
Abstract
Introduction
Adenoid cystic carcinoma (ACC) is a malignant tumor that most occurs in the salivary glands but rarely seen in the nasopharynx, 1 which accounts for 0.13% to 4% of all nasopharyngeal carcinomas (NPCs).2,3 Previously, ACC was first described as “cylindrome” by Bilroth in 1856. Common clinical features included slow tumor growth, nerve infiltration, aggressive clinical course, high tendency of local recurrence (LR), and distant metastasis. Myoepithelial and epithelial neoplastic cells create 3 unique development patterns in ACC: cribriform, tubular, and solid; sometimes, more than one pattern is observed in a single tumor.1,4 Nasopharyngeal ACC (NACC) is distinguished by advanced T-stage at presentation, invasion of the skull base, frequent perineural invasion (PNI), and positive margins.5,6 NACC is considered to have a higher proportion of solid pattern, which is also more aggressive with poorer prognosis. 7
ACC of nasopharynx is rare, and most studies were case reports with conflicting conclusions of treatment. Therefore, there is no agreement on the optimal time and standardized therapy for NACC. The purpose of our study was to analyze the clinical features of 12 patients with NACC in our hospital and report our clinic treatment experience of NACC.
Methods
Our study retrospectively enrolled 12 patients diagnosed with NACC who undertook endoscopic nasopharyngectomy at the Department of Otorhinolaryngology of Eye, Ear, Nose and Throat Hospital Affiliated to Fudan University from January 2019 to January 2021. Evaluation of the specimen confirms the diagnosis of NACC and helps in the grading of the cancer. The patients’ medical records were summarized for clinical symptoms, radiologic images, immunohistochemical staining, treatment, and follow-up data. Follow-up time was calculated from the beginning of treatment in our hospital to the date of the outcome. This study was permitted by the Ethics Committee of the Affiliated Eye, Ear, Nose, and Throat Hospital at Fudan University.
Results
Clinical Characteristics
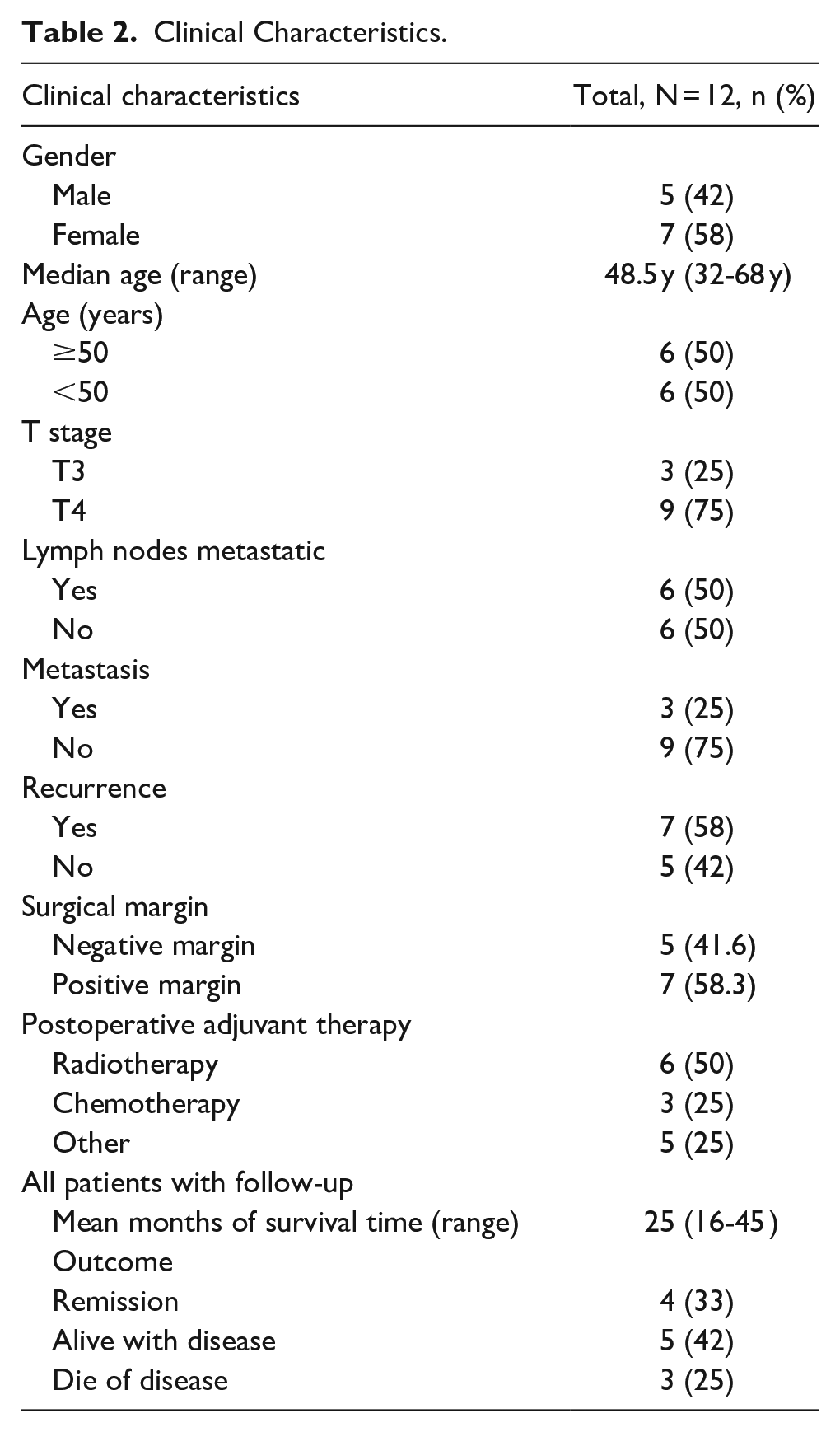
The clinical data of 12 patients with ACC of nasopharynx receiving endoscopic endonasal approach (EEA) in our hospital were analyzed. Table 1 shows the clinical features of the patients. The prevalence rate for men and women were significantly different, with 5 male patients and 7 female patients (5:7). They were all adults, ranging in age from 32 to 68 years (mean 40.7, median 48.5). The symptoms differed depending on where the lesion was located. The most prevalent symptom among the 12 individuals was epistaxis (n = 7). Other local symptoms included facial swelling and pain (n = 4), headache (n = 4), ear stuffy (n = 3) and hearing loss(n = 3), rhinobyon (n = 3), decreased vision (n = 2), and tinnitus (n = 1).
Features of 12 Cases With Nasopharyngeal Adenoid Cystic Carcinoma.
Radiologic Findings and Abnormal Laboratory Results
All patients undertook preoperative diagnostic imaging, including enhanced computed tomography (CT) and enhanced magnetic resonance imaging (MRI). If the tumors involved with cavernous sinus, brain stem infiltrated, and internal carotid artery circumvented, patients will undertake MRA/MRV to clearly show lesion region and the relationship with internal carotid artery. We showed typical image of NACC in Figures 1 to 3. Before surgery, we recommended they receive 18F-fluorodeoxy glucose positron emission tomography (PET)/CT to exclude gross distant metastasis. Among all the 12 patients, 11 underwent PET-CT to rule out distant metastasis. Only one patient chose the alternative method for financial reasons (Case 1). Therefore, we recommended her to use head enhanced MRI, chest CT, neck lymph node ultrasound, abdominal ultrasound, and bone scan to save costs. While MRI is superior for evaluating soft tissue extension, CT is better at defining bone invasion. MRI is clearly superior to CT for assessing nerve invasion. Combined with the results of CT and MRI, we identified 3 (25%) patients with T3 and 9 (75%) patients with T4. Since most of our patients had recurrent tumors, half of them had already developed lymph node metastases. There were 1 case with bone metastasis and 2 cases with lung metastasis.
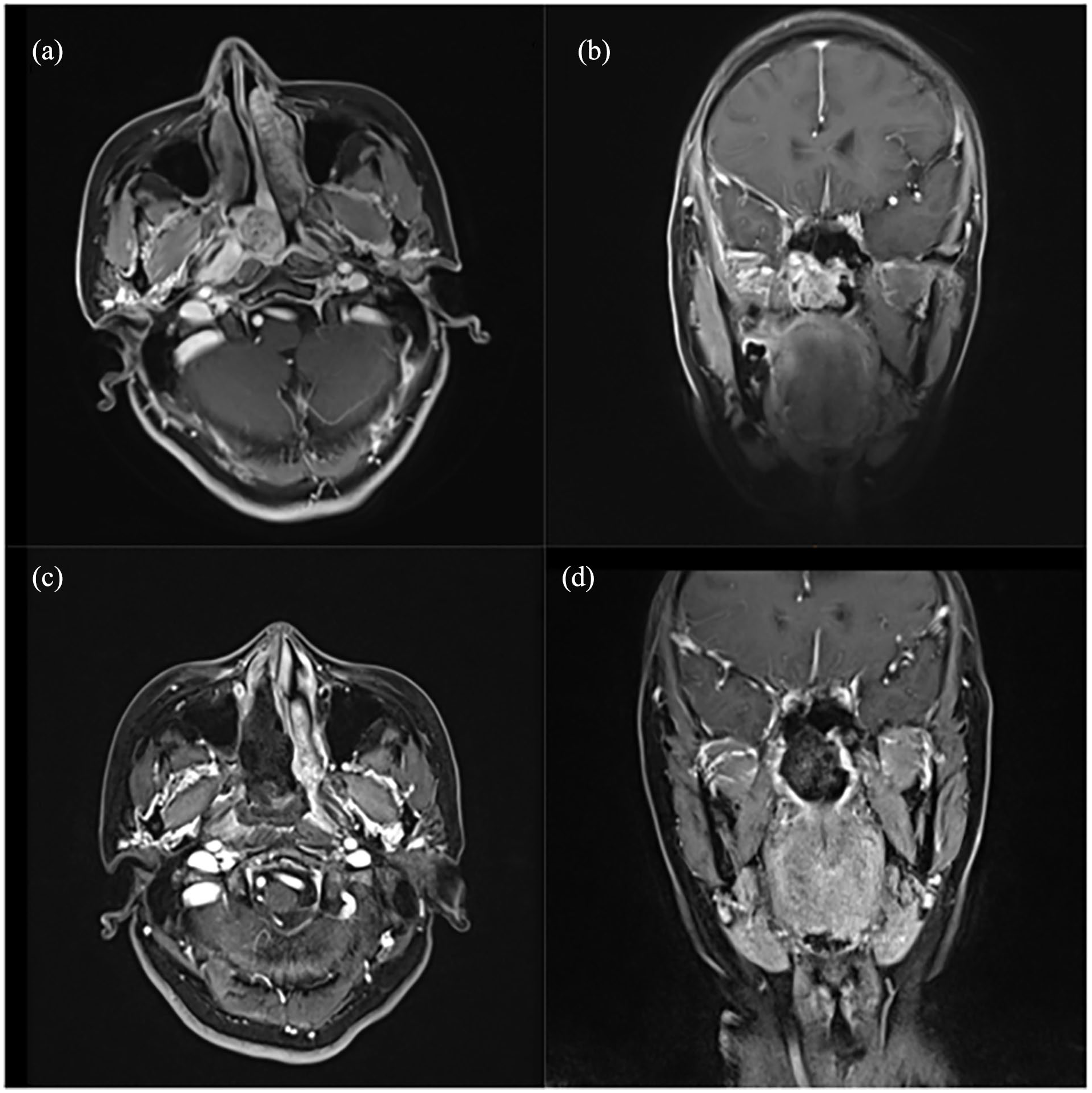
A 55-year-old woman complained of nasal obstruction and epistaxis lasting for 1 year. She underwent a complete resection of tumor. She did not receive postoperative radiation therapy. Both the clinical and imaging manifestations improved after a 45 month follow-up. The figure displayed the axial and coronal MRI images pre-[(a) and (b)] and post-surgery [(c) and (d)] (Case 1). MRI, magnetic resonance imaging.
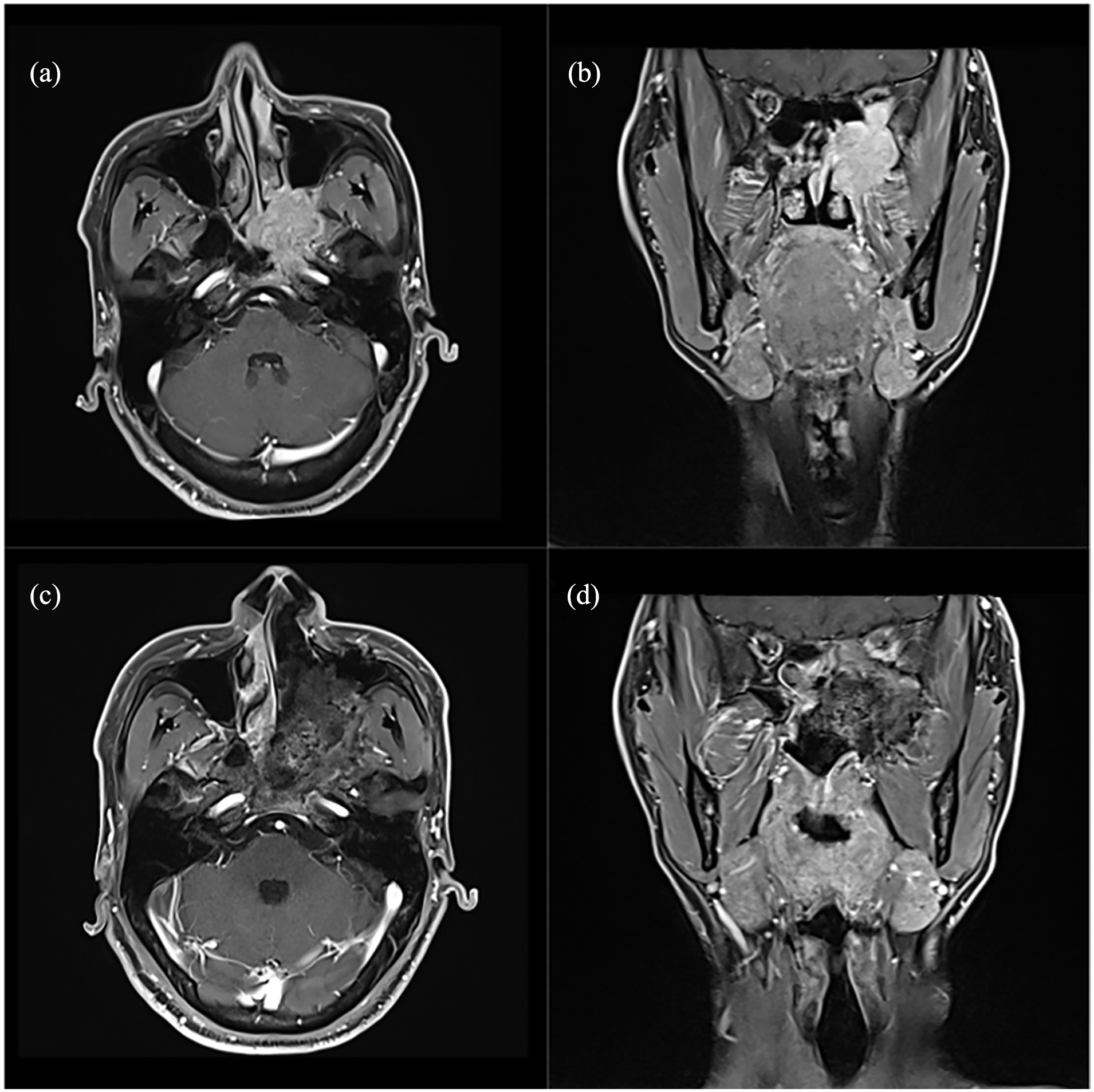
A 39-year-old man complained of headache and epistaxis lasting for 4 months. He underwent a partial excision of tumor. The surgical margin was positive, and he receive postoperative radiation therapy. But after 9 months follow-up, bone metastases were found. Seven months later, he died unfortunately. The axial and coronal MRI images before [(a) and (b)] and after [(c) and (d)] surgery were shown in the figure (Case 3). MRI, magnetic resonance imaging.
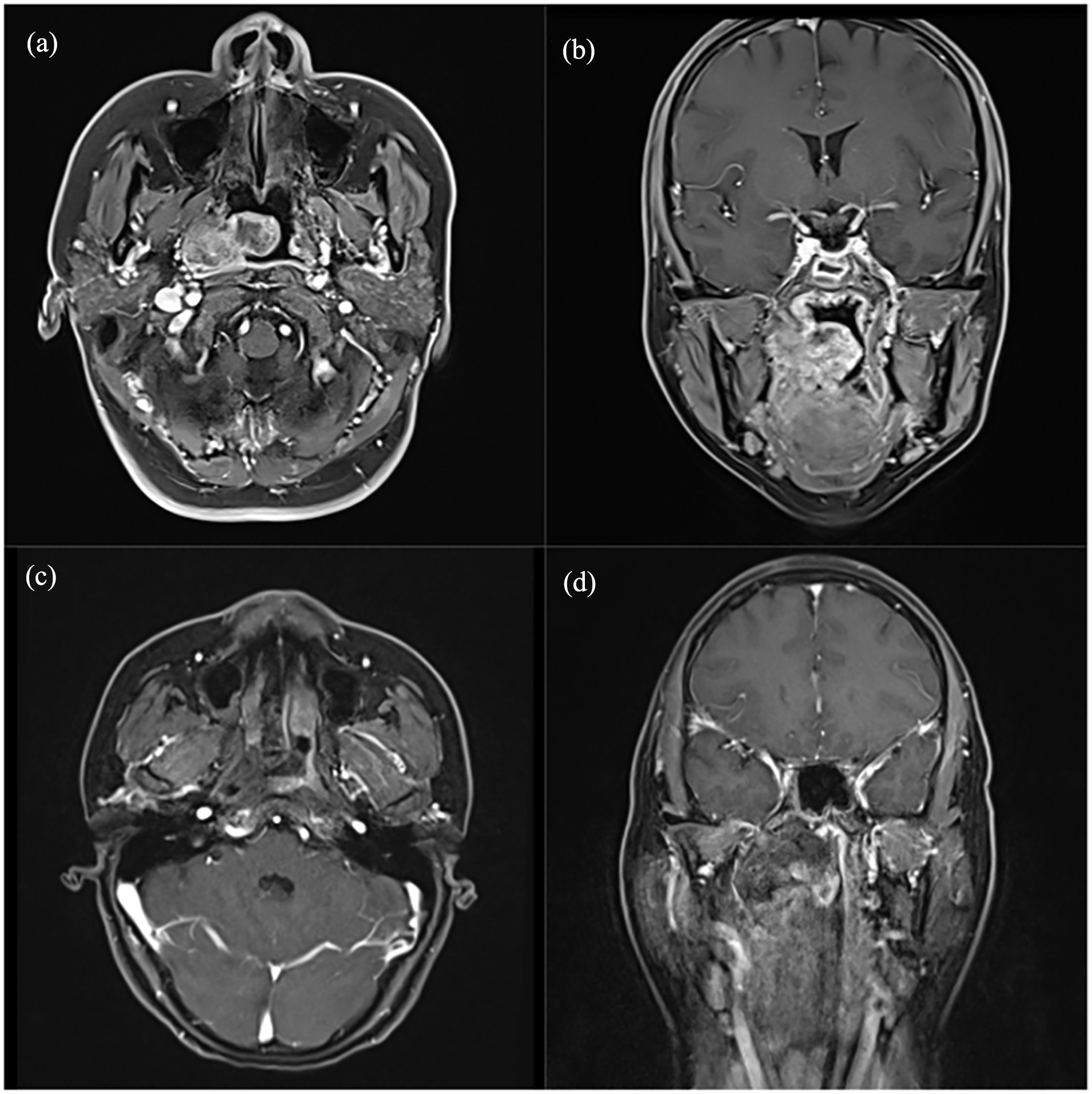
A 40-year-old woman diagnosed with nasopharyngeal ACC received surgery and radiotherapy. After 16 months of follow-up, her tumor had completely subsided. The top figure displays the MRI taken prior to treatment [(a) and (b)], while the bottom image was taken 1 month after surgery [(c) and (d)] (Case 11). ACC, adenoid cystic carcinoma; MRI, magnetic resonance imaging.
Histological Characteristics and Immunohistochemical Staining
Microscopy histopathological examination has demonstrated that ACC are asymmetrical tumors with different growth patterns, such as invasive or lobulated growth patterns. ACC is mainly composed of nonluminal cells, basaloid, hematoxyphilic cells with small to medium size of cytoplasm, while the luminal, short cuboidal, and eosinophilic cells are much less. Three different structural patterns—tubular, cribriform, and solid—have been identified. Most histological patterns were not available because this was a retrospective study.
Among the patients, 12/12 (100%) was positive for Ck-pan, p63, vimentin, though weakly. 11/12 (92%) were positive for CD117 and HHF35 (shown in Table 2); 10/12 (83%) were positive for S100; 8/9 (87.5%) were positive for SOX10; 8/8 (100%) were positive for P16, 4/5 (80%) were positive for CK7; 3/8 (100%) were positive for NF. The Ki-67 proliferative index ranged from less than 1% to 30% in 7 patients, while there were 3 patients with Ki-67 proliferative index greater than or equal to 30%.
Clinical Characteristics.
Treatment and Follow-Up Data
All enrolled patients were confirmed by pathological diagnosis and underwent endoscopic resection surgery. For patients with NACC who have never received radiotherapy, we recommend postoperative radiotherapy for all patients. The postoperative radiotherapy dose was 54 to 70 Gy and the median dose was 66 Gy. Seven patients had recurrent ACC. Among them, 6 patients had received radiotherapy before surgery. Because repeated radiotherapy may slow down wound healing, cause necrosis of the operative cavity, and increase the risk of internal carotid artery rupture, we do not recommend repeated radiotherapy for these patients. NACC is surrounded by many important large blood vessels and nerves, so it is difficult to remove the tumor completely. Thus, complete tumor resection was only achieved in 5/12 (41.6%) of patients, and microscopically positive margins were found in 7/12 (58.3%) of patients. Case 4 underwent neoadjuvant chemotherapy before surgery because the tumor was adjacent to the internal carotid artery. Three patients who had bone and lung metastasis, respectively, underwent partial resection of tumor for unbearable headaches and nosebleeds. Among 3 patients with distant metastases, 2 patients received paclitaxel plus cisplatin (TP) after surgery. The other patient underwent surgery to relieve pain and received no treatment after surgery.
The follow-up data were available for 12 patients with the follow-up period ranging from 16 to 45 months (median, 25 months). Among the 12 patients followed up, 3 died of the disease (2 patients died of distant metastasis within 18 and 20 months after the surgery, and another patient with recurrent NACC died of hemorrhage), whereas 5 patients were stable (alive with disease, but there are various degrees of improvement and no disease progression) and 4 patients were in remission. One patient had difficulty opening his mouth 1 month after surgery, but his condition improved after training of mouth opening. Compared to traditional open surgery, there was no perioperative mortality, meningitis, cerebral spinal fluid (CSF) leak, or cerebrovascular accident. Two patients were dead of distant metastasis within 18 and 20 months after the surgery, and another patient with recurrent NACC died of hemorrhage.
Discussion
NPC is a malignant tumor with high prevalence in Southern China. Squamous cell carcinoma is the main histological form of primary NPC. ACC is a malignant tumor arising from secretory glands like maxillary sinus but rarely occurs in nasopharyngeal region. Therefore, nasopharyngeal adenocarcinoma is rarely seen and only accounts for less than 0.13% to 0.48% of all nasopharyngeal cancers.1,2 Compared to typical nasopharyngeal malignancies, our study showed that NACC is an uncommon nasopharyngeal malignancy with unique biological characteristics and different therapeutic policies.
To our knowledge, this is the biggest retrospective study conducted at a single institution that summarizes the clinical characteristics and assesses the management strategies for advanced NACC that has been published to date. NACC is a woman preponderance disease and our study reported that the male to female ratio of cases was 5:7, which agrees with previous reports.2,8 Compared with other studies, our study demonstrated a 50% degree of nodal involvement, which is significantly higher than historical reports that range anywhere from approximately 3.8% to 15%,2,9,10 but clearly lower than NPC (64%-88%). However, it is reasonable because we received a higher risk population with more advanced, recurrent tumors or with comorbidities which might have influenced nodal involvement and worse prognosis.6,8 In contrast to typical nasopharyngeal malignant tumors, NACC exhibits a unique biological mode of PNI. Eight of the 12 (66%) patients in our study had invasions of the optic, oculomotor, and trigeminal nerves. Distant metastases were found in 25% of patients with ACC of nasopharynx. A poor prognosis may result from the tumor’s propensity to migrate along nerves to the orbital or cranial cavities. Moreover, these lesions frequently have advanced stages at diagnosis and may be linked to significant bone loss, making surgical removal more challenging.
The etiology and pathogenesis of the NACC are still unknown. Unlike most NPC pathological types, previous studies have identified that the development of NACC has little relationship with the infection of Epstein-Barr virus.11-14 Chemotherapy and multikinase inhibitors that target the vascular endothelial growth factor receptor (VEGFR), such as axitinib and lenvatinib, are now the available systemic treatments. In addition, a case study combining cetuximab with induction chemotherapy and concurrent chemoradiotherapy was published. This combination treatment was well tolerated and produced encouraging local and objective responses. 15 In general, VEGFR inhibitors result in an about 85% illness control rate and an objective response rate of 10% to 15%. 16 One noteworthy finding in other study suggest aggressive adjuvant therapy may be beneficial with intermediate-/high-grade tumor. 17 The presence of patient preference, symptoms, tumor burden, tumor growth rate, and tumor growth rate should all be considered when determining whether to begin. Therefore, we predicted that provable advantage of chemotherapy in NACC is the low propensity for nodal spread but not cure cancer patients.
There is no consensus on standardized treatment protocols. Previous studies have suggested that primary NPCs are usually treated with radiotherapy or chemoradiotherapy. Since radiation therapy is not very effective in treating ACCs, surgery is considered the most appropriate treatment for NACC. 18 A prior study found that the majority of individuals with sinonasal adenoid cystic carcinoma and NACC were T4a or T4b, which was considered “traditionally unresectable.” 17 Traditional treatment strategies of sinonasal and nasopharyngeal adenoid cystic carcinoma (SNACC) results in craniotomy, pathological facial incisions, craniotomy, dural removal, cavernous sinus resection, and cavernous sinus resection. Ramakrishna et al reported that negative margins are only attained 50% of the time with vigorous, open surgery, and there has been little improvement in overall survival (OS) or disease-free survival (DFS) since the 1960s.6,19-21 EEA has recently acquired popularity and provides comparable therapeutic outcomes when utilized for sinonasal malignancy. The advantages of EEA including no facial incisions, less neural manipulation, reduced length of hospital stay, improved visualization, and shortened time to initiation of adjuvant therapy. Our results showed that the negative margin rate of endoscopic nasal surgery was 41.6% in patients with advanced NACC. Besides, there were no postoperative complications in these patients. EEA offers a balance between survival and quality of life, decreasing morbidity for patients with this difficult to cure disease. Endoscopic nasopharyngeal resection for nasopharyngeal malignancies is feasible and safe in appropriately selected patients. 18 However, endoscopic surgery is highly technical for doctors, who need specialized equipment and a surgical team skilled in endoscopic tumor surgery. Long-term follow-up is required.
The literature on endoscopic treatment of nasopharyngeal ACC is limited. Because of limited endoscopic surgical skills, surgery for NPC is frequently applied to biopsy specimen or the salvage of chosen patients with residual or persistent local or recurrent regional malignancy. Pervious study showed that less than one-third of patients using the EEA had microscopically negative margins. 17 This suggests that NACC may require a comprehensive approach. Current treatment modalities suggest that aggressive surgical resection with negative margins and adjuvant radiotherapy provide the best prognosis for NACC. The research of Kashiwazaki et al shows that organ-preserving EEA with adjuvant radiotherapy (RT) for low-grade NACC have comparable outcomes when compared to other sites treated with surgery and adjuvant radiotherapy. 17 As for patients with high-grade tumor, they got poor outcomes and may benefit from novel treatment strategies. 17 Previous study showed that patients treated with surgery and combined modality therapy (CMT) live longer than RT alone.2,8 Patients with NACC were treated with the EEA and RT, which avoid internal carotid artery injury, optic nerve injury, and CSF leak. 17 The 5 year survival rate was comparable to that reported by other research. Another study of 36 cases found no difference in overall survival between CMT and RT alone. 22 There is no approved treatment for recurrent or metastatic ACC, and there is no ideal timing to begin systemic therapy. Re-irradiation is not recommended because it may result in serious side effects like soft tissue necrosis, brain necrosis, osteoradionecrosis, severe trismus, cranial neuropathies, and hearing loss. Few literatures concluded conflicting results, which offer little guidance to treatment. Our single-institution study represents the largest series of NACC treated by the EEA with a mean follow-up time of 25 months. Because this study was retrospective and the baseline of patients enrolled was inconsistent, no definitive conclusions could be drawn about treatment options. However, we have expanded the NACC database and may provide some data and reference significance for other researchers. Our study suggests that EEA might be a better option than traditional treatment strategies for patients with advanced NACC. Further studies with more patients and longer follow-up times would be implemented.
The factors affecting survival rate of NACC remain unclear. A study summarized the treatment patterns of NACC in 11 clinical studies in the United States, the presence of nodal involvement as well as distant metastasis independently predicted for shorter OS, 8 while PNI and adjuvant therapy had no impact. 23 Recurrence rate was related with primary tumor site, infiltrative pattern, positive surgical margins, and PNI. 17 Prokopakis’s studies analysis of 58 patients undergoing surgery for ACC of the head and neck, suggesting that local recurrence rates were decreased in patients with negative surgical margins who were irradiated. 24 Other study showed that surgery with adjuvant RT yielded significantly better local control instead of better OS. 25 Patients with ACC of the skull base have advanced illness, and their survival is determined by distant metastasis, which frequently occurs within 3 years. 26 Liu et al 2 has concluded that patients suffering from cranial nerves invasion, advanced stage, and surgical treatment showed a significant worse OS. Meanwhile, stage and surgical treatment were independent factors affecting OS. Due to the low incidence of NACC and the small number of cases in the multivariate analysis, a large multicenter study is needed to further evaluate the treatment strategy and prognostic factors of NACC.
Shortcomings of this study include its small sample size, retrospective approach, and lack of comprehensive histopathological characteristics. In addition, the relationship between histological features and prognosis is unclear. Also, individual dosages and duration of treatment in drug therapy and radiation therapy were not identical among enrolled patients. In most of our cases, different treatments are given simultaneously or sequentially. As a result, it is difficult to assess the exact effects of different treatments.
In conclusion, NACC is a rarely seen malignant tumor in nasopharynx. For patients with advanced staged NACC or recurrent tumors who have received radiation therapy, EEA may be the most favorable treatment choice with the least amount of complication. The standard treatment for NACC needs multicenter study data and longer follow-up time.
Footnotes
Acknowledgements
I would like to thank the pathology experts of the Eye, Ear, Nose and Throat Hospital Affiliated to Fudan University for the diagnosis of nasopharyngeal adenoid cystic carcinoma and the immunohistochemical results provided.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Yujie Chen and Yuxuan Shi. The first draft of the manuscript was written by Yujie Chen and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data Availability
The data used to support the findings of this study are available from the corresponding author on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Natural Science Foundation of China Grants (81970856 to H.Y.); the New Technologies of Endoscopic Surgery in Skull Base Tumor: CAMS Innovation Fund for Medical Sciences (CIFMS; 2019-I2M-5-003 to H.Y.).
Ethics Approval
This study was permitted by the Ethics Committee of the Affiliated Eye, Ear, Nose, and Throat Hospital at Fudan University.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.