
Abstract
We report the case of a 10-year-old girl with a painless slowly growing mass that had developed over the course of 2 years in the left submandibular area. Physical examination revealed a firm painless submandibular mass with no other associated signs. Ultrasound graphics were in favor of a sebaceous cyst. Fine-needle aspiration and magnetic resonance images (MRI) concluded to a pleomorphic adenoma of the submandibular gland. The patient underwent left submandibulectomy. Histopathological examination confirmed the diagnosis of pleomorphic adenoma arising from the submandibular gland. The postoperative course was uneventful. Pleomorphic adenoma of the submandibular gland represents a diagnostic and therapeutic dilemma in children. Preoperative evaluation, including MRI and fine-needle aspiration, is recommended. Total submandibulectomy is also recommended to minimize recurrences and to avoid malignant transformation.
Introduction
Pleomorphic adenoma of the submandibular gland is very rare in children. 1,2 An appropriate diagnostic approach is compulsory in order to provide an accurate evaluation and management of these masses, given their high potential of recurrence and eventual malignant transformation.
Hereby, we report a rare case of a pleomorphic adenoma of the submandibular salivary gland in a child.
Case Report
A 10-year-old girl presented to our department with 2-year history of a painless slowly growing mass in the left submandibular area. The patient denied any fever, trauma, or salivary colic. Physical examination revealed a firm, mobile, and nontender submandibular mass measuring 2 cm, with no skin inflammation (Figure 1). No cervical lymphadenopathy was palpable.
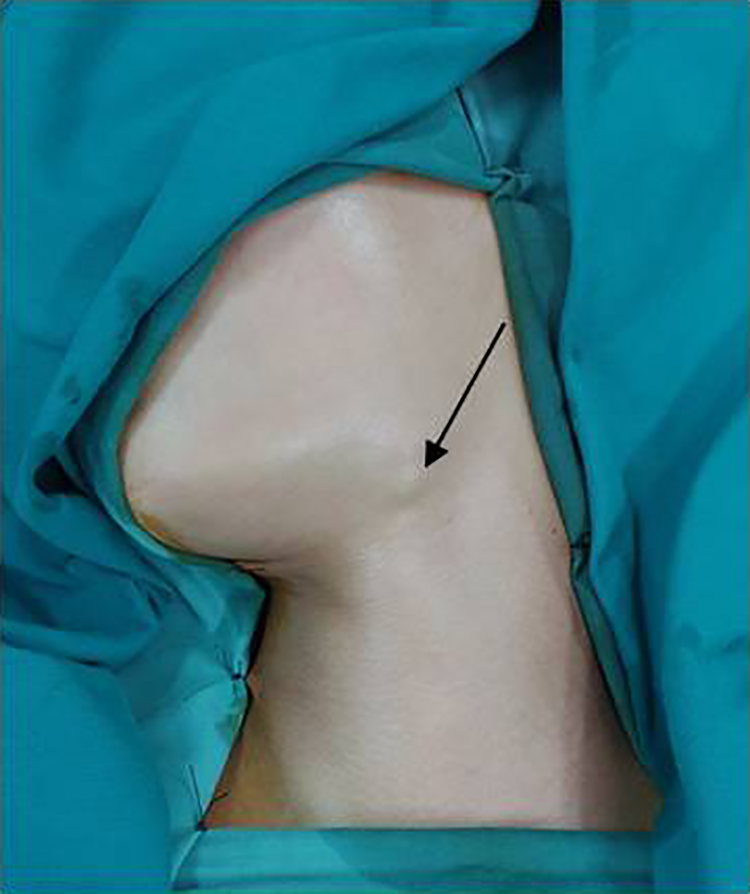
A 2-cm left submandibular mass.
Ultrasound images were suggestive of a sebaceous cyst. Considering the consistency of the mass, fine-needle aspiration (FNA) was practiced and suggested a diagnosis of pleomorphic adenoma (Figure 2).
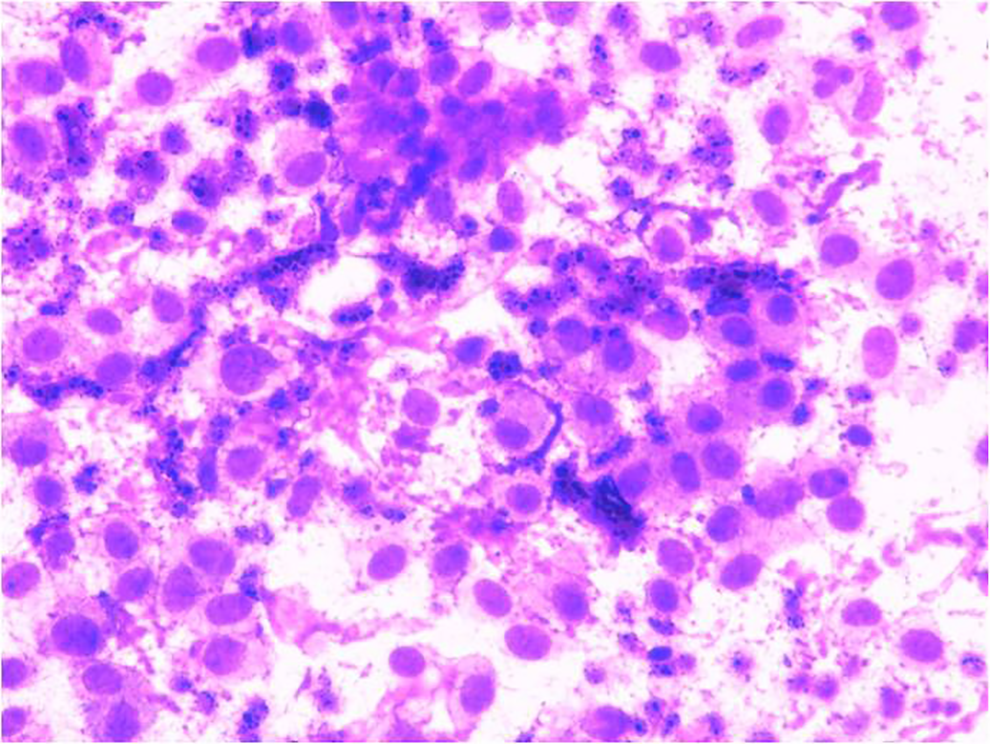
Gland cytology showing pleomorphic adenoma with predominantly plasmacytoid myoepithelial cells and scant fibrillary magenta colored matrix (×400).
Magnetic resonance image (MRI) showed a well-circumscribed bosselated mass measuring 16 × 14 mm, with low signal intensity on the T1-weighted images, on hypersignal on the T2-weighted images with a capsule on hyposignal, and having a heterogeneous enhancement. On diffusion-weighted images (DWI), it appeared of high signal with high ADC (=1.4). The dynamic contrast-enhanced images were type A (Figure 3).
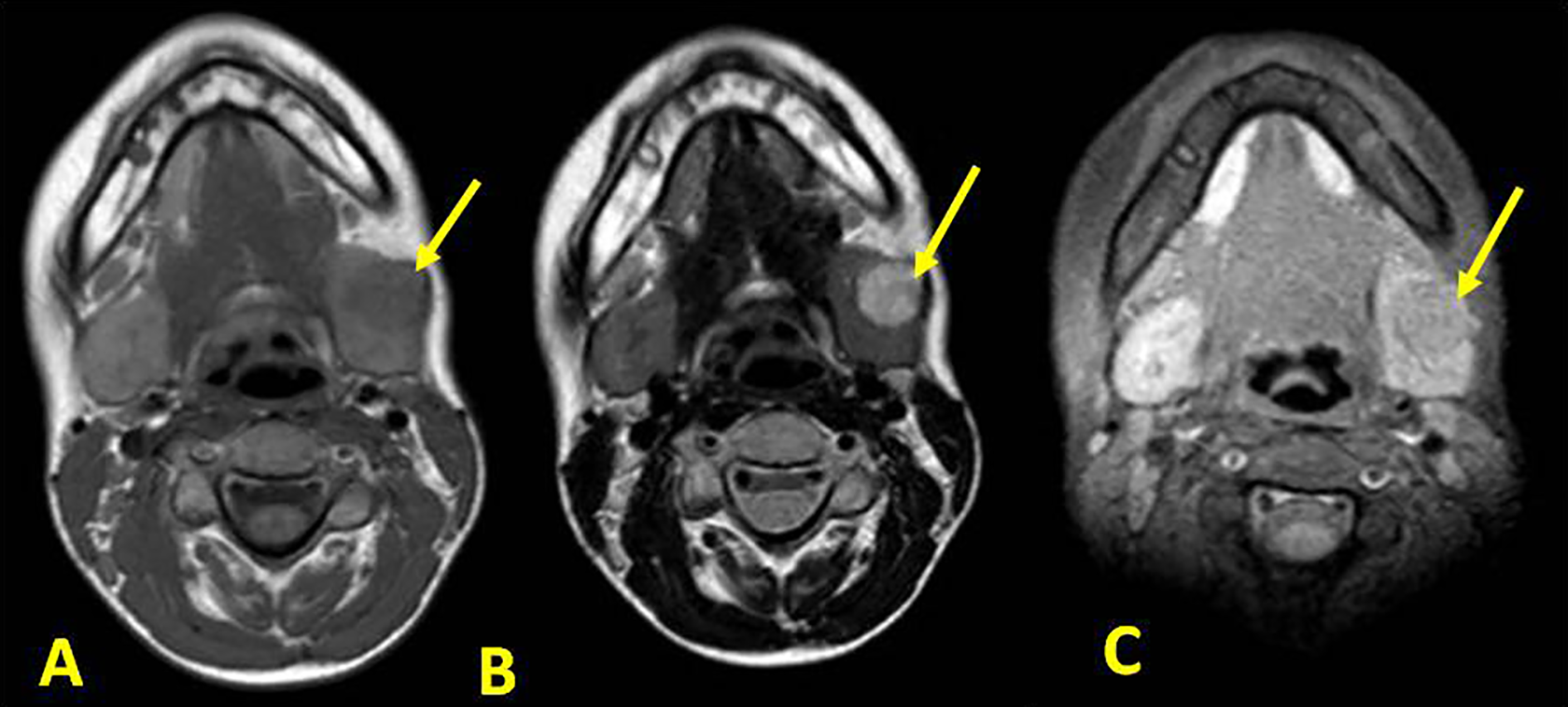
Cervical MRI: (A) the T1-weighted image shows a hyposignal round mass of the left submandibular gland. B, The T2-weighted image shows the mass with hypersignal and well defined borders (C). MRI indicates magnetic resonance image.
The patient underwent surgical treatment consisting in a total left submandibulectomy. The mass was well encapsulated, and there was no infiltration of the surrounding soft tissues such as muscles, nerves, and vessels. The postoperative course was uneventful.
Histopathological examination confirmed the diagnosis of a pleomorphic adenoma arising from the left submandibular gland. No areas of malignant transformation were visualized.
Discussion
Salivary gland tumors are extremely rare in the pediatric population, accounting for less than 5% of all salivary gland tumors. 1 They most commonly develop in the parotid glands (61%), followed by the minor salivary glands (21%) and the submandibular glands (18%). 2
In this location, masses are more likely to be benign, although their rates in the pediatric population are less known than in adults, considering their extreme rarity. The gender ratio is 1:3 in pediatric submandibular pleomorphic adenoma (PA). 3
Patients present often with a permanent painless swelling of the submandibular region, without other associated signs. In most cases, physical examination reveals an isolated, firm, nontender, mobile submandibular mass. Lymph nodes and contralateral tumors are usually absent. No facial weakness is associated. 2
Ultrasound exam is the first line technique in accessible lesions to rule out differential diagnosis. 4 However, it has limited specificity in PA and poor performance in the preoperative planning. 5 It could mislead the diagnosis as reported in our case.
Fine-needle aspiration is a well-established diagnostic technique in adult mass lesions but less applied in cases of pediatric lesions. Because it could be difficult to carry out in children without sedation and has the risk of insufficient cells for accurate diagnosis. 5 When sufficient specimen is obtained, cytology/histology concordance was reported to be 97.5% in PA. 4
Magnetic resonance image is the examination of choice for the characterization of the pleomorphic adenoma. 6 It provides an excellent soft tissue study and a precise analysis of the lesion: its location, size, extent, margins, and signal intensity, 7 without exposure to radiation. But it is time-consuming, costly, and might require sedation for younger children. 2
PA on MRI is described to be homogeneous with an intermediate to low signal intensity on T1-weighted images, inhomogeneous with a high signal intensity on T2-weighted images, and having an inhomogeneous enhancement after gadolinium injection. These characteristics have a high predictive value for the diagnosis of PA, which are signs similar to our findings. 6
Diffusion-weighted images represent a key diagnostic tool of the exam, especially when combined with the ADC values: A study using DWI and dynamic contrast-enhanced MRI found a mean ADC of 1.42 ± 0.35. 8 In the literature, DWI was thought to be more reliable to detect functional changes in parotid glands, compared with submandibular glands.
The treatment of choice for PA in submandibular gland (GSM) is “en block” resection of the tumor along with the gland without disrupting the tumor capsule. More minimal approaches, like enucleation of the tumor, are thought to be avoided since they lead to a high risk of recurrence (30%-80%). 1,4
Several studies have shown an excellent local control for PAs of GSM after total submandibulectomy which contrasts with the rate of recurrence observed for PA of the parotid. In fact, totally encapsulated forms are very predominant, which explains this very low rate of recurrence. 4
Except for tumor recurrence, postoperative complications including the temporary dysfunction of the marginal mandibular nerve or lingual nerve have been reported after total submandibulectomy. 1,3 New modern surgical techniques such as Robot-assisted excision of the submandibular gland by a postauricular facelift approach 9 and trans-oral submandibulectomy are still in the phases of refinement and evaluation. 10
In case of radical surgical treatment, the follow-up is usually uneventful. But the overall risk of recurrence is significant, considering that children who present with a PA typically have a high life expectancy. 11 A study of pediatric PA patients measured the risk of recurrence to be 0.45% per year of follow-up after surgery. 2
On the other side, if the tumor is not operated, malignant transformation might occur. 12 An increase in size is also possible. It could even lead to giant PA since the tumor is painless, slowly growing, and easily neglected by patients. 13 Except for the rare cases of malignant transformation, the prognosis of PA is excellent.
Conclusion
PA represents a diagnostic and therapeutic dilemma. Preoperative evaluation including MRI and FNA is recommended. Total submandibulectomy is also recommended to minimize recurrences and to avoid malignant transformation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.