
Abstract
Pleomorphic adenoma (PA) represents the most frequently occurring benign tumor within both major and minor salivary glands. However, in rare instances, nasal PA is an epithelial-derived borderline tumor, often originating from the nasal septum. Diagnosis usually relies on histopathological analysis. Under general anesthesia, these rare nasal tumors can be completely resected via endoscopic surgery. This article reports a case of PA originating from the nasal septum in a 49-year-old patient presenting with nasal congestion, along with a brief review of the current literature. The diagnostic nasal endoscopic examination showed a pink neoplastic mass in the left nasal cavity. Subsequent radiologic examination demonstrated a soft tissue mass in the anterior part of the nasal septum. After complete resection under nasal endoscopy, histopathological examination confirmed it as PA. Fortunately, no related complications occurred perioperatively and postoperatively. After surgery, performing a thorough examination with nasal endoscopy and scheduling regular follow-ups are crucial steps to prevent local recurrence.
Introduction
Pleomorphic adenoma (PA) is a borderline tumor originating from epithelial tissue, primarily occurring in the parotid and submandibular glands, with occurrences in the nasal cavity being rare. 1 When PA does occur in the nasal cavity, it is most commonly located in the nasal septum, accounting for about 80% of cases, followed by occurrences in the lateral nasal cavity. 2
Case Report
The patient, a female, 49 years old, was admitted due to nasal congestion for over 3 years with no purulent discharge or headache. She has a history of subtotal hysterectomy. The specialist examination revealed no external nasal deformity, a deviated nasal septum, poor ventilation, and turbinate hypertrophy. A pink neoplasm was observed in the left nasal cavity. In addition, there was no redness, swelling, or tenderness in the sinus areas. Computed tomography scan of nasal sinus (Figure 1) showed a lesion in the anterior part of the left nasal cavity resembling a benign tumor and inflammation of the bilateral maxillary sinuses. Nasal endoscopy (Figure 2) showed a deviated nasal septum and hypertrophy of the right inferior turbinate were observed, accompanied by mucosal congestion within the nasal cavity. In addition, a neoplasm was identified in the left nasal cavity. Most important, there were no abnormalities in the nasopharyngeal area. The patient underwent nasal endoscopic lesion excision and inferior turbinate reshaping under general anesthesia. Endoscopic examination revealed a pink, round mass in the left nasal passage that bleeds easily. On further examination, its base was identified as originating from the mucosa of the nasal septum. Subsequently, the mass was completely excised from its base, adjacent to the nasal septum, for pathological examination, utilizing electrocautery for hemostasis. Enlarged lower turbinates on the left side were fractured and displaced to clear the main nasal passage, with no active bleeding observed. The left nasal cavity was packed with a gelatin sponge for hemostasis, followed by 2 expandable sponges. The postoperative pathology report (Figure 3) indicated a salivary gland-origin tumor, specifically a PA (mixed tumor). The tumor tissue is well-demarcated from the surrounding tissue, with an intact capsule. Immunohistochemical staining results: P40 (mostly positive); P63 (mostly positive); smooth muscle actin (SMA; partially positive); CK5/6 (mostly positive); S-100 (sporadically positive); vimentin (positive); P53 (wild type); CK8/18 (sporadically positive); CK8/18 (sporadically positive).
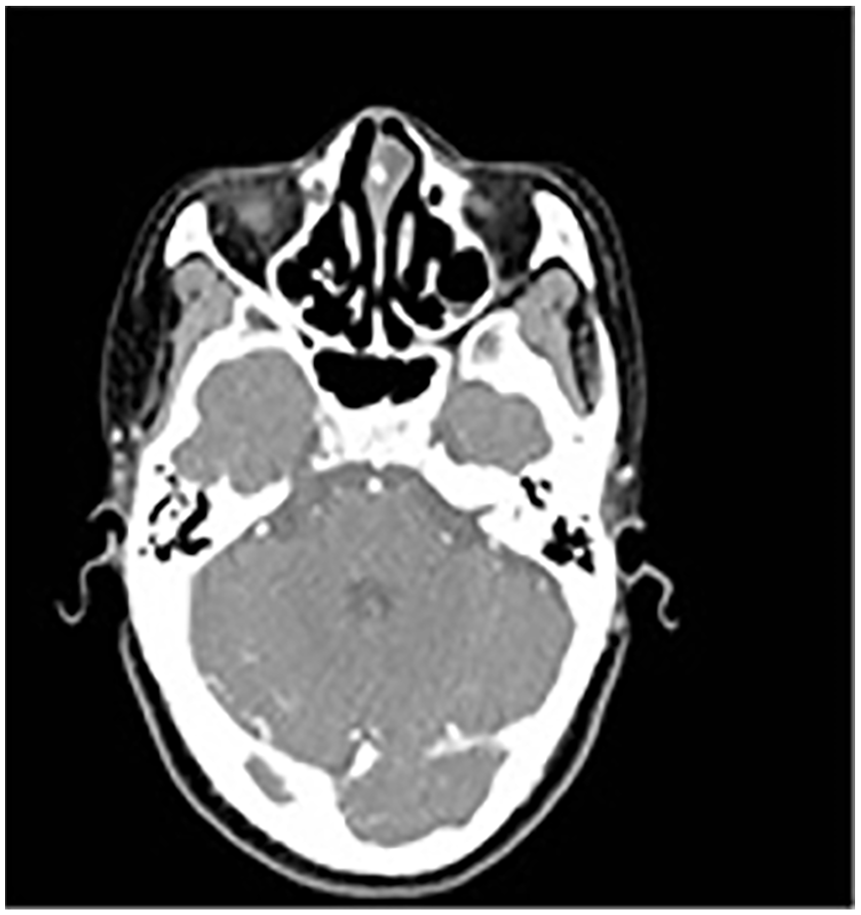
Nasal CT indicates a lesion in the anterior part of the left nasal cavity, benign tumor lesion. CT, computed tomography.
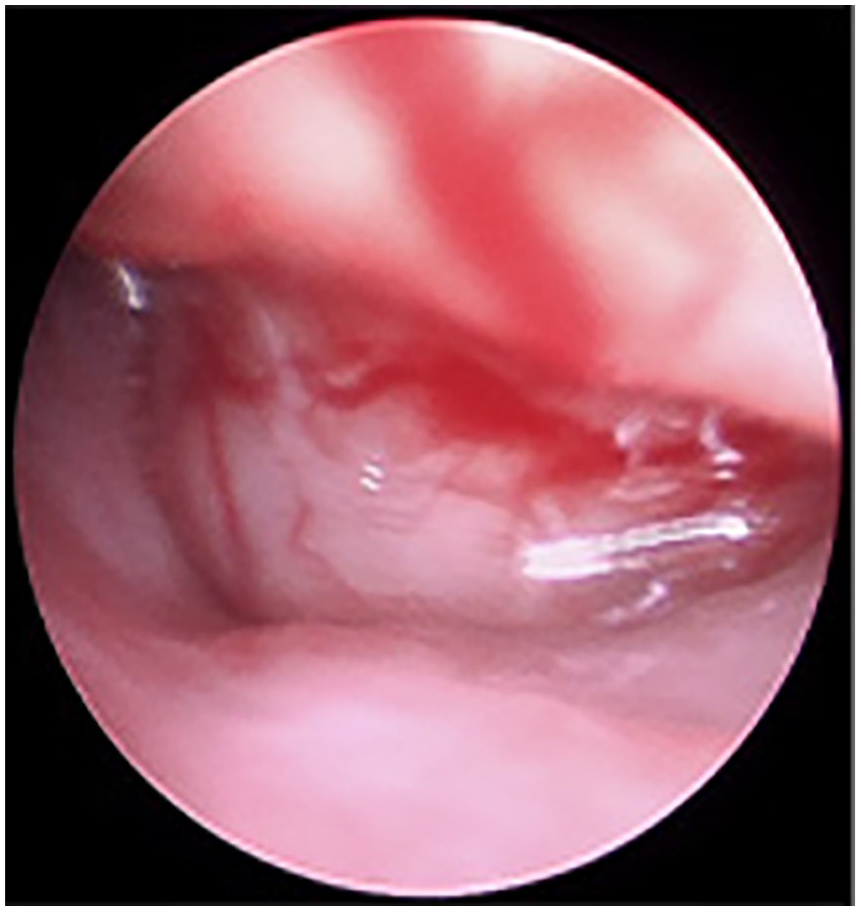
Endoscopic view indicating a neoplasm in the left nasal cavity.
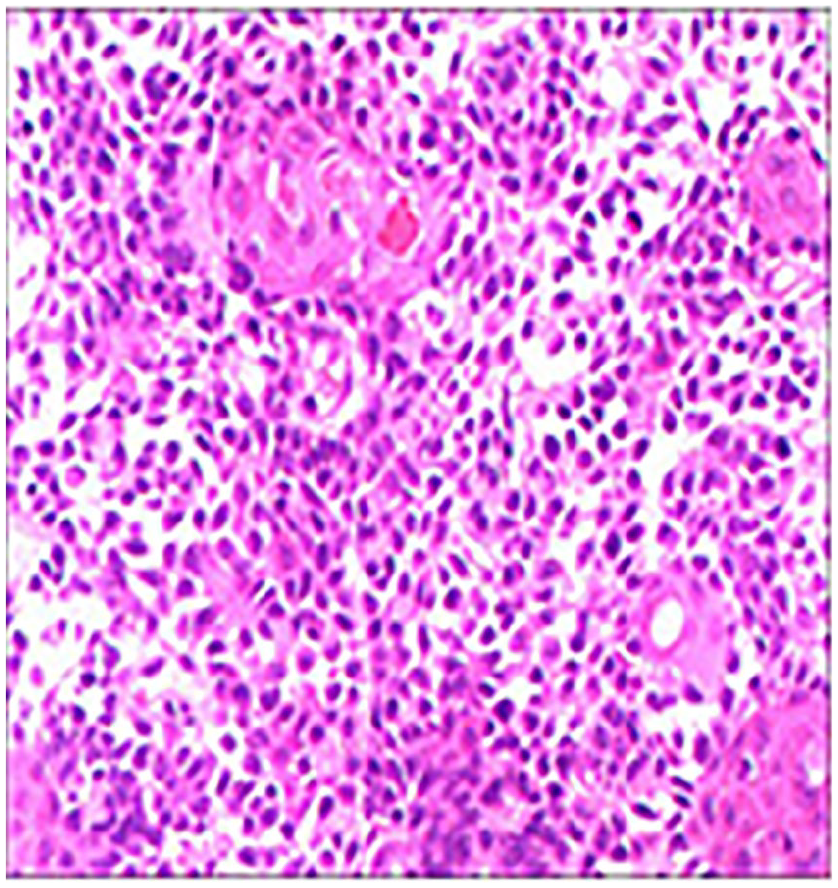
Histopathological slide (×200HE). HE, hematoxylin eosin.
Discussion
The pathogenesis of nasal PA remains unclear; however, potential viral factors have been explored. Malinvaud et al 3 reported on multiple cases of nasal septum pleomorphic adenomas, noting that all cases were positive for Epstein-Barr Virus (EBV) blood antibodies, which included one patient who was also positive for EBV-DNA.
Nasal PA typically presents as a unilateral nasal lesion, characterized by its slow expansive growth. When the lesion obstructs the nasal passage, it can manifest as progressive unilateral nasal congestion and may be accompanied by symptoms such as nasal bleeding, headache, or olfactory dysfunction. If the tumor enlarges further and grows along the nasal cavity, it often results in poor sinus drainage, sinusitis, as well as mucosal edema and polyps. 4
The diagnosis of nasal PA is primarily confirmed through histopathological examination. The histology of nasal PA is distinguished by 3 basic components: epithelial cells, myoepithelial cells, and mesenchymal/stromal. 1 Nasal PA and salivary gland PA exhibit significant histological differences; specifically, nasal PA is characterized by a higher cellular structure and epithelial component, accompanied by relatively less stromal matrix, thereby further distinguishing it from salivary PA. 5 Moreover, these tumors typically lack a capsular structure. The histological diagnosis of PA can be confirmed through the positive immunohistochemical expression of cytokeratin, vimentin, S100 protein, SMA, and glial fibrillary acidic protein. 6 Signs of malignant proliferation in PA are marked by the overexpression of p53 protein, HER-2, and the proliferation marker Ki-67 (MIB-1) at the lesion site. 5
Nasal PA is a relatively rare benign tumor that grows slowly, yet carries a certain risk of malignancy. 6 Currently, surgical removal remains the primary treatment method for nasal PA, aiming to meticulously remove the tumor tissue as thoroughly as possible while ensuring the safety of the margins. This approach aims to minimize the risk of leaving tumor residue or facilitating recurrence. 4 Endoscopic tumor removal is currently the preferred surgical method for treating nasal PA, offering several significant advantages. First, this technique enables precise determination of the tumor’s extent and location. Second, it is known to minimize the occurrence of postoperative complications. Last, it is critical in preserving the patient’s nasal form and function.7,8 For patients with suspected nasal PA, it is crucial to perform postoperative histopathological biopsy and immunohistochemical testing to confirm the diagnosis. Performing a tumor biopsy before surgery is not recommended. During surgery, preserving the integrity of the tumor capsule to the greatest extent possible is essential. If the tumor capsule accidentally leaks, it should be immediately suctioned off, and the area should be repeatedly flushed with saline to ensure the cleanliness of the surgical area. For larger nasal tumors, rhinotomy can ensure the complete removal of the tumor, thus avoiding the risk of recurrence or metastasis due to tumor residue or rupture. 4 In this case of nasal PA, we utilized endoscopic surgery, which provided a clear surgical field, allowing for the complete removal of the tumor under direct vision while preserving safe margins and ensuring that normal structures and functions were not compromised.
The primary risks associated with nasal PA include malignant transformation and local recurrence after surgical resection. Recurrence rates post surgery range from 7.5% to 8%, while the risk of malignant transformation stands at approximately 6%. 8 Notably, frequent recurrences significantly increase the risk of malignant transformation. 9 Key risk factors for recurrence are identified as a myxoid stroma, an irregular or infiltrative capsule, and multinodularity. In cases of malignant transformation, the vast majority of malignancies are squamous cell carcinoma and adenoid cystic carcinoma, along with undifferentiated carcinoma and mucoepidermoid carcinoma. 8
Conclusion
In summary, nasal PA is a clinically rare benign tumor with a potential for low-grade malignancy. Patients often present with symptoms such as unilateral progressive nasal obstruction and epistaxis. A definitive diagnosis necessitates both pathological examination and immunohistochemical analysis to identify characteristic markers. For treatment, endoscopic excision performed along the capsule ensures complete tumor removal and is the preferred method. Long-term follow-up is required due to the risk of malignant transformation.
Footnotes
Data Availability
Data are available and shared.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Fund of Health Commission of Gansu Province Outstanding Young Talent Project (GSWSQN2021-002).
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent has been obtained from the patient for the purpose of publication.