
Abstract
Background
Warthin's tumor or cystadenolymphoma (CAL) is a benign salivary gland tumor occurring almost exclusively in the parotid gland. CALs of other locations are rare.
Case presentation
We report a laryngeal CAL detected in a positron emission tomography/computed tomography (PET/CT) performed for breast cancer follow-up. The tumor was successfully treated by transoral surgery.
Discussion
Only 14 cases of laryngeal CAL are reported worldwide. These cases confirmed our experience of an uncomplicated and mostly successful transoral resection.
Conclusion
CALs of the larynx are very rare. They are characterized by hypermetabolism in PET/CT. The increasing use of PET/CT investigations in cancer patients could give rise to more incidental findings of CALs at unusual locations such as the larynx.
Keywords
Background
Laryngeal tumors are predominantly malignant, with squamous cell carcinoma being the most frequent histopathological entity. Benign tumors represent around 5 % of all laryngeal tumors, and most of these are papillomas (more than 80 %).
Cystadenolymphoma (CAL) is a benign tumor of the salivary glands, also known as Warthin's tumor or papillary cystadenoma lymphomatosum. CAL affects most often the parotid gland, and is the second most frequent benign salivary gland tumor following pleomorphic adenoma. CALs represent about 10 % of all salivary gland tumors, are most prevalent after the 6th decade of life, have a male predominance, and are more common in smokers. In general, salivary gland tumors of the larynx are rare and malignant forms prevail. Benign salivary gland tumors of the larynx are very rare and therefore poorly documented, despite claims that oncocytic lesions occur more frequently than previously thought [1].
The aim of the present article is to report a case of supraglottic CAL and review all cases of laryngeal CALs in the literature in order to discuss presentation, histological features, management and outcome.
Case presentation
A 61-year-old woman was treated for a lobular carcinoma of the left breast in 2010. She had been disease-free since the end of treatment, but the 2-year follow-up 18 F-fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) showed increased uptake on the left supraglottic region (Fig. 1). With the exception of some intermittent episodes of hoarseness in the recent past, she was without symptoms. The patient is an active smoker and free of professional or environmental exposures.
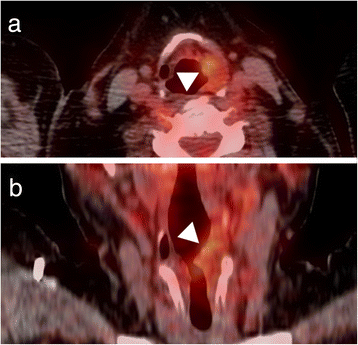
18F-FDG-PET/CT of the larynx. Intense FDG uptake in the left supraglottic region (arrowhead).
Transnasal fiberoptic laryngoscopy revealed a 2 x 1 cm expansive mass involving the left side of the supraglottis. Vocal fold mobility was unaffected. A direct laryngoscopy under general anesthesia was performed (Fig. 2) for biopsy, which revealed a CAL. Complete endoscopic examination of the upper aerodigestive tract was otherwise normal. An MRI showed a 2 × 1 × 3.5 cm multi-cystic lesion of the left supraglottic region (Fig. 3). Therapeutic excision was performed endoscopically under suspension microlaryngoscopy using CO2 laser. Histopathologic analysis of the resection specimen confirmed the diagnosis of a CAL (Fig. 4). The follow-up was complicated by edema of the involved aryepiglottic fold causing moderate dysphagia three months after surgery. A second CO2 laser resection under suspension microlaryngoscopy was performed in order to resect inflammatory and edematous tissue. Further follow-up was uneventful, without any symptoms or signs of recurrence after 2 years.

Direct laryngoscopy. A 2 × 1 cm expansive mass on the left side of the supraglottis (arrowhead; asterisk = anterior commissure)

Fat-suppressed T2 weighted MRI of the larynx. Multi-cystic hyperintense lesion occupying the left supraglottic region (arrowhead).

Histopathology of the laryngeal cystadenolymphoma. H&E staining of the laryngeal CAL showing oncocytic epithelium (arrowhead) surrounded by lymphoid stroma (asterisk) (magnification 40×)
Discussion
Summary of published cases of laryngeal cystadenolymphoma

Abbreviations: M – male; F – female; FR – full recovery; NR – not reported
Male to female ratio was 2:13, and patients’ mean age was of 64.2 ± 10.99 years (range: 45–80). The clinical presentation was not disease–but organ-specific, reflecting laryngeal involvement, with hoarseness as leading symptom in 7, dyspnea in 3, and dysphagia in 2 patients. One patient presented with neck swelling. The location was exclusively supraglottic, with glottic involvement in only one of the cases. One case showed a bilateral CAL. Two patients presented CAL within a laryngocele. Tumor size ranged between 1 and 4.5 cm. In 2 cases, synchronous CALs of the parotid gland were seen. Transoral resection was performed in 9 out of 11 patients, and 2 underwent open transcervical resection. In most cases (9 out of 11 reported) one surgical procedure was sufficient to eradicate the tumor, whereas in one case 4 operations were needed for recurrent disease and the second case showed tumoral persistence after 4 months. Our case underwent a second operation due to persistent supraglottic edema with no residual CAL during definitive histopathologic examination. Another 2 cases showed persistent laryngeal edema postoperatively.
In summary, laryngeal CAL is very rare and can most often be managed with transoral resection. Recurrence seems to be an exception in the larynx and only few complications or side effects of the treatment are reported. The unique feature of our reported case is that the patient's CAL was detected incidentally due to regular PET/CT follow-up investigation for a previously treated breast cancer. Only retrospective inquiry showed minor laryngeal symptoms consisting of some hoarseness episodes. Accurate diagnosis requires nonetheless histopathologic examination of the resected specimens. Malignant degeneration of CALs, originating from both the epithelial and the lymphoid compartments, is a rare but possible event. In the specific case of laryngeal CALs, no case of malignant degeneration could be identified.
Workup with PET/CT has been shown to indicate false positive results in head and neck cancer patients showing a CAL within neck lymph nodes mimicking a metastasis [14]. There was similarity with our case, where FDG-uptake was found in the larynx, and initially mistaken for a breast cancer metastasis. Van der Wal et al. described the largest series of laryngeal CALs (3 cases) along with seven other cases of extraparotideal CALs (cheek, oropharynx, palate, buccal fold, lower lip, submandibular gland) [11]. As CALs show a hypermetabolism in PET/CT exams, which are increasingly performed, future PET findings might bring new insight regarding synchronous and multiple Warthin's tumor locations and into pathogenesis of this particular tumor. While some authors have classically considered CAL to be more similar to a reactive process than to a true neoplasia, the views on pathogenesis have evolved over the last decades. Current techniques show that the epithelial portion of a substantial subset of CALs is monoclonal and frequently harbors a translocation between chromosomes 11 and 19 t (11;19), which in turn results in the fusion oncogene CRTC1-MAML2 [CREB(cAMP response element-binding protein)-regulated transcription co-activator 1–mastermind-like protein 2], which is a master key involved in several signaling pathways that contribute to cell survival and proliferation, primarily the Notch pathway [15]. Van der Wal et al. underlined the fact that laryngeal CALs are indeed rare tumors and pathologic diagnosis can be challenging, especially when it comes to distinguishing CAL from oncocytic hyperplasia or metaplasia, pointing out that the only basic difference between these entities is the lack of lymphoid stroma in oncocytic lesions [11].
Another interesting point is the potential multifocal presentation of CALs. We found 2 cases of concomitant involvement of the larynx and the parotid gland (Table 1) [9, 12]. This is not a new finding, as synchronous or metachronous development of CALs in both parotid glands is not a rare event, which raises the question if there is a need for long-term follow-up in patients with CALs in general. Although speculative in nature, we feel that careful workup in incidental PET/CT findings could reveal a previously underestimated amount of extra-salivary and multiple synchronous CAL cases. In light of the open questions regarding the pathogenesis of CALs, more cases as the present ones could bring further insight into the nature of this special benign tumor.
Conclusion
Warthin's tumors of the larynx are very rare. Transoral resection seems to be feasible for most cases, has little side effects, and is most often curative. As Warthin's tumors show increased FDG-uptake similar to malignant tumors, it is hypothesized that with increasing PET/CT use, the number of Warthin's tumor case reports outside the salivary glands may augment.
Consent
The patient has given her consent for the Case report to be published.
Footnotes
Acknowledgements
The authors wish to thank Mrs. Irina Ciorba-Nisa, MS, and Mr. Krzysztof Szmigiel, scrub nurse, for their skillful assistance during production of this manuscript and translation of several articles.