
Abstract
Septoplasty is a widely performed procedure globally to correct a deviated nasal septum and improve nasal breathing. Life-threatening nasal bleeding as a complication of septoplasty has been reported in a few cases in the literature. In cases of massive postoperative nasal bleeding, transarterial embolization using angiography was performed for the treatment. This article documents 1 case of excessive postoperative nasal bleeding following an uneventful septoplasty, which was successfully treated with embolization of the frontal branch of the middle meningeal artery. This case represents an extremely rare occurrence, and we present it in conjunction with a literature review.
Introduction
A deviated nasal septum results in obstructed nasal airflow and a sensation of nasal obstruction in the patient. Septoplasty is a surgical procedure aimed at correcting a deviated nasal septum to improve nasal airflow. Postoperative complications of septoplasty such as nasal bleeding, cerebrospinal fluid leakage, nasal septal perforation, and saddle nose deformity are known to occur. 1 One group reported a 3.3% incidence of excessive bleeding as a complication following septoplasty. 2
The middle meningeal artery (MMA) is known to arise from the internal maxillary artery, which is a branch of the external carotid artery. The MMA provides blood supply to over two-thirds of the cranial dura. 3 Therefore, otorhinolaryngologists do not commonly encounter MMA, although it may be familiar to neurosurgeons. The MMA, which is encountered during the middle fossa approach in otology, is not typically exposed in surgery within the field of rhinology.
In this case report, we describe an extremely rare occurrence of early postoperative bleeding following septoplasty, which was successfully managed through angiography and subsequent arterial embolization. The bleeding source was identified as a frontal division of the MMA. We present this extremely rare case along with a review of the literature to highlight the uncommon nature of this complication.
Case Report
A 58-year-old female presented to the outpatient clinic with worsening complaints of rhinorrhea, postnasal drip, and left-sided nasal congestion that has been ongoing for 1 year. She underwent hormone replacement therapy for 8 years after menopause and was healthy with no other significant medical conditions. Despite being on medication, she reported experiencing persistent symptoms of postnasal drip and nasal congestion. The endoscopic examination of the nasal cavity showed a leftward deviation of the nasal septum (Figure 1A and B).
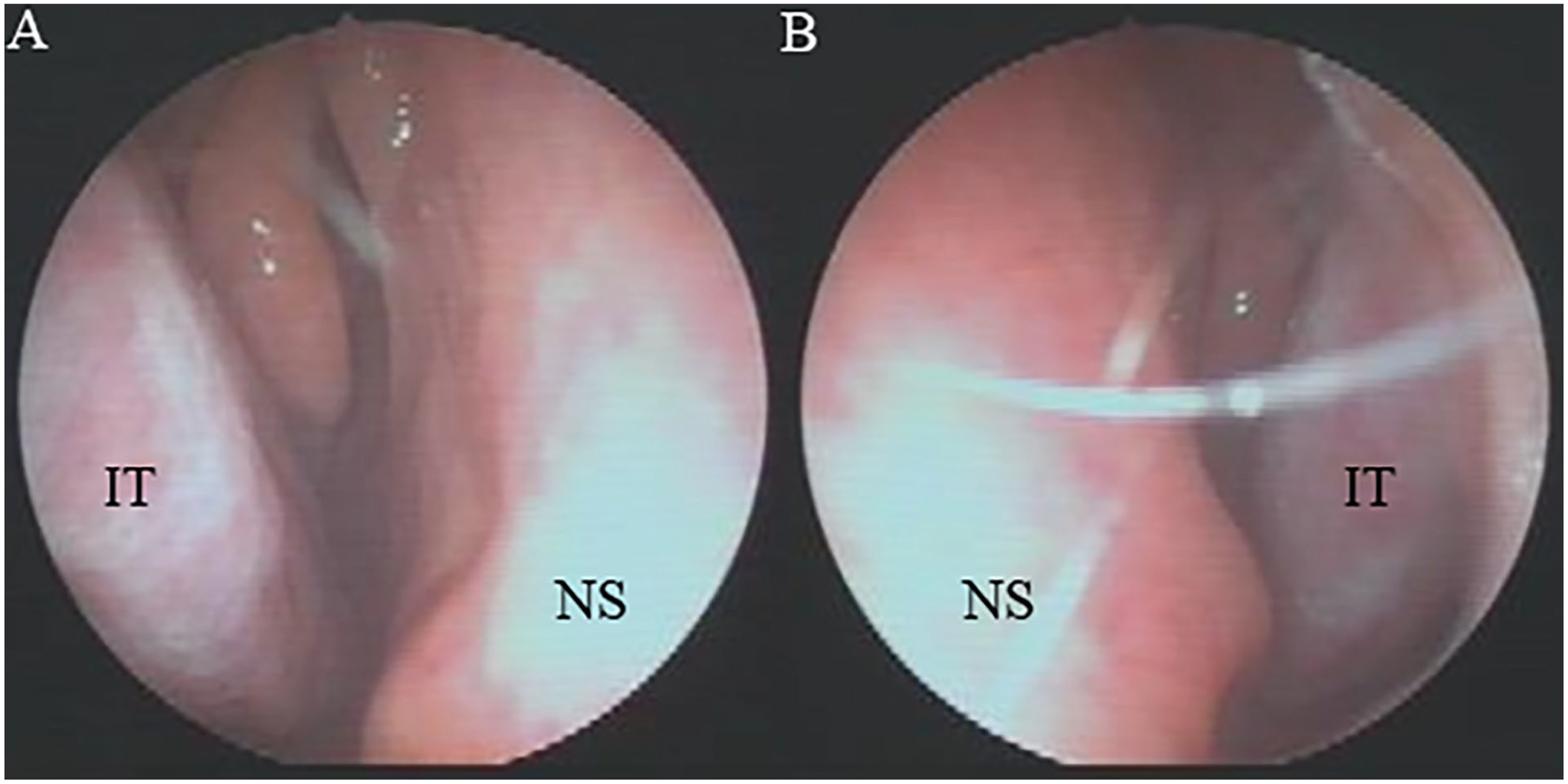
Preoperative nasal endoscopy images of the patient demonstrating deviated nasal septum toward the left side. (A) Right side and (B) left side of the nasal cavity.
The patient underwent elective septoplasty under general anesthesia. After making a hemitransfixation incision of the left septal mucosa, the mucous membranes on both sides of the nasal septum were elevated and the curved cartilaginous septum and bony septum were selectively removed using Jansen-Middleton septum forceps. Silastic splints were inserted into both nasal cavities and nasal packing with Rhinocel®. No excessive bleeding was noticed intraoperatively, and the operation was performed as usual and uneventful. The patient exhibited a progressive increase in nasal bleeding 4 hours after the surgery. Nasal packing was attempted in the patient’s ward but failed to control the nasal bleeding, necessitating the patient’s return to the operating room for hemostasis. Due to the massive nasal bleeding and difficulties in achieving electrocautery and surgical ligation for hemostasis, angiography with embolization was performed as an alternative intervention. She was given 6 units of packed red blood cells, 6 units of fresh frozen plasma, and 1600 ml of platelets. Unexpectedly, extravasation of contrast was observed from the frontal branch of the left MMA during the angiography of the left external carotid artery, and successful superselective embolization was performed (Figure 2A-C). There was absence of rebleeding after the removal of nasal packing the next day, and we did not perform repeat transarterial embolization. We observed the patient for up to 1 year posttreatment, and there were no instances of epistaxis or complications.
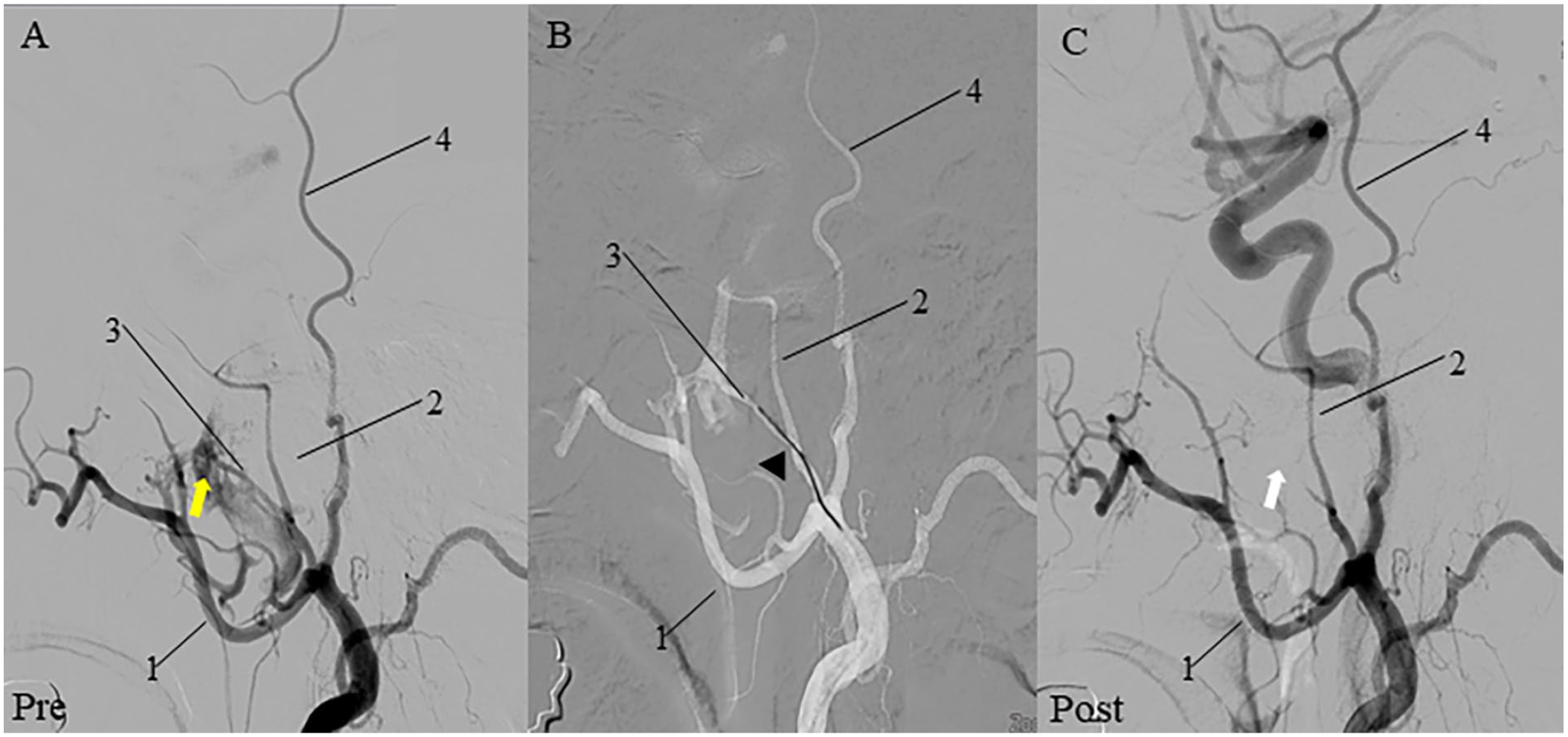
Pre- and post-embolization angiography of the patient. (A) The left external carotid artery angiography shows the extravasation (yellow arrow) of contrast from the frontal branch of MMA. (B) The microcatheter is placed super selectively in the frontal branch of the MMA (black arrowhead). (C) Post-embolization angiography showing no extravasation of dye (white arrow).
Discussion
Septoplasty is one of the commonly performed surgeries by otorhinolaryngologists worldwide. According to the reported data, the incidence of complications after septoplasty ranges from 5% to 60%. 4 It is known that mild oozing can occur for approximately 1 to 2 days after septoplasty. Bleeding or hemorrhage during intraoperative or postoperative septoplasty is reported as one of the most common complications, with true hemorrhage documented at a rate of 6% to 13.4%. 4
Intraoperative acute bleeding during septoplasty is often attributed to the trauma of the highly vascular septal mucosa. 4 To prevent bleeding, the application of topical vasoconstrictors and bilateral lidocaine-epinephrine injection at the septum before making the septal incision is highly beneficial. Furthermore, it is well-known that identifying the subperichondrial and subperiosteal planes is important. Manipulation of the turbinates during septoplasty is considered one of the primary causes of postoperative bleeding. 4 In cases of nasal bleeding occurring after surgery due to the aforementioned reasons, hemostasis is typically achievable through nasal packing or electrocautery. However, in cases of uncontrolled nasal bleeding, there may be a need for additional procedures such as surgical ligation or angiography with embolization of the nasal blood supply.
After the successful treatment of 2 cases of intractable epistaxis in 1974 using angiographic embolization with Gelfoam particles targeting the internal maxillary artery and sphenopalatine artery, 5 therapeutic angiographic embolization has been recognized as an effective and safe method for managing nasal bleeding. Furthermore, angiographic embolization provides a distinct advantage as it allows for the identification of the bleeding source through pre-embolization angiography and enables the procedure to be performed at the most distal vessel of the bleeding site. 6 In this patient’s case, the MMA branch was identified as the source of nasal bleeding, and embolization emerges as a crucial therapeutic approach in situations where surgical hemostasis is not feasible, as exemplified by this case.
To date, 3 cases have been reported in the English literature, describing significant nasal bleeding as a complication of submucosal resection and septorhinoplasty.7 -9 Two cases among these were found to be caused by carotid-cavernous fistula formation,7,8 and the patient with bilateral internal carotid artery injury in 1 case died. 9 The vascular injury observed in the aforementioned 3 cases was attributed to damage to the sphenoid bone and surrounding structures during procedures involving bone manipulation, such as nasal bone osteotomy and septal bone removal. 9 Considering that the primary focus of this case was the correcting of anterior nasal septal deviations, minimal manipulation of the bone was performed during septoplasty. Therefore, the exact cause of the damage to the MMA branch during surgery in this patient remains unclear. The MMA might not be perforated at the time of surgery because there were no signs of immediate bleeding. The mechanism of bleeding in this patient suggests a hypothesis that either a surgically developed pseudoaneurysm or a preexisting one may have ruptured.
The MMA is considered as one of the crucial dural arteries, and serving as a major vessel for transarterial embolization of dural-based lesions. 10 Understanding the complex anatomy of the MMA, including its diverse variations (origins and branches) and dangerous anastomoses, is crucial for the application of the MMA embolization in the treatment of dural fistulas, meningiomas, chronic subdural hematomas, and other related conditions. 10 The MMA bifurcates into 2 branches, anterior (frontal) and posterior (parietal), within the pterional region. Before this bifurcation, the MMA gives the petrosal branch and the cavernous branch. 3 In this patient, the frontal branch of the MMA was identified as the source of the hemorrhage. The frontal branch of the MMA is known to primarily supply to the frontal and anterior parietal convexity, superior sagittal sinus, and the anterior and middle fossa. 3 Therefore, it is not entirely clear how bleeding in the frontal branch of the MMA could manifest as epistaxis. It is known that the frontal branch of the MMA has a possible anastomosis with the anterior and posterior ethmoidal arteries, 3 which might be relevant to this patient.
To the best of our knowledge, this is the first reported case in which epistaxis was treated with embolization of the MMA. Furthermore, this is also the first reported case where the MMA was identified as the cause of nasal bleeding following septoplasty. In cases of unexpected massive postoperative nasal bleeding as a complication of septoplasty, it is advisable to try transarterial embolization, considering the possibility of involvement of vessels not commonly manipulated by otorhinolaryngologists.
Footnotes
Acknowledgements
None declared.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This case was approved by the institutional review board of Nowon Eulji Medical Center (IRB No. EMCS 2023-06-011).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the institutional review board of Nowon Eulji Medical Center (IRB No. EMCS 2023-06-011).
Statement of Informed Consent
The institutional review board of Nowon Eulji Medical Center waived the requirement for informed consent (IRB No. EMCS 2023-06-011). This study is a case report that does not involve collecting or recording personally identifiable information of the patient.
Statement of Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.