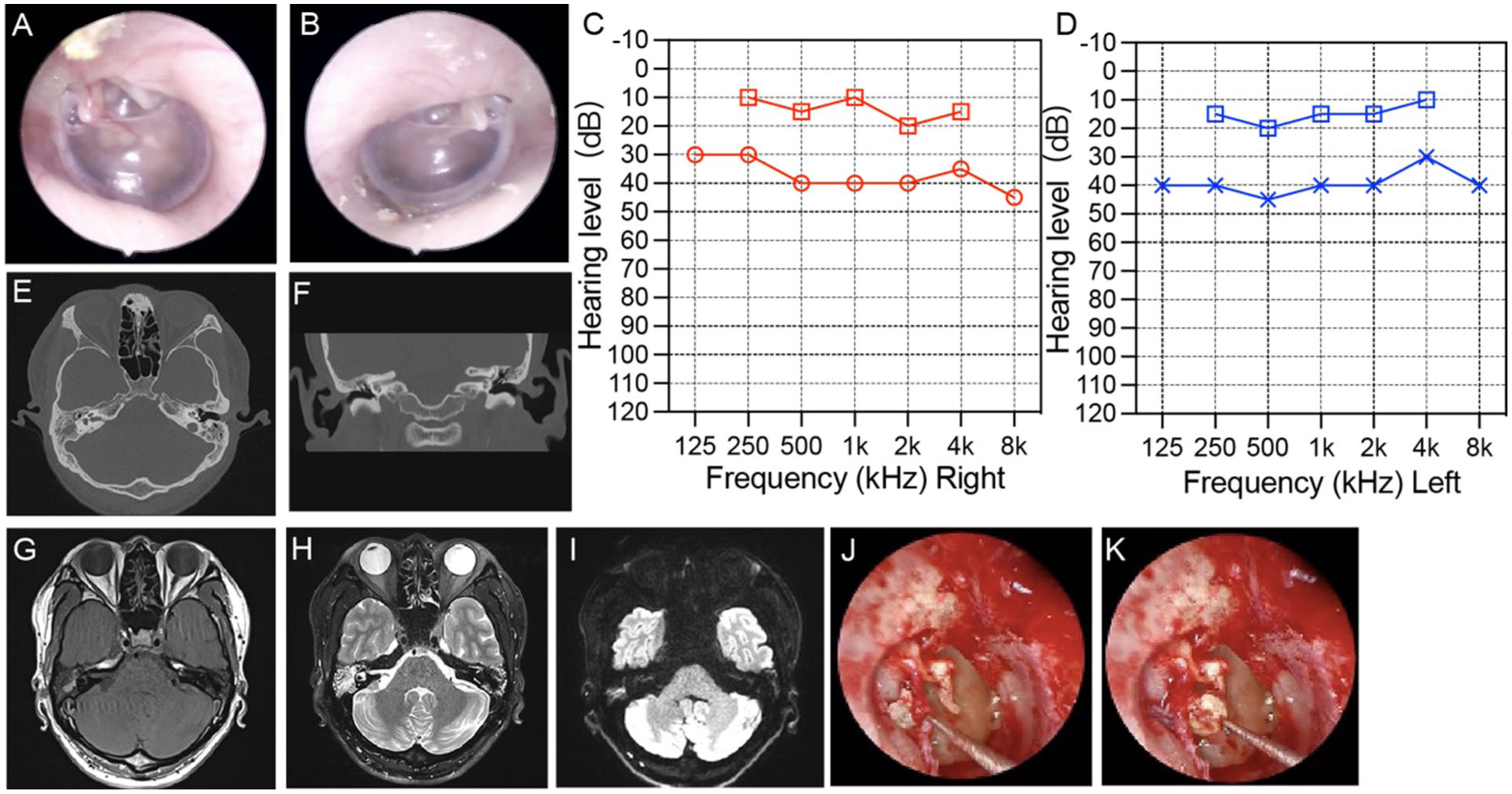
(A, B) The male, 31 years old, had bilateral TM invagination, which obviously in posterior and upper part of TM. AdOM Sade “stage II” in both ears. (C, D) The audiogram showed mild hearing loss in both ears. (E, F) CT showed bilateral middle ear mastoiditis, right tympanic sinus soft tissue lesions. (G–I) MRI showed bilateral middle ear mastoiditis, right tympanic sinus with cholesterol granuloma probably. (J, K) The right tympanoplasty and the cholesteatoma around the tympano-ossicular chain were found during the operation. AdOM, adhesive otitis media; CT, computed tomography; MRI, magnetic resonance imaging; TM, tympanic membrane.
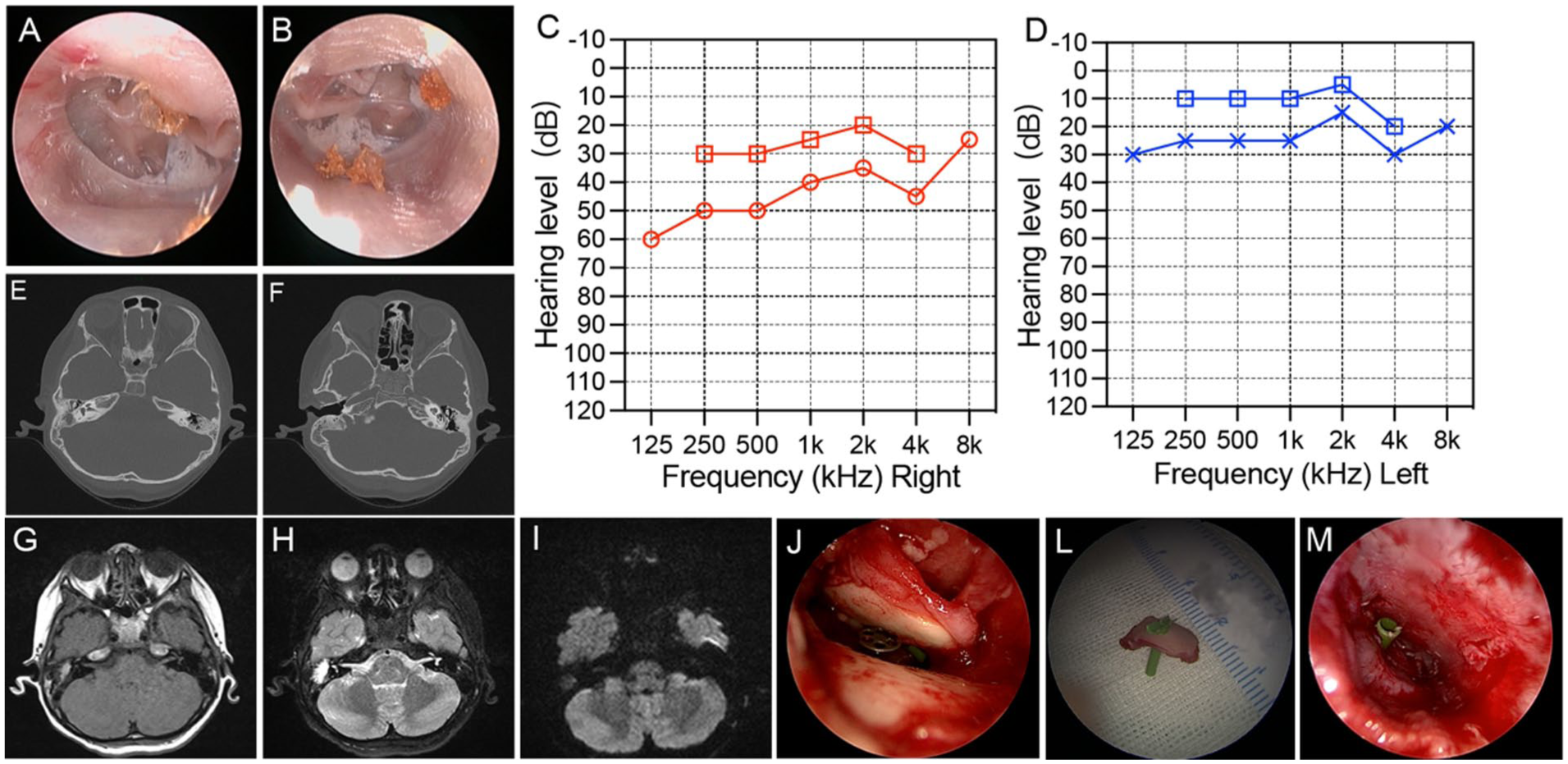
(A, B) The 9-year-old boy had bilateral TM adhere with promontory, graded as AdOM Sade “stage IV” in both ears. (C, D) He had hearing loss in both ears for 4 years. The left ear audiogram showed mild conductive hearing loss, and the right ear audiogram showed moderate mixed hearing loss. (E, F) CT examination showed low-density soft tissue lesions in the right tympanic sinus and partial bone absorption in the right incus. Decreased opacity in a few mastoid chambers on the left ear. (G–I) MRI showed poor gasification of the right ear mastoid, abnormal signal shadow in the middle ear mastoid region, contour signal on T1WI, high signal on T2WI, and a small amount of slightly high signal shadow in the tympanic sinus region on DWI, suggesting the possibility of cholesterol granuloma in the middle ear. Small amount of high signal fluid on T2WI in the left mastoid air chamber. (J–M) Right tympanoplasty, ossicular chain PORP reconstruction, and tympanotomy tube insertion had been performed. AdOM, adhesive otitis media; CT, computed tomography; DWI, diffusion-weighted imaging; MRI, magnetic resonance imaging; TM, tympanic membrane.
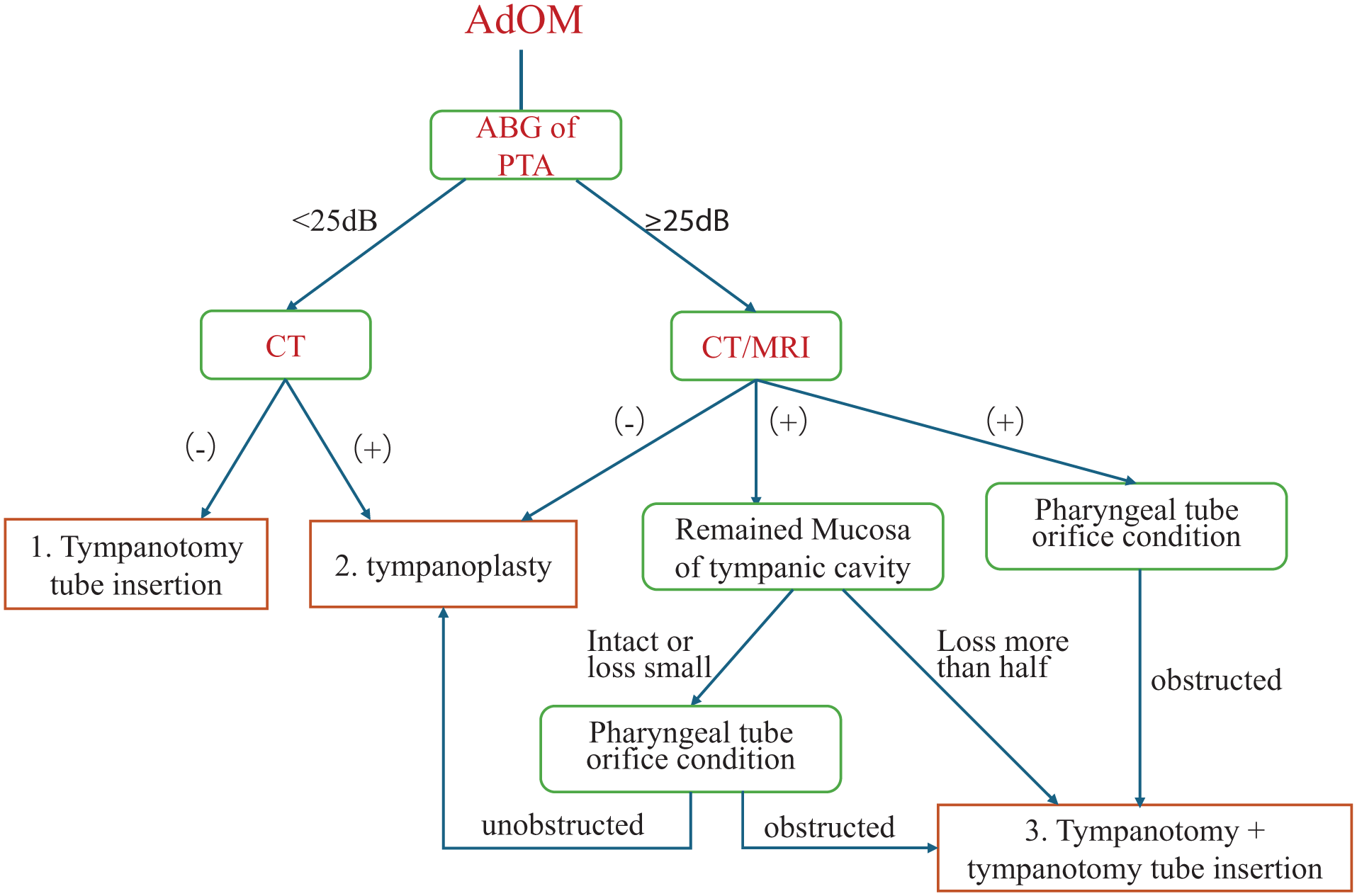
The surgery workflow of AdOM. AdOM, adhesive otitis media.
Tympanotomy tube insertion was performed under direct visualization using oto-endoscope. The catheterization site was carefully selected in the anterior upper or lower quadrant of the TM, and a silicone T-tube was inserted (Figure 2).
At the beginning of the tympanoplasty, a circular incision was created 1 cm from the tympanic ring to allow cutting of a tympanic canal flap. The skin of the external auditory canal and the TM was meticulously stripped from 2 to 6 o’clock. The adherent TM was carefully elevated off the ossicles and medial wall of the tympanic cavity. This facilitated exposure of the cavity, allowing a thorough search for lesions such as cholesteatoma or granulation. If a cholesteatoma was suspected based on preoperative evaluations or observations during surgery, the bone of the lateral wall of the upper tympanic chamber was delicately ground away. Crucially, this exposed the tympanic sinus and facilitated thorough cleaning of the cholesteatoma. Ossiculoplasty was performed in patients with damaged ossicles. The surgeon selected among partial ossicle reconstruction, total ossicle reconstruction, and ossicular chain release based on the severity of the damage (Figure 3).
The ipsilateral tragus cartilage was harvested, carefully trimmed, and both the cartilage and its ear canal-side perichondrium were preserved for TM reconstruction. Intraoperatively, if the Eustachian tube function was poor, or if the orifice of the pharyngeal tube was adherent, and/or mucosa of the tympanic cavity was lost after cleaning lesions in the tympanic cavity (including granulomas, cholesterol granulomas, cholesteatomas), TM catheterization was performed. A hole was created in the cartilage, and a ventilation tube was inserted (Figure 4).
Postoperative Follow-Up
All patients were initially followed up in the outpatient clinic 2 weeks after surgery, and then 1, 3, 6, and 12 months after surgery. At the first follow-up visit, we evaluated the repair of the TM healing and the position and patency of any TM ventilation tube. At each follow-up, we asked all patients if they experienced ear tightness, tinnitus, otorrhea, or poor hearing. After at least 6 months of follow-up, ventilation tubes were removed under endoscopic guidance when the following criteria were met: (a) intact TM reconstruction, (b) aerated middle ear space on Valsalva maneuver, and (c) absence of effusion for ≥3 consecutive monthly examinations. PTA was performed 1 to 3 months after the operation, and imaging 6 months after the operation, to examine the air content of the tympanum and the status of residual or recurrent lesion. Reoperation was considered when either (a) persistent ABG >30 dB at 6 month audiometry, or (b) CT evidence of recurrent cholesteatoma.
Statistical Analysis
Clinicodemographic data were presented as means (standard deviations) for normally distributed data, or medians (interquartile range) for non-normally distributed data, and counts with percentages for categorical data. As some patients exhibited binaural AdOM, and as hearing was measured repeatedly (before and after the operation), the outcomes were correlated within patients. Thus, to estimate the effect of surgery on hearing improvement as well as whether there was evidence of other influential factors related to the change of hearing levels, generalized estimating equation (GEE) was applied, which is one of the commonly used statistical technique for longitudinal analysis, that is, applicable to broad data type. It can be performed in continuous or categorial outcomes regardless of their contributions and allows for analysis in the data with missing values and estimate the parameters with maximum likelihood technique. The efficacy of surgery on hearing (AC, BC, and ABG) was initially explored using univariate GEE models, in which surgery, time (pre- and post-operation), and the Surgery × Time interaction was included to estimate changes of hearing after surgery. Then, the efficacy of surgery was estimated in the multivariate models adjusting for the influential covariates, including imaging examination, ossicle damage, and mastoid. The change patterns of hearing levels pre- and post-operation were further analyzed in different Sade grading subgroups. Since GEE focused on the average effect of the group rather than the individual variations, the clustering structures of the data within group were specified, and the differences of model fitness were compared in the sensitivity analysis. The improvement of models was assessed with Quasi Information Criterion (QIC), and model with a smaller value of QIC often presented better goodness of model fit. RStudio (Posit, version 2023.06.0) was used for all statistical analysis and data plotting. Statistical significance was established to a two-sided P < .05.
Results
Characteristics of the Patient
Of the 73 patients, 33 (45.2%) were male and 40 (54.8%) were female. Eight patients were binaural, with an average age of 44 years (range: 5-74 years). Forty-eight point one percent of all patients reported ear tightness, and 46.9% tinnitus, before surgery. The average PTA threshold (0.25-2 kHz) of all 81 ears indicated conductive hearing loss, and about 49.4% of the ears had an ABG ≥25 dB; the proportion increased with the Sade’s grade. Preoperative HRCT and/or MRI + DWI showed that 54.3% of the ears had cholesterol or granulomatous lesions in the middle ear cavity, and 24.7% had cholesteatomas (Table 1).
Basic Information of Patients.
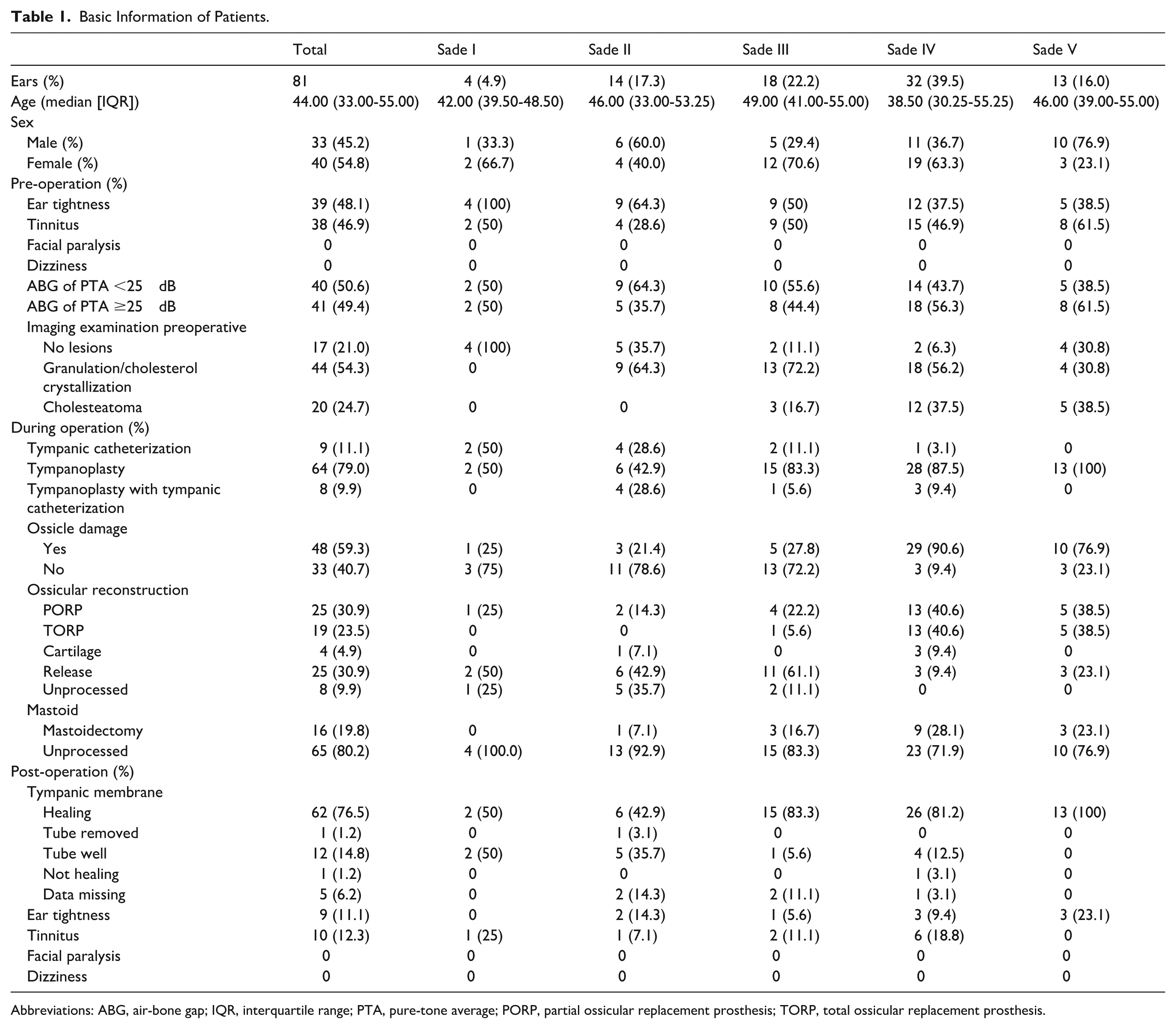
Abbreviations: ABG, air-bone gap; IQR, interquartile range; PTA, pure-tone average; PORP, partial ossicular replacement prosthesis; TORP, total ossicular replacement prosthesis.
The choice of surgical method was based on the PTA data, the preoperative imaging results, the integrity (or lack) of the mucosa of the tympanic cavity, and the condition of the orifice of the pharyngeal tube. Tympanotomy tube insertion (Figure 2), tympanoplasty (Figure 3), and a combination of both (Figure 4) were the 3 main types of surgery (11.1% [9/81], 79% [64/81], and 9.9% [8/81] of ear, respectively). The proportion of tympanoplasty increased with Sade grade. Sade grades IV and V ears exhibited a higher incidence of ossicular chain injury than the others. Of all patients, 19.8% underwent partial endoscopic mastoidectomy, which including the atticotomy or atticoantrotomy, the mastoid bone was drilled away in an aqueous environment (Table 1).
Postoperative TM Healing, Symptom Recovery, and Imaging Data
The ears that underwent tympanoplasty (79.0%; n = 64/81) involved TM reconstruction using ipsilateral tragus cartilage. Follow-up assessments of TM status from 1 to 6 months postoperatively showed that 96.9% of ears (62 out of 64) demonstrated excellent healing, although data for 1 ear were lost. One patient presented with a small fissure at the edge of the TM, indicating that it had not fully healed (Table 1).
Eight ears (9.9%; 8 out of 81) underwent both tympanoplasty and placement of the tympanostomy tube, using tragal cartilage for TM repair. Perforations were created in the center of the cartilage for the insertion of the tympanostomy tube. Nine ears (11.1%; 9 out of 81) received only tympanic catheterization. Follow-up evaluations of TM status from 1 to 6 months postoperatively indicated that 1 tympanostomy tube could be removed due to excellent TM healing. Furthermore, 70.6% (12 of 17) of the ears exhibited well-positioned tubes, although data for 4 ears were lost (Table 1).
Of all ears, 48.1% (39 out of 81) reported tightness before the operation. At 1 month postoperative follow-up, 24 ears had fully recovered, 7 showed improvement, 2 did not improve, and data for 6 ears were lost. Additionally, 46.9% (38 out of 81) of the ears experienced tinnitus before the operation. Postoperatively, 28 ears fully recovered, 7 improved, and 3 did not show improvement. In particular, no patients experienced facial paralysis or dizziness after the operation (Table 1).
Six months after operation, HRCT was used to assess the air content of the tympanum, the recovery of the repaired TM invagination, and the status of adhesion, residual, or recurrent lesions. Eight ears (9.9%; 8 out of 81) had air-filled tympana and demonstrated significantly improved hearing. In 6 ears (7.4%; 6 out of 81), the tympana were observed to be filled with lesions. MRI + DWI confirmed that 1 patient experienced a recurrent cholesteatoma that required reoperation.
Postoperative Hearing
PTA was performed 3 months after the operation. Preoperative and postoperative AC and BC were plotted and analyzed according to Sade grade. Compared to the AC threshold before surgery, the threshold after surgery improved significantly from 0.25 to 2 kHz (Figure 6A). The postoperative AC of Sade grades III to IV patients improved significantly (Figure 6B). Compared to the preoperative BC threshold, the postoperative threshold slightly improved (Figure 6C), mainly in patients of Sade grade IV or V (Figure 6D), from 0.25 to 2 kHz. The GEE showed that 3 months after surgery, the average AC threshold decreased significantly in patients of Sade grades III to V (Figure 7A and Table 2). The average AC decreased after surgery by 6.83 dB (95% confidence interval [CI] −10.97 to −2.69, P = .001) for patients of Sade grade III (Table 2). There was no significant difference in the average BC threshold before and after surgery, except for a slight increase in patients of Sade grade I (Figure 7B and Table 2). The ABGs of Sade grades III to V patients decreased significantly (Figure 7C and Table 2). Postoperative AC and ABG improved significantly in patients of Sade grades III to V (Table 2, Figures 7A and 7C).
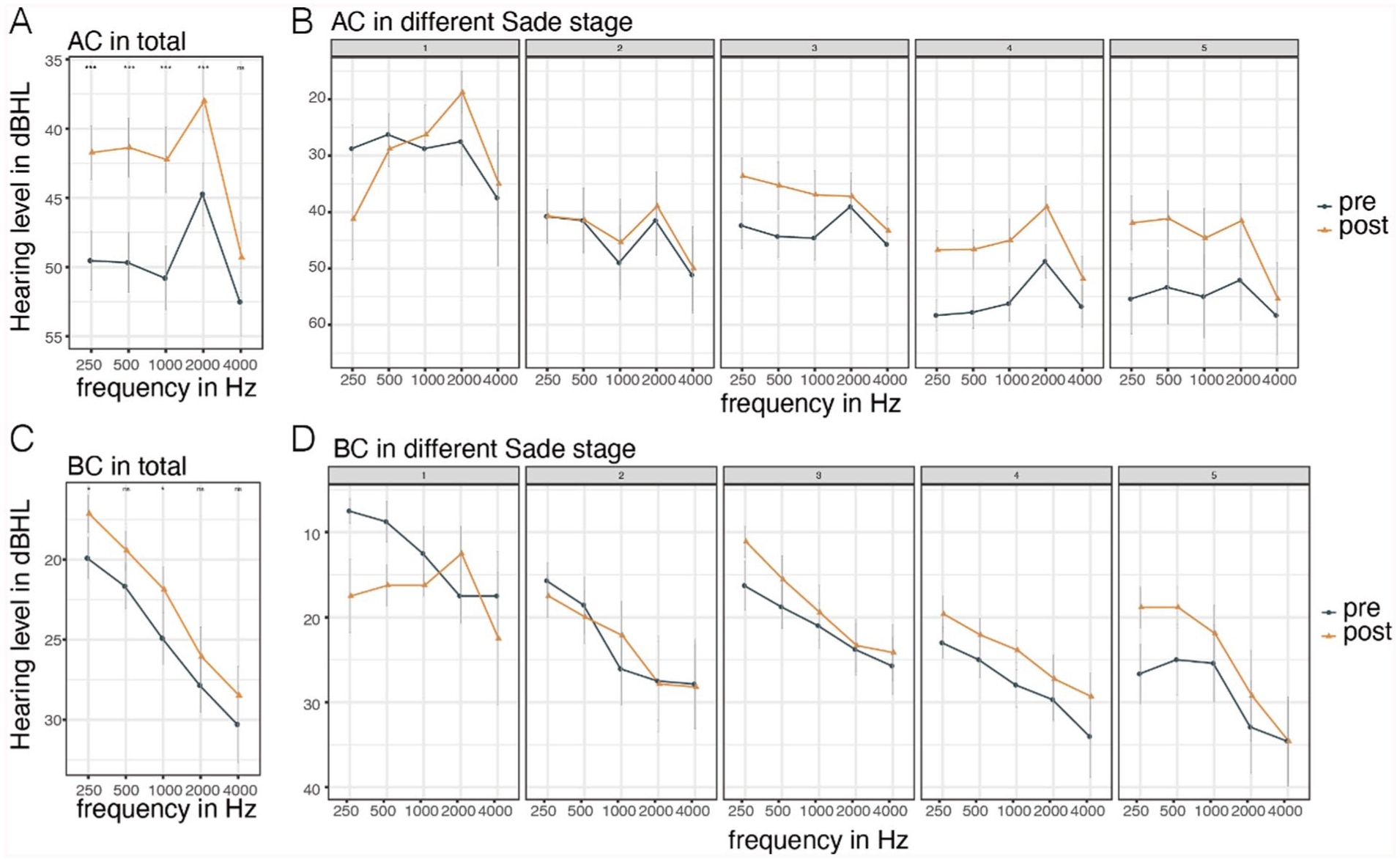
Comparison of audiogram before and after operation. (A) Compared with preoperative AC, postoperative AC at 0.25 to 2 kHz was significantly improved. (B) The patients were grouped according to Sade grading, and the preoperative and postoperative AC audiogram were shown, respectively. (C) Compared with preoperative BC, postoperative BC at 0.25 and 1 kHz was significantly improved. (D) The patients were grouped according to Sade grading, and the preoperative and postoperative BC audiogram were shown, respectively. AC, air conduction; BC, bone conduction.
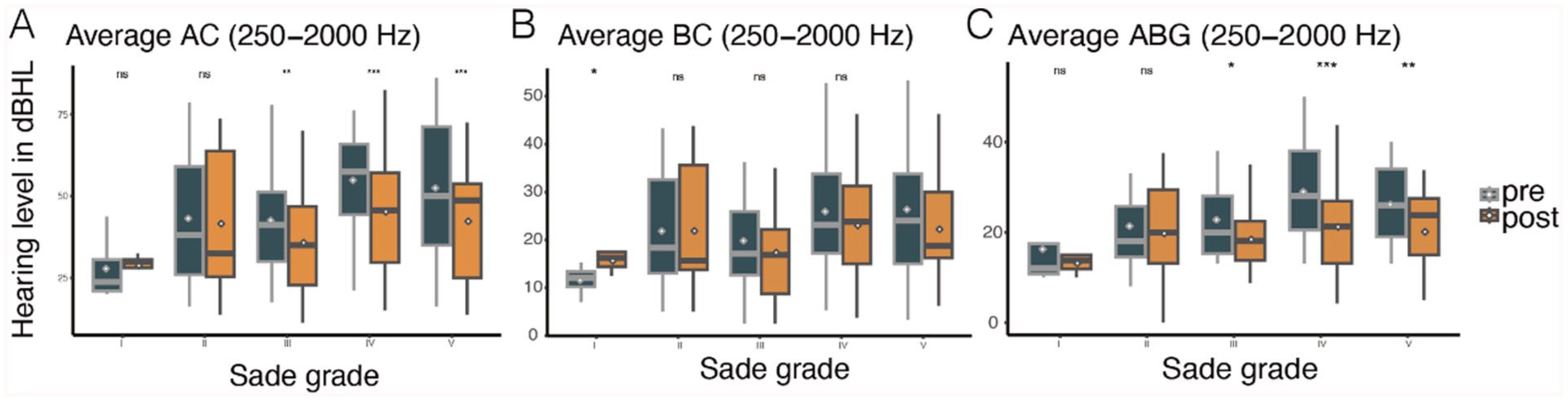
Comparison of mean threshold of hearing before and after surgery based on Sade grading. (A) The results of GEE showed that the AC threshold of patients in Sade grade III to V group was significantly improved after surgery compared with preoperative. (B) There was no significant difference in BC threshold before and after surgery, except in Sade grade I group. (C) The ABG of patients in groups III to V was significantly improved after surgery compared with preoperative. ABG, air-bone gap; AC, air conduction; BC, bone conduction; GEE, generalized estimating equation.
Comparing the Difference of Hearing Between Postoperative and Preoperative.
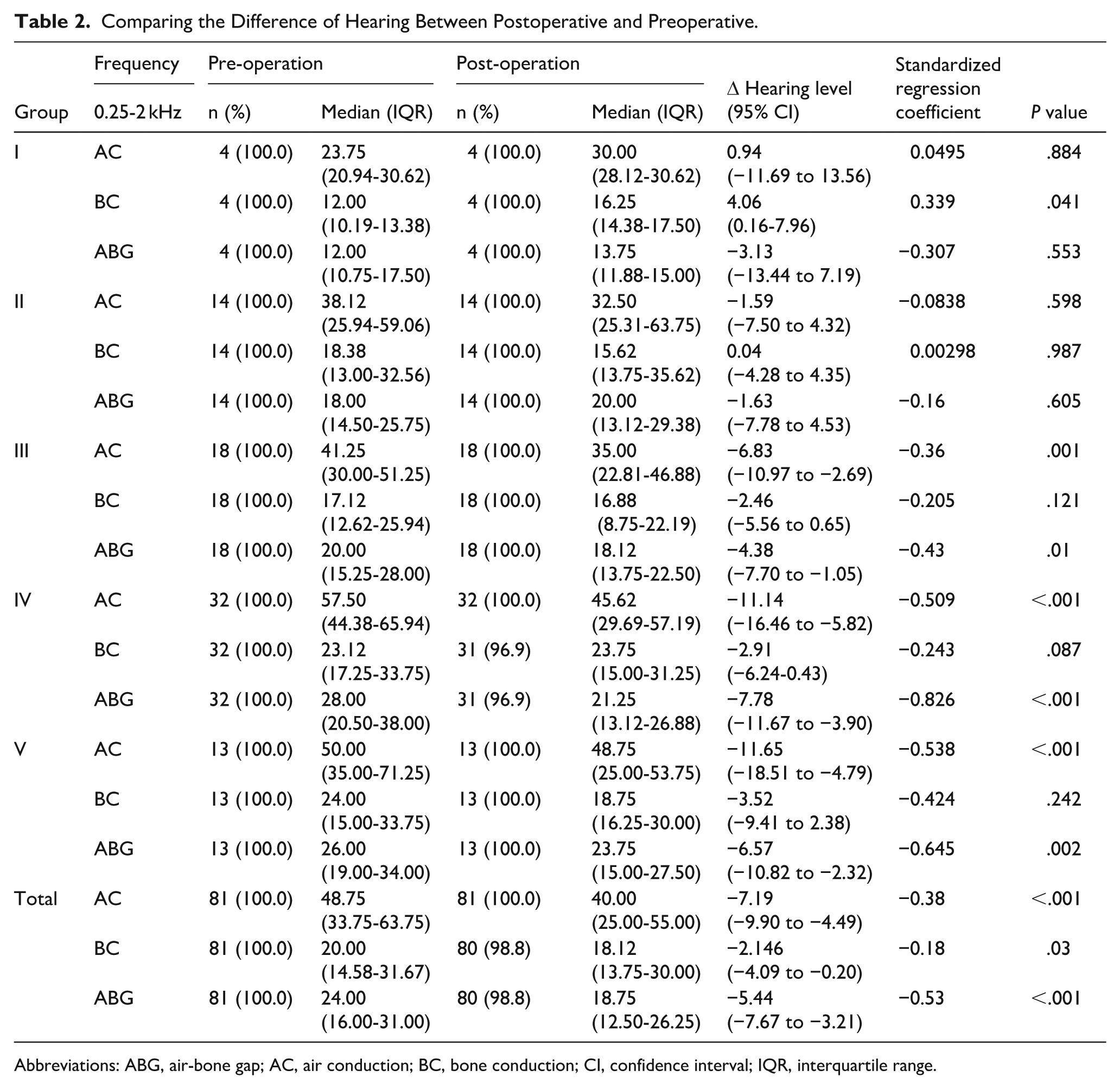
Abbreviations: ABG, air-bone gap; AC, air conduction; BC, bone conduction; CI, confidence interval; IQR, interquartile range.
We also explored the effects of clinical factors and found that the lesion characteristics on preoperative imaging, and ossicle and mastoid damage, significantly affected AC and ABG. Soft tissue lesions on the middle ear, tympanic cholesterol granulomas, cholesteatomas, ossicular chain disruption, and surgical involvement of the mastoid reduced hearing recovery (all P < .05). After controlling for the effects of these factors, the curative effects of surgery remained significant. The average AC decreased by 7.19 dB (95% CI −9.90 to −4.49, P < .001, Figure 8) and the average ABG by 5.43 (95% CI −7.66 to −3.21, P < .001, Figure 8). Although Sade grades III to V patients enjoyed somewhat better AC and ABG results, the differences were not statistically significant (Figure 8). After standardizing the covariates as well as hearing levels, the standardized coefficients that measured the effect size of each covariate for hearing threshold changes were identified. Soft tissue lesions, tympanic cholesterol granulomas, cholesteatoma and ossicle damage had the greatest impact on the hearing level damage, while operation was the most efficient cure for hearing improvement in ABG (Figure 8, Supplementary Tables 1 and 2).
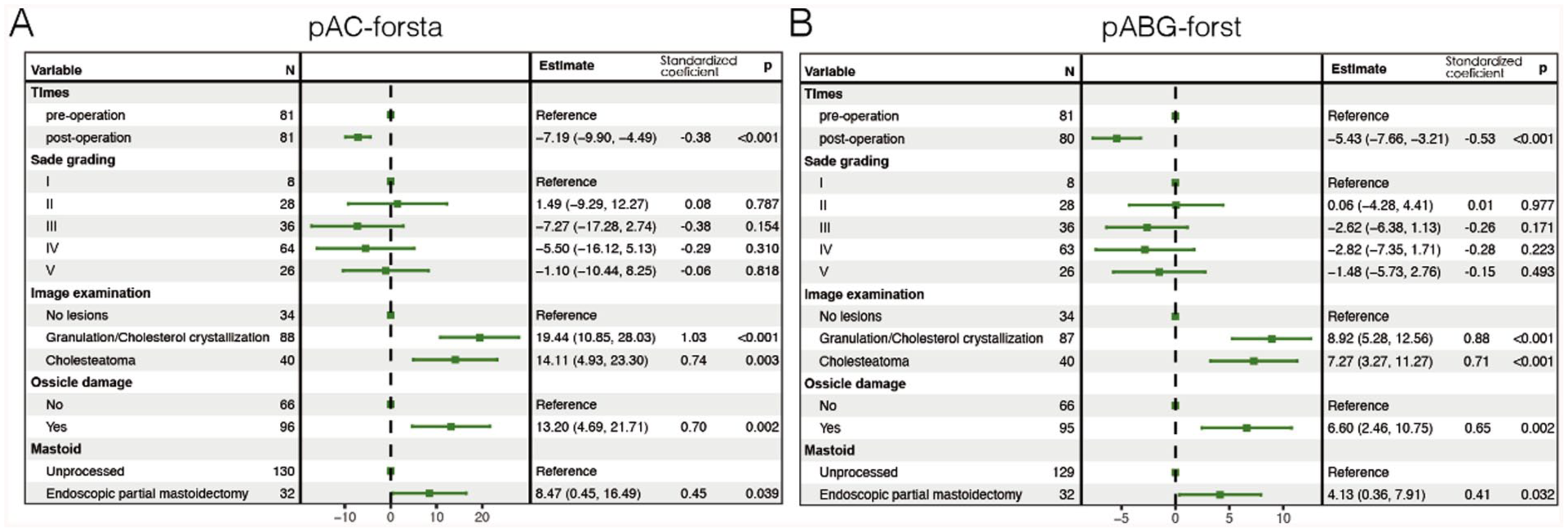
Forest plot for the multivariate GEE models estimating the efficacy of surgery on hearing (average AC threshold and ABG of hearing). Estimates were the parameters with 95% CI for the primary predictor (surgery) and covariates. Standard coefficients were the effect size for the covariates that compared the magnitudes of the covariates that measured at the same scale, like the Sade grading or imaging examination. Higher standard coefficient suggested stronger impact on the outcomes. Forest plots presented the estimates of efficacy of surgery on hearing and the effects of other predictors adjusting in the models. Compared with pre-operation, average AC was estimated to drop 7.19 dB HL (95% CI −9.90 to −4.49, P < .001), and ABG was estimated to drop −5.43 (95% CI −7.66 to −3.21, P < .001). The Sade grades of AdOM had no significant effect on the recovery of AC and BC after operation (P > .05). Imaging findings of middle ear lesions (soft tissue lesions, tympanic cholesterol granuloma, cholesteatoma), ossicular chain disruption, and surgical involvement of mastoid may affect hearing recovery (P < .05). Granulation or cholesterol crystallization found in images was supposed to have stronger impact on hearing exacerbation, with higher standard coefficients than that of cholesteatoma (1.03 vs 0.74 estimated in GEE models for AC). ABG, air-bone gap; AC, air conduction; AdOM, adhesive otitis media; BC, bone conduction; CI, confidence interval; GEE, generalized estimating equation.
Reoperation
One ear (1.2%, n = 1/81) required reoperation 6 months after the initial procedure to treat recurrent cholesteatoma.
Discussion
AdOM is usually a late-stage form of secretory otitis media, but it can also be a sequel of chronic suppurative otitis media. While the precise etiology of AdOM remains unclear, current evidence suggests that impaired Eustachian tube function plays a significant role, despite the challenges in definitively establishing this relationship.3 -6 Recent data from a large systematic review demonstrate that tympanoplasty can successfully restore hearing in 70.7% of chronic otitis media cases. 7 Nevertheless, AdOM continues to present substantial clinical challenges, with treatment outcomes often proving inconsistent. The management of AdOM cases without otorrhea remains particularly contentious, 5 with no established consensus in current guidelines. In this study, we advocate for early intervention in AdOM and discuss the surgical outcomes of the tailored surgical intervention approach we have implemented in clinical practice.
Characteristics of AdOM and Main Factors Determining Treatment
Our clinical experience demonstrated that symptoms of AdOM differ by disease severity, and there is no obvious correlation with the extent adhesion of TM. The most frequently reported symptoms include ear tightness and tinnitus, with the absence of vertigo or facial paralysis. In the later stages of Sade grade (particularly grades III-V), patients with AdOM show an increased incidence of granulation tissue, cholesterol granulomas, and cholesteatoma within the tympanic cavity. Intraoperation findings revealed that the extent of ossicular chain injury increased as AdOM worsened, increasing the need for ossicle implantation.
Various methods have been used to treat AdOM and reduce the risk of re-adhesion. These include cartilage tympanoplasty with a transtympanic ventilation tube,3,8 transplantation of nasal mucosal epithelial cell sheets into the middle ear cavity, 9 application of anti-adhesion materials, 10 and tympanoplasty with placement of a silicone insulator in the drum chamber.
We hypothesize that the different forms of AdOM should be treated using different methods. Watchful waiting is appropriate for patients with grade I AdOM who are asymptomatic, have normal hearing, and are stable, consistent with the literature. 3 If ear tightness or hearing loss develops, surgery is required. In our hospital, most grade I AdOM patients are treated in the outpatient department. Our choice of surgical method for patients with AdOM grades II to IV is based on PTA, preoperative imaging results, and tympanic cavity lesion status, which includes tympanotomy tube insertion, tympanoplasty, or both, which are detailed in Figure 5. Our comparative analysis of pre- versus postoperative audiometric data demonstrated significant improvement in speech-frequency hearing (0.25-2 kHz), with both AC thresholds and ABGs showing clinically meaningful gains. These improvements were particularly pronounced in patients with advanced AdOM (Sade grade IV), whose median ABG improved from a preoperative value of 28.00 (20.50-38.00) dB to a postoperative value of 21.25 (13.12-26.88) dB. This finding is consistent with outcomes reported in recent literature. For instance, a study on endoscopic management of cholesteatoma observed a mean ABG reduction, with preoperative and postoperative ABG-PTA values of 26.17 ± 12.20 and 18.88 ± 12.11 dB, respectively. 11 The observed hearing recovery provides preliminary support for the effectiveness of our individualized treatment strategy in this challenging patient subgroup. However, further validation through larger, randomized clinical trials is warranted to confirm these findings and establish broader generalizability.
The success of ear surgery is largely dependent on good Eustachian tube function and aeration of the middle ear,3,7,12 which enhance the air content of the tympanic cavity, thus helping recovery from AdOM and improving hearing.13,14 A conventional surgical method has been used to remove lesions from grade I patients, with the placement of a silicone or cartilage film in the tympanum to prevent adhesion. Six months later, stage II surgery was performed for hearing reconstruction. However, hearing recovery remained poor in most patients 15 because long-term stability of the tympanic air chamber was not achieved. For patients with identified Eustachian tube dysfunction during surgery, we performed concurrent tympanostomy tube placement with tympanoplasty to potentially enhance hearing recovery and achieve dry ear status. Postoperative tympanic cavity aeration was assessed via CT imaging at 6 month follow-up. Thirteen patients (16.1%) underwent repeat CT, and the air levels of the tympanum were good in 8 patients (61.5%). However, due to the relatively small cohort receiving this combined procedure in our study, we cannot yet draw conclusions with high clinical evidence level.
Despite these efforts, some patients experienced residual symptoms. In our cohort, residual ear tightness was reported in 11.1% (9/81) of ears, which may result from inadequate postoperative middle ear aeration and Eustachian tube dysfunction. Tinnitus persisted in 12.3% (10/81) of ears, which may be attributed partly to pre-existing tinnitus, and could also be associated with cochlear changes from acoustic energy during drilling or ossicular manipulation, as well as residual conductive hearing loss that alters auditory processing. To better understand the persistence of these symptoms and their underlying mechanisms, longer-term postoperative follow-up and more detailed monitoring of Eustachian tube function may be necessary.
Advantages of Endoscopic Ear Surgery in Managing AdOM
Modern ear microsurgery seeks to remove lesions and restore function with minimal trauma. 16 While the traditional microscopic approach offers high magnification, its field of view is relatively narrow. Extensive removal of bone from the posterior and superior walls of the external auditory canal is often necessary to fully expose and access lesions located in the posterior tympanic chamber and facial recess, a process that may increase the risk of facial nerve injury. Since most TM adhesions in AdOM are situated in the posterior tympanum, adequate visualization is critical. Ear endoscopes provide a wide-angle view that facilitates clear visualization of middle ear structures, including the posterior tympanic chamber and facial recess, with minimal bone removal. 17 In our experience, endoscopic surgery was associated with shorter hospital stays compared to microscopic tympanoplasty in AdOM patients, suggesting potential benefits in cost-efficiency.18 -20 However, further long-term clinical observations are required to substantiate these outcomes and more comprehensively evaluate the functional advantages of the endoscopic technique.
Conclusions
Individualized oto-endoscopic surgery, particularly tympanoplasty (with or without tympanotomy tube insertion), significantly improves hearing outcomes in advanced AdOM (Sade grades III-V), as evidenced by reduced ABG and high TM healing rate. Patients with varying degrees of AdOM require customized treatment approaches.
Limitations
While our study provides valuable insights, several limitations should be noted. The relatively small sample size and short follow-up period may restrict the statistical power and long-term assessment of outcomes. The single-surgeon and single-center design may introduce operator-specific bias, limiting the reproducibility and generalizability of our results. The lack of a control group prevents direct comparisons with non-surgical management approaches and other treatments. Although our data are encouraging, more rigorous studies – particularly randomized double-blind cohort studies with longer-term observational results – are required to establish evidence-based conclusions regarding the postoperative prognosis of AdOM.
Supplemental Material
sj-docx-1-ear-10.1177_01455613251390063 – Supplemental material for Individualized Endoscopic Surgical Treatment According to the Extent of Adhesive Otitis Media
Supplemental material, sj-docx-1-ear-10.1177_01455613251390063 for Individualized Endoscopic Surgical Treatment According to the Extent of Adhesive Otitis Media by Jingfang Wu, Xiaoling Lu, Yimeng Li, Haojie Sun, Weiming Hao, Lei Ye, Yibo Huang, Huiqian Yu and Dongdong Ren in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We gratefully acknowledge the personnel involved in the diagnosis and treatment of the surgery and ward, including nurses, anesthesiologists, and resident physicians.
Author Contributions
All authors made substantive intellectual contributions to this study. Dongdong Ren, Huiqian Yu, Yibo Huang, and Jingfang Wu conceptualized this work. Dongdong Ren and Jingfang Wu were responsible for the diagnosis, surgery, and follow-up assessment. Xiaoling Lu, Yimeng Li, and Lei Ye collected the data. Xiaoling Lu, Yimeng Li, Haojie Sun, Weiming Hao, and Lei Ye contributed to data collection, obtained ethical approval for the study, and performed statistical analysis. Xiaoling Lu, Lei Ye, Dongdong Ren, and Jingfang Wu drafted the manuscript. All authors participated in the review of the manuscript and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Medical innovation research project of Shanghai 2022 “Science and Technology Innovation Action Plan” (grant number: 22Y11901900 to Jingfang Wu), the National Natural Science Foundation of China (NSFC; grant numbers: 82271166, 81970880, and 81771017 to Dongdong Ren), Natural Science Foundation of Shanghai (grant number: 22ZR1410100 to Dongdong Ren), the Health Industry Clinical Research Project of Shanghai Municipal Health Commission (grant number: 20224Y0319 to Xiaoling Lu).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated and analyzed during the current study will be made available upon reasonable request after the manuscript is accepted for publication. Researchers can contact the corresponding author at
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.