
Abstract
Introduction
Meniere disease is a condition involving recurrent episodes of vertigo, low to medium frequency sensorineural hearing loss, tinnitus, and sensations of aural fullness.1-3 First described in the late 1800s, Meniere disease was historically defined by its clinical profile. The American Academy of Otolaryngology—Head and Neck Surgery Committee on hearing and equilibrium has published clinical guidelines for diagnosis of Meniere disease. The histopathology of Meniere disease was first outlined in 1938.4,5 In 1960, Lindsay published clear histopathological images of “hydrops of the labyrinth” from human temporal bone sections and correlated his findings to clinical data and audiograms. 6 This was the morphologic demonstration of distension of the endolymphatic spaces of the membranous labyrinth and the correlation of that distortion with Meniere disease symptoms, particularly hearing loss.
The classic histopathologic finding of endolymphatic dilation has been accepted as pathognomonic of Meniere disease for almost a hundred years. However, these have all been in postmortem specimens. We present here the first pairing of Meniere specimens with dilation of the endolymphatic spaces as seen on magnetic resonance imaging (MRI) in living patients.
Materials and Methods
The Institutional Review Board/Office for the Protection of Research Subjects has issued a grant of exemption from IRB review: Waiver for study 2023-1201 of HIPAA Authorization for use of Protected Health Information or research purposes.
Temporal Bone Histopathologic Images
Patient 1—The histopathologic images of Meniere disease distortion of the endolymphatic space were taken from a 76-year-old female who died in 1969 (Figure 1a and b). Symptomatology, audiometric studies, and improvement after endolymphatic sac operation confirmed Meniere disease of the right ear (audiogram of affected right ear—Figure 2).
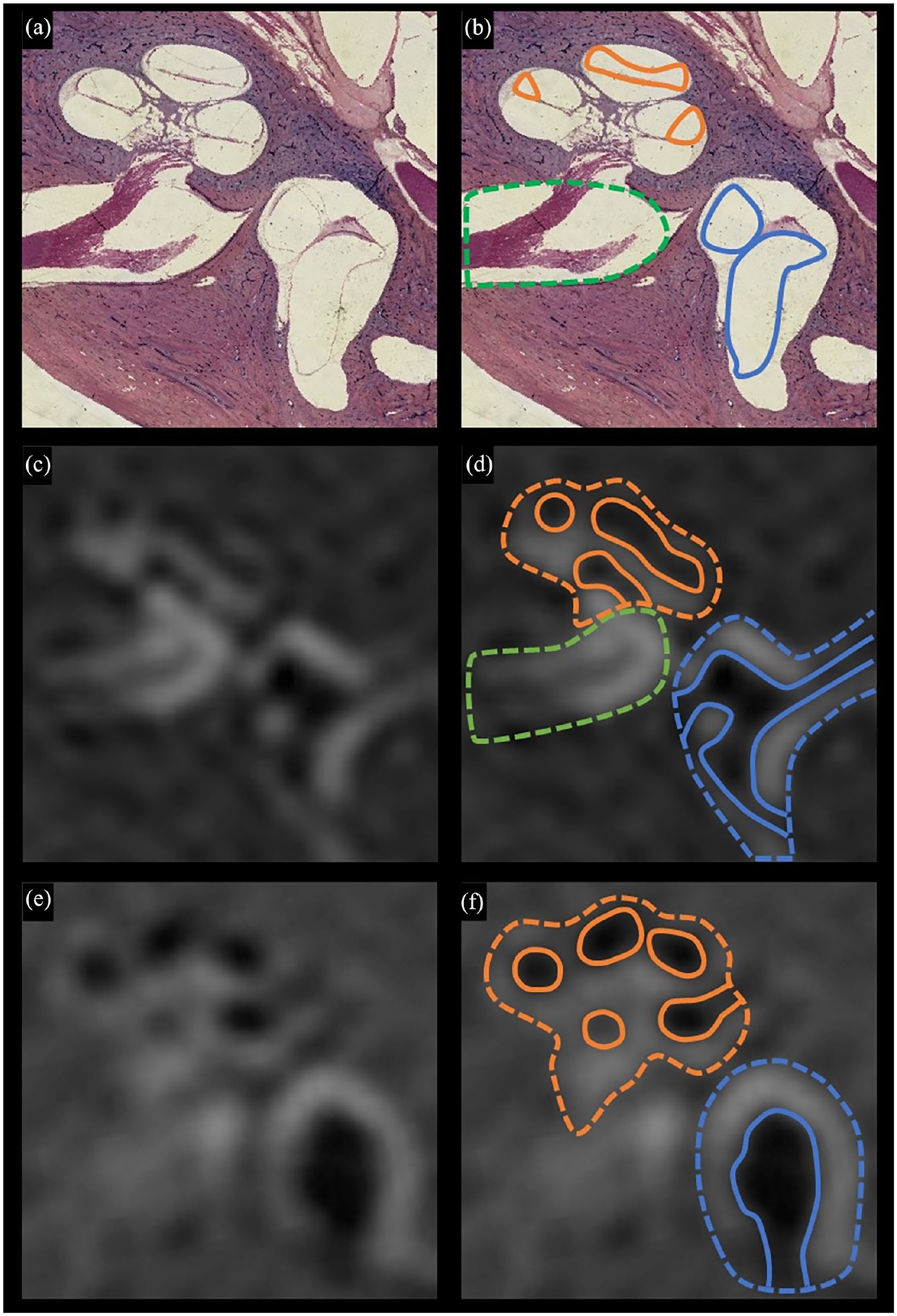
Postmortem patient 1—Meniere disease histopathology and living patients 3 and 4—affected ears—MRI (histopathologic images of the affected ear reversed left/right for illustrative purposes). (a) Postmortem patient 1—histopathologic image of Meniere disease’s distortion of the endolymphatic space. (b) Postmortem patient 1—histopathologic image with outlined scala media (solid orange), saccule-utricle complex (solid blue), and internal auditory canal (dotted green). (c) Living patient 3 affected ear—4 hour delayed REAL IR MRI of the affected ear with Meniere disease symptoms and audiometry. (d) Living patient 3 affected ear—4 hour delayed REAL IR MRI with diagrammed cochlea (dotted orange), vestibule (dotted blue), and internal auditory canal (dotted green), with distention of the scala media (solid orange), and distention of the saccule-utricle complex (solid blue). (e) Living patient 4—4 hour delayed REAL IR MRI showing the distended endolymphatic spaces in one cross-sectional image. (f) Same REAL IR MRI with diagrammed cochlea (dotted orange), vestibule (dotted blue), and internal auditory canal (dotted green), with distention of the scala media (solid orange), and distention of the saccule-utricle complex (solid blue). MRI, magnetic resonance imaging; IR, inversion recovery.
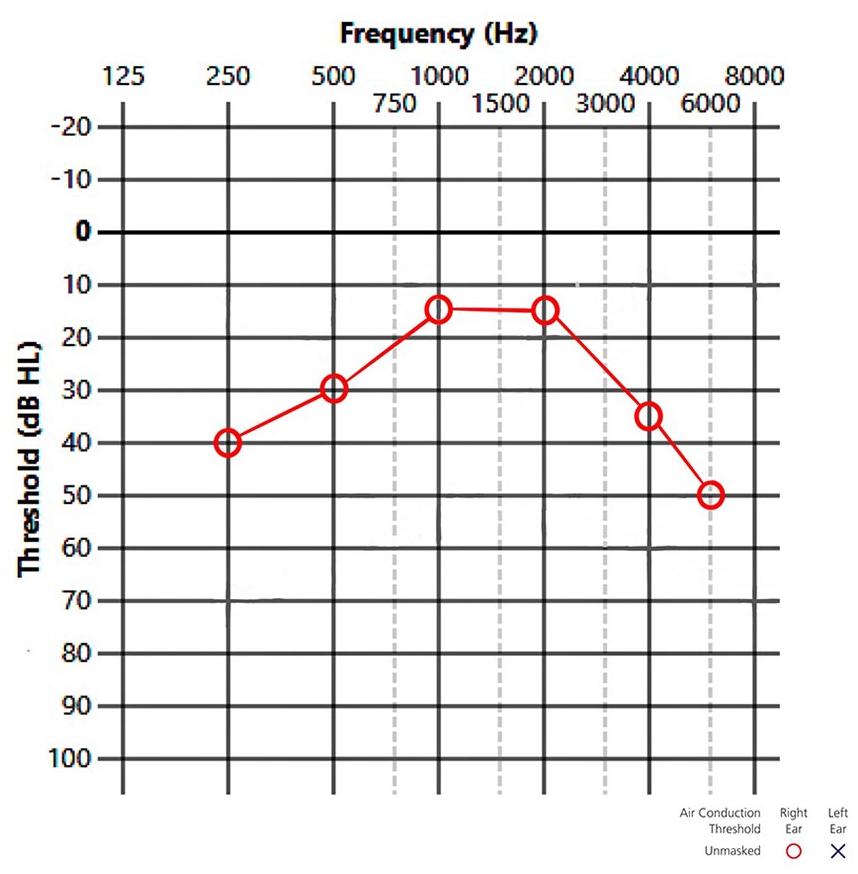
Audiogram of patient 1 right ear. This patient had classic episodic vertigo with fluctuating right upsloping sensorineural hearing loss and some relief from an endolymphatic sac operation. Shown are the right pure-tone thresholds in established pure sensorineural hearing loss.
Patient 2—The histopathologic images of a normal (non-Meniere disease) membranous labyrinth, without distortion of the endolymphatic space, were taken from a female who died of osteogenic sarcoma in 1955 (Figure 3a and b).
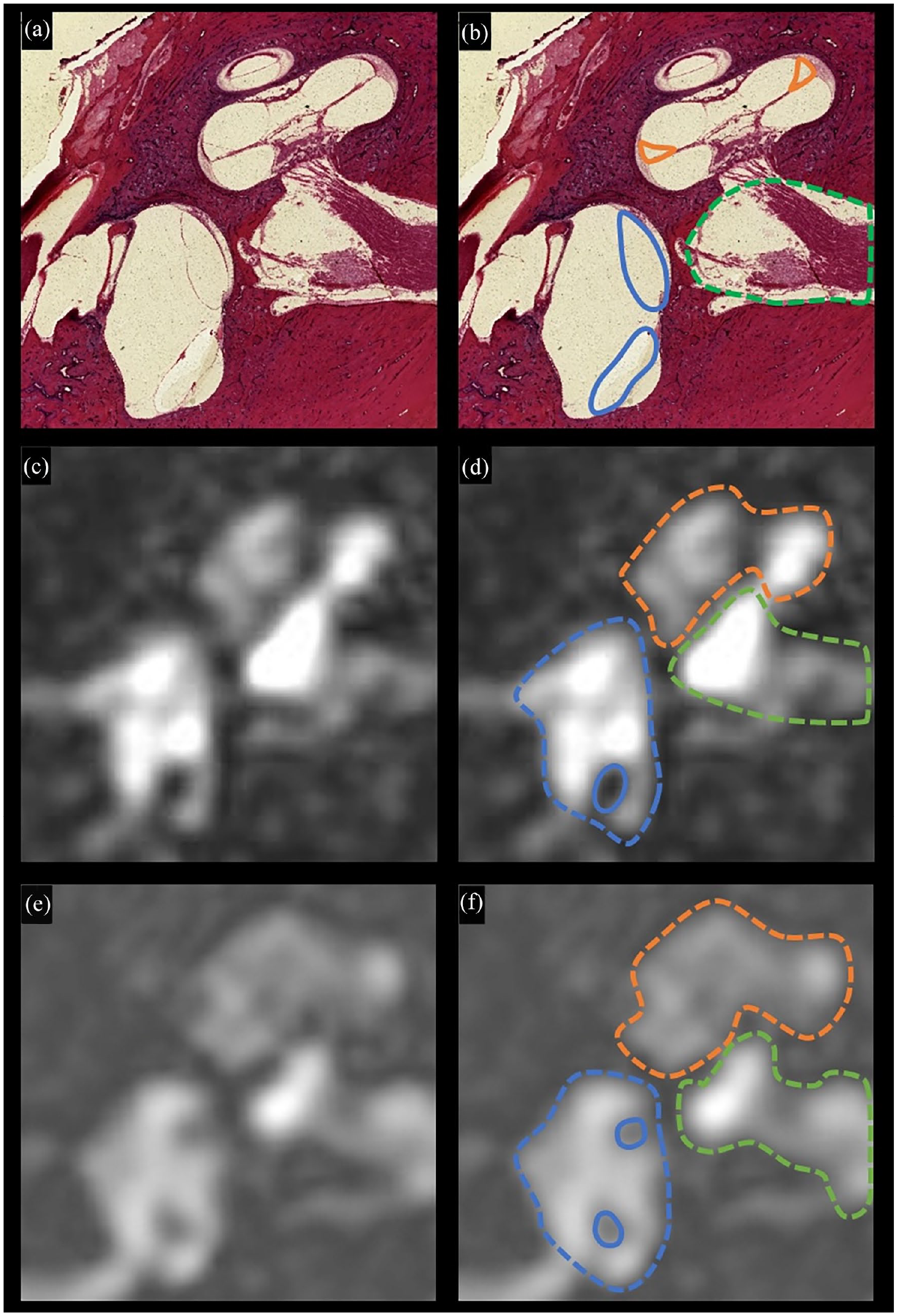
Postmortem patient 2—non-Meniere disease histopathology and living patients 3 and 5 unaffected ears—MRI. (a) Postmortem patient 2—histopathologic image of non-Meniere disease without distortion of endolymphatic space. (b) Postmortem patient 2—histopathologic image with outlined scala media (solid orange), saccule-utricle complex (solid blue), and internal auditory canal (dotted green). (c) Living patient 3 unaffected ear—4 hour delayed FLAIR SPACE MRI of unaffected ear with non-Meniere disease symptoms and audiometry. (d) Living patient 3 unaffected ear—4 hour delayed FLAIR SPACE MRI with diagrammed cochlea (dotted orange), vestibule (dotted blue), and internal auditory canal (dotted green), with nondistention of the saccule-utricle complex. (e) Living patient 5 unaffected ear—4 hour delayed FLAIR SPACE MRI showing the nondistended endolymphatic spaces in one cross-sectional image. (f) Living patient 5 unaffected ear—4 hour delayed FLAIR SPACE MRI with diagrammed cochlea (dotted orange), vestibule (dotted blue), and internal auditory canal (dotted green), with nondistended scalae and saccule-utricle complex. MRI, magnetic resonance imaging; FLAIR, fluid-attenuated-inversion-recovery; SPACE, Sampling Perfection with Application optimized Contrast using different flip angle Evolution.
After these subjects’ temporal bones were removed in postmortem, they were processed by the traditional methods as outlined by Nadol 7 and Linthicum et al. 8 The temporal bones were initially immersed in 10% buffered formalin for 1 month. Subsequently, they underwent decalcification with ethylenediaminetetraacetic acid for multiple months until all calcium was removed. Following decalcification, the specimens were subjected to a dehydration process using a series of alcohol concentrations (80%, 95%, 100%). They were then embedded in celloidin, progressing through concentrations of 2%, 4%, 6%, and 12%. The celloidin blocks were clarified with cedar wood oil and then cut into 20 micron sections, which were attached to numbered tissue squares. One out of every 10 sections were stained using hematoxylin and eosin and placed on 1 inch by 3 inch glass slides.
Four-Hour-Delayed Gadolinium 3D REAL IR and SPACE FLAIR MRI
Patient 3—The MRI of the affected ear (Figure 1c and d) and the nonaffected ear (Figure 3c and d) were taken from a 46-year-old forklift driver who has episodes of unilateral hearing loss and tinnitus and spinning. Audiogram shows the affected and the nonaffected ears in this patient (Figure 4).
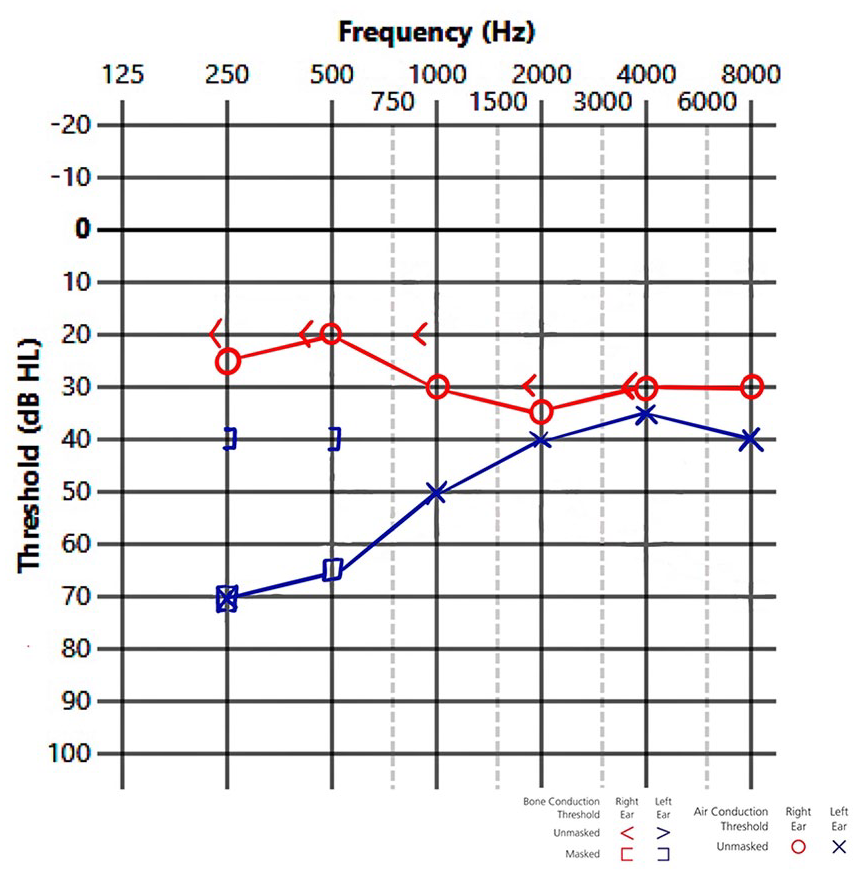
Audiogram of living patient 3 showing the affected and unaffected ears.
Patients 4 and 5. The MRI of the affected ear (Figure 1e and f) of living patient 4 and the nonaffected ear of living patient 5 (Figure 3e and f) are displayed.
The MRI examinations were performed on a 3 T Siemens Vida with a 64-element head coil. All patients underwent MRI 4 hours after injection of a single dose of gadolinium (1.0 mmol/mL at a dose of 0.1 mmol/kg). The imaging sequences were turbo-spin-echo 3D REAL inversion-recovery (3D REAL IR) and Sampling Perfection with Application optimized Contrast using different flip angle Evolution (SPACE) fluid-attenuated-inversion-recovery (FLAIR) sequences.
The 3D-REAL IR sequence was acquired with an axial orientation and features a slice thickness of 0.8 mm, with 36 slices. The repetition time was 16,000 ms, the echo time was 551 ms, and the inversion time was 2700 ms. The sequence had an average of 1.6 and a flip angle of 120°. The voxel size was 0.3 × 0.3 × 0.8 mm³, and the field of view was 160 mm × 160 mm. The entire acquisition took 9 minutes and 20 seconds.
The 3D FLAIR sequence was conducted with a field of view of 190 mm, a section thickness of 0.8 mm, a repetition time of 6000 ms, and an echo time of 168 ms. The number of excitations was set to 1, with an inversion time of 2000 ms and a flip angle of 180°. The matrix size was 384 × 384, and the bandwidth was 186 Hz per pixel. The turbo factor was 27, and the voxel size was 0.5 mm × 0.5 mm × 0.8 mm. The total scan time was 14 minutes.
These sequences, performed 4 hours after gadolinium injection, captured gadolinium sequestered and concentrated in the perilymphatic spaces while being absent from the distended endolymphatic spaces.
Results—Paired Imaging Modalities
The histologic images from the postmortem examination of Meniere disease patient 1 reveal a distinct dilated morphology of the membranous labyrinth, as depicted in Figure 1a and b. Specifically, the saccule, utricle, and scala media are each notably distended, indicative of the pathological changes associated with Meniere disease. This histologic evidence aligns with imaging findings in our living patient: In patient 3, who suffers from unilateral Meniere disease, a 4 hour delayed MRI scan of the labyrinth demonstrates similar distention of the saccule, utricle, and scala media on the affected side (Figure 1c and d). These MRI results corroborate the postmortem findings, suggesting a consistent pattern of endolymphatic hydrops across different diagnostic modalities and patient conditions.
To further illustrate this correlation, we have paired the histologic evidence of endolymphatic distension from patient 1 with a corresponding 4 hour delayed MRI from patient 4. This MRI shows the classic distention of the scala media and utriculosaccular space in a single cross-sectional view (Figure 1e and f). This side-by-side comparison underscores the reliability of MRI in detecting endolymphatic hydrops in living patients, mirroring the pathological changes observed postmortem.
In contrast, the postmortem histopathology of patient 2, who did not have Meniere disease, shows normal morphology of the saccule, utricle, and scala media (Figure 3a and b). This normal histological presentation serves as a control, highlighting the absence of dilation and providing a baseline for comparison. Consistently, the 4 hour delayed MRI of a living patient 3 on the unaffected side shows no dilation of the membranous labyrinth, reinforcing the specificity of the findings associated with Meniere disease (Figure 3c and d).
In addition, we have paired the normal histology from patient 2 with a superior 4 hour delayed MRI from patient 5, who presents with a normal utriculosaccular space (Figure 3e and f). This pairing further demonstrates the diagnostic capability of delayed MRI in differentiating between normal and pathological states of the membranous labyrinth, enhancing our understanding of Meniere disease and its radiological features.
Discussion
This original article demonstrates how the 4 hour delayed MRI in living patients suspected of Meniere disease recapitulate postmortem histopathology which has been attributed to Meniere disease. The aim is to provide a dynamic context for the histopathological findings which as we know can be delayed for decades from the onset of disease. Such a correlation provides 2 new pieces of information. First, the visible dilation of the endolymphatic space in a living person confirms the postmortem histopathological morphology of Meniere disease. The membranous labyrinth is in fact dilated during active Meniere disease in a living person.
The second piece of information is that an accessible real-time investigation can be performed on a living patient to establish the diagnosis of Meniere disease. The ability to get a confirmatory MRI will prove especially useful in patients suspected of Meniere disease but whose symptoms are not classic.
Histologic confirmation of Meniere disease has historically been delayed until postmortem examination. Furthermore, current real-time diagnostic techniques are limited in their utility. The summating potential/action potential (SP/AP) ratio on electrocochleography measurements can involve cumbersome scheduling logistics. Most important, the SP/AP ratio was found to have low sensitivity, low specificity, and poor correlation with severity. 9 As a result, recent guidelines regarding Meniere disease have continued to rely on symptomatic presentation and exclusion of other vestibular causes. The gold standard thus remains a combination of clinical symptoms with an upsloping low-frequency sensorineural hearing loss.
Recently, advances in MRI sequences have paved the way for visualization of endolymphatic hydrops in living patients.10-14 These techniques utilize IR, in which signals from specific tissues are suppressed to maximize contrast between regions of interest. FLAIR is one such sequence that specifically suppresses signals from fluids. In combination with a gadolinium contrast agent that does not diffuse into the membranous labyrinth, this produces a high contrast between the gadolinium-enhanced perilymph and the endolymph and has allowed for identification of hydrops by radiologists with high sensitivity and specificity. It has been found that 3T MRI with intravenous gadolinium injection is a credible method for establishing endolymphatic hydrops in patients with Meniere disease.15,16
The limitations of this study are that atypical Meniere disease is not explored here. We have not presented patients with isolated cochlear or vestibular Meniere disease. Nor were 4 hour delayed MRIs performed on patients who had no symptoms of Meniere disease in either ear. Our nonaffected samples were from the unaffected ears of unilateral Meniere disease patients. However, Fujita et al concluded in their study that MRI for atypical Meniere disease has become a useful tool to look for endolymphatic hydrops and can be used for patients with ambiguous clinical pathology. 16
The major strength of this study is the support it gives to the classic histopathologic description of Meniere disease. The best evidence would be MRI and histopathological images from the same individual, but logistically this combination would be very difficult to attain. Instead, the correlation reported here provides very strong circumstantial evidence that the histopathological findings are valid. It brings the dilation of the endolymphatic space back full circle to original postmortem descriptions. In addition, the authors hope that this study, in the otolaryngologic literature, will encourage otologists to use this 4 hour delayed MRI modality to help identify Meniere disease patients. The authors also hope that this study will remind the otologic public of the continued significance of the priceless and irreplaceable temporal bone collections across the world. We very much want to raise public awareness that these collections are valuable and should be curated.
Temporal bone histopathology has clarified the pathophysiology of otologic disease in the United States for more than 100 years. 17 Temporal bone otopathology laboratories, once a standard for academic otolaryngology practice, have now become less prominent across universities worldwide. 18 However, this study’s immediate goal is to show how the fundamentals from these early histopathologic studies continue to inform our understanding today. This study’s overall aim is to raise public awareness that these neglected collections are valuable and should be curated. This article demonstrates the correlation of traditional histopathologic findings with the MRI-demonstrated distention of the endolymphatic spaces. As temporal bone histopathologists, we take particular satisfaction in seeing the real-time mirroring and confirmation of the postmortem histopathologic findings.
Footnotes
Data Availability Statement
The authors confirm that the de-identified data supporting the findings of this study are available within the article. Due to the nature of the study, which involves patient health records, the data cannot be made publicly available to maintain patient confidentiality and privacy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The Institutional Review Board/Office for the Protection of Research Subjects (IRB/OPRS) has issued a grant of exemption from IRB review: Waiver for study 2023-1201 of HIPAA Authorization for use of Protected Health Information (PHI) for research purposes [45 CFR 164.512(i)(1)(i)].