
Abstract
External stapediovestibular dislocations are rare and often traumatic. Congenital facial nerve anomalies, as in this case, make reconstruction of the ossicular chain even more challenging.
A 37-year-old woman patient presented progressive bilateral hearing loss and aural fullness for 1 month in May 2024. She had suffered a fall from a height of approximately 4 stories in 2017. The audiometry showed bilateral conductive hearing loss with an air-bone gap greater than 50 dB. A temporal bone computed tomography scan showed suspected stapes detachment and facial nerve anomalies in both ears. Right exploratory tympanotomy revealed external stapediovestibular dislocation with duplication of facial nerve in the tympanic segment. A type V tympanoplasty with piston wire insertion was performed. Audiometry after right ear surgery showed closure of the air-bone gap by 42 dB, without vertigo or facial nerve injury.
Surgery aims to prevent facial nerve injury while successful restoring hearing loss. The cause of stapediovestibular dislocation is discussed, along with methods for reconstruction of the ossicular chain.
Introduction
External stapediovestibular dislocation is a rare condition, typically resulting from traumatic injury to middle ear structures. 1 Dislocations can be classified as internal (with the stapes depressed into the vestibule) or external (where the stapes is dislocated and hanging in the tympanic cavity). The resulting hearing loss can be purely conductive if the ossicular chain is disrupted, or mixed if a perilymphatic fistula (PLF) occurs. In such cases, cochleovestibular symptoms, including tinnitus and vestibular dysfunction, may also be present.
Case Report
A 37-year-old female had a history of anxiety and major depressive disorder. She sustained a fall from a height of approximately 4 stories in 2017, resulting in multiple injuries, including head injury. A facial bone computed tomography (CT) scan was performed to evaluate the trauma, revealing pneumocephalus in the bilateral temporal region and a fracture line over the anterior wall of the left middle ear. No remarkable fractures were observed on the right side.
She visited our ENT outpatient department (OPD) 1 month after the injury, noting left-sided aural fullness and hearing impairment since the trauma. Physical examination revealed left middle ear effusion. Audiometric testing showed a 4-frequency pure-tone average of 79 dB Hearing Level (HL), with an air-bone conduction gap (ABG) of 54 dB on the right side and an average of 54 dB HL with an ABG of 33 dB on the left side (Figure 1). Thereafter, she was lost to follow-up.
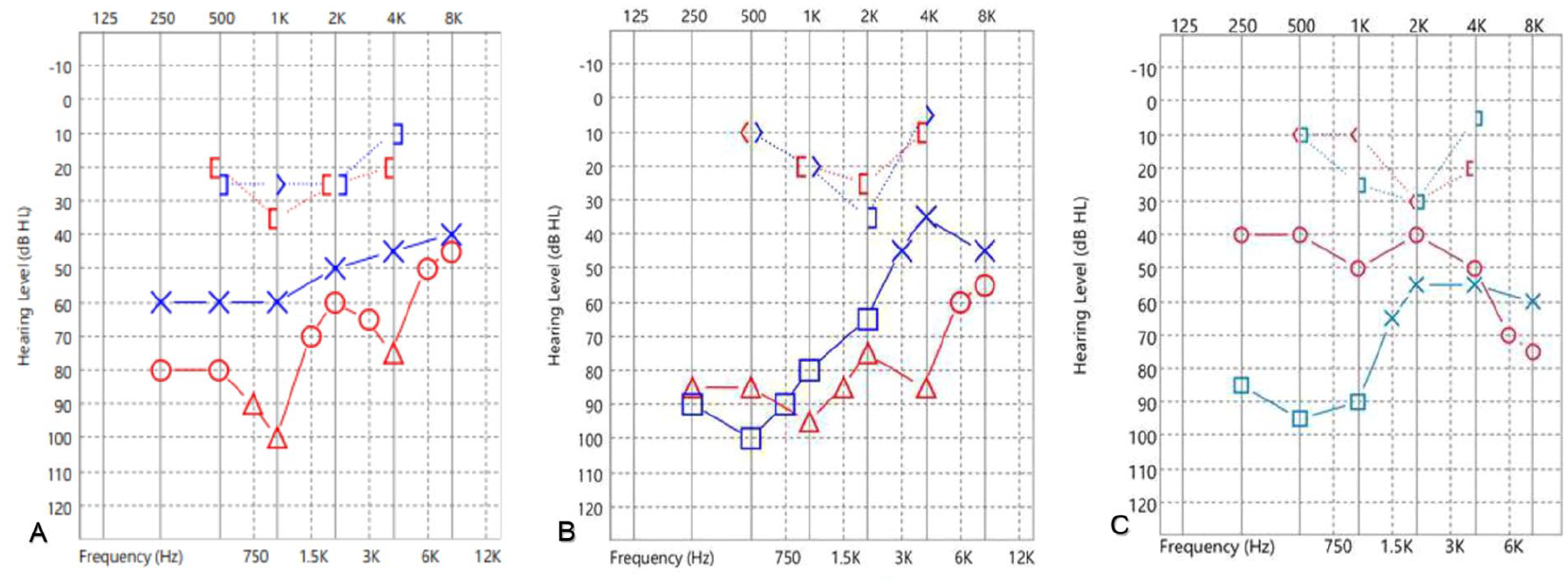
Preoperative and postoperative audiograms of the patient. (A) Audiogram on February 15, 2017, following the fall, showing right-sided conductive hearing loss with 4-frequency pure-tone average of 79 dB Hearing Level (HL) with an air-bone gap of 54 dB HL. (B) Preoperative audiogram on May 6, 2024, showing right-sided conductive hearing loss with an average of 85 dB HL with an air-bone gap of 69 dB HL. (C) Postoperative pure tone audiogram on July 23, 2024, showing right-sided improved hearing with average of 45 dB HL with an air-bone gap of 27 dB HL.
In May 2024, she returned to our ENT OPD, complaining of progressive bilateral hearing loss and aural fullness for the past month. No otorrhea, otalgia, or fever were reported. Speech or language impairments were not observed. She did not mention any previous fall history. Physical examination revealed bilateral grade 1 microtia (Figure 2). Her external ear canals and tympanic membranes were relatively normal.

Right ear grade 1 microtia of the patient.
A 4-frequency pure-tone audiometry (PTA) revealed an average HL of 85 dB with an ABG of 69 dB on the right side, and an average HL of 70 dB an ABG of 52 dB on the left side, with a 2k dip. These results indicated bilateral progressive hearing loss compared to those in 2017, both in terms of average threshold and air-bone gap (Figure 1).
Temporal bone CT showed a suspected right facial nerve duplication at the tympanic segment, with one segment at the normal facial canal and another below the oval window. The stapes was lateralized to the oval window (Figure 3). On the left side, the tympanic segment of the facial nerve was aberrant, positioned below the oval window. The stapes was detached from the oval window, lateralized, and suspected to adhere to the facial nerve (Figure 3).
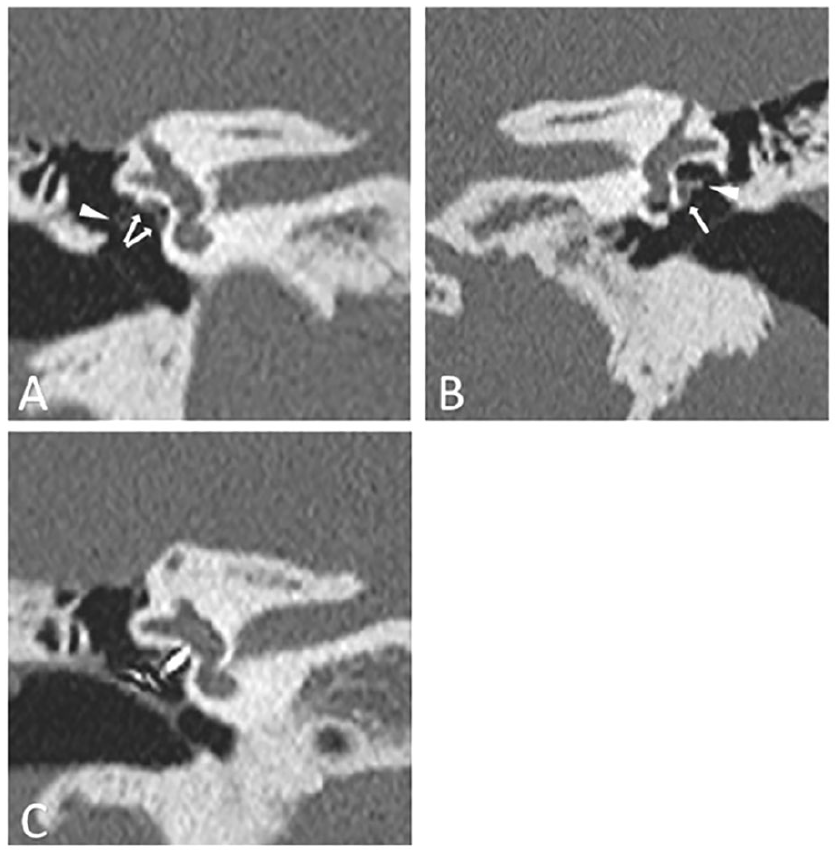
Preoperative and postoperative temporal bone High-Resolution Computed Tomography (HRCT) of the patient. (A) Preoperative temporal bone HRCT showing right facial nerve duplication at the tympanic segment (white arrows). The stapes was lateralized to the oval window (white arrowhead). (B) Preoperative temporal bone HRCT showing aberrant left facial nerve in the tympanic segment, positioned below the oval window (white arrow). The stapes was suspected to be adherent to the facial nerve (white arrowhead). (C) Postoperative temporal bone HRCT of right ear showing the piston wire well-seated between the 2 duplicated facial nerves.
With a diagnosis of bilateral stapes detachment, the patient opted to undergo right-sided exploratory tympanotomy first.
During the right exploratory tympanotomy via the postauricular approach, the malleus and incus were abnormally orientated. External stapediovestibular dislocation was found. The 3 ossicles remained connected, yet the stapes was dislocated and floating, with its suprastructure intact. The presumed footplate and oval window were not in the expected position between the bifurcated tympanic segment of the facial nerve (Figure 4). Both bifurcated facial canals were dehiscent.
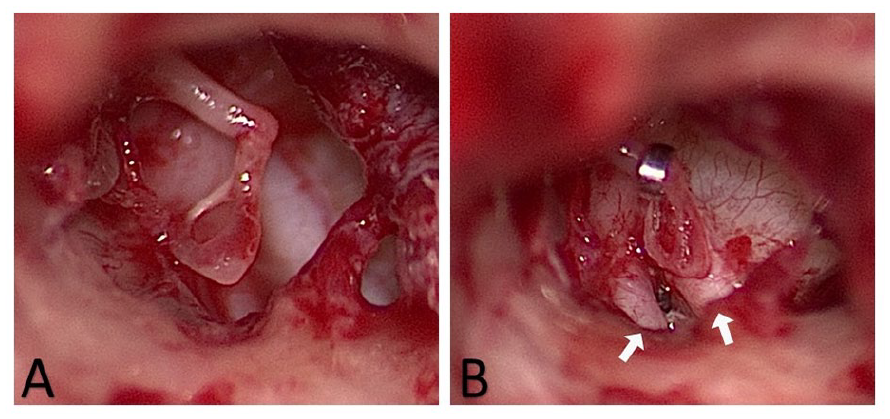
Intraoperative findings. (A) The stapes was dislocated and floating. (B) Piston wire was inserted into the vestibular fenestration between the bifurcated facial nerves (white arrows) and fixed to the long process of the incus.
To repair the stapediovestibular dislocation, vestibular fenestration was performed between the facial nerve duplications using a manual perforator instead of a powered drill or laser to avoid injury to the facial nerve because the distance between the duplicated facial nerves was very narrow. A piston wire was inserted into the vestibular fenestration and fixed to the long process of the incus (Figure 4). The fenestra were sealed with a muscle graft. The stapes was left untouched, as it did not interfere with the reconstructed ossicular chain.
Two months after surgery, the postoperative PTA showed an average of 45 dB HL and an ABG of 27 dB on the right side (Figure 1). Follow-up CT revealed a well-seated right piston wire between the 2 duplicated facial nerves (Figure 3), with no vertigo reported postoperatively.
Discussion
A malpositioned facial nerve in the middle ear was further categorized by Jahrsdoerfer 2 according to its position relative to the oval window 2 :
(a) Crossing at the level of the oval window
(b) Crossing inferior to the oval window
(c) Pressing against the stapes superstructure
(d) Bifurcating to branch around the facial nerve (may or may not rejoin)
(e) Crossing the promontory vertically
(f) Suspended in mid-air.
For this case: right ear—group (d); left ear—group (b).
Tympanic segment bifurcation is the most common, 3 as seen in our case. Diagnosis is difficult, even with preoperative CT scanning by radiologists.
According to a recent retrospective study in China, 4 887 patients underwent stapes surgery, and the prevalence of facial nerve bifurcation was 1.13% (10/887 patients). All the patients had bifurcation in the tympanic segment. The detection rate of bifurcation by 2 radiologists reviewing the preoperative CT images was 0%. However, in our case, facial nerve duplication was observed preoperatively on CT. Another special finding in our case is external stapediovestibular dislocation.
Stapediovestibular dislocation is rare among all types of ossicular chain disruptions and is often a result of traumatic injury to the middle ear structures. A recent study showed that most patients experience internal dislocations (depressed into the vestibule) rather than external dislocations. 1 In our case, a fall injury seemed to be responsible for the external dislocation.
However, given the patient’s history (she has no speech problems, which are common in congenital hearing loss), imaging, and intraoperative findings, we proposed a hypothetical mechanism as follows: a subluxation of the stapes develops into spontaneous external dislocation over a period of time.
A review of her brain CT scan performed immediately after the trauma revealed no remarkable fracture line in the right temporal region. Additionally, according to the patient, her hearing loss had progressed.
Traumatic dislocation is often accompanied by a PLF that causes mixed type hearing loss. 1 However, during the surgery, no fracture line or healing tissue was observed in the temporal bone. No signs indicated previous PLF. The oval window was replaced with a dense bone plate.
As fenestration of the vestibule is an essential step in ossicular chain reconstruction, a risk of injury to the adjacent facial nerve exists. There is literature discussing the application of facial nerve monitors to avoid nerve injury in such cases. Facial nerve monitoring should be used as much as possible.
In this case, both the duplicated facial canals were dehiscent and the immediate vicinity (0.36 mm) of the bifid nerve made surgery even more challenging. To perform the fenestration, we chose a manual stapes perforator instead of a microdrill or laser to avoid facial nerve injury. The laser may cause thermal injury, and the shaft of the microdrill may contact the facial nerve and cause avulsion injury.
Conclusion
In conclusion, this case involved a spontaneous external stapediovestibular dislocation with a congenital duplicated facial nerve tympanic segment. Preoperative High-Resolution Computed Tomography (HRCT) of the temporal bone is mandatory for a correct diagnosis. Using facial nerve monitoring and manual instruments instead of powered instruments, the patient was successfully treated with surgery, which yielded a satisfactory hearing outcome without complications.
Footnotes
Acknowledgements
None.
Ethical Considerations
Our institution (Research Ethics Committee of Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation) does not require ethical approval for reporting individual cases.
Consent to Participate
Informed consent was obtained from the patient of this case report.
Consent for Publication
Written informed consent was obtained from the patient of this case report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.