
Abstract
A variety of diseases can affect the nasal vestibule. It might be challenging to diagnose and treat a nasal vestibular tumor due to the anatomical characteristics of the nasal vestibule. Neurilemmoma is a tumor derived from Schwann cells of the nerve sheath. Less than 4% of these tumors invade the nasal cavity and sinuses. Nasal vestibule neurilemmoma is rare, it is often overlooked when a mass discovered. The diagnosis of it is mainly based on clinical symptoms, nasal endoscopy, and imaging, The mainstay of treatment is complete resection surgery. Pathological examination provides the final diagnosis. We present a patient with nasal vestibule neurilemmoma who underwent a successful endoscopic surgery without cosmetic deformity, and discuss the clinical manifestations, histological features, imaging features, differential diagnosis, treatment options, then reviewed relevant literature of this rare benign lesion.
Introduction
Neurilemmomas arise from Schwann cells, which are also known as schwannomas. The vast majority of them are benign neural sheath tumors that are subdivided into neurilemmomas and neurofibromas. 1 Malignant tumors accounting for fewer than 5% of all. 2 Most neurilemmomas occur in the parapharyngeal spaces of the head and neck, accounting for 25% to 45% of the overall incidence,3,4 Involvement of the nose and paranasal sinuses is rare and only occurs in 4% of cases. 5 Neurilemmoma in the nasal vestibule is extremely rare. Except for the optic and olfactory nerves, which lack these cells, neurilemmomas can occur in all peripheral nerves.3,6 Although trigeminal nerve neurilemmoma is uncommon, it is the second most prevalent type after vestibular neurilemmoma, and is hypothesized to be the origin of nasal neurilemmoma.6,7 They commonly present as a painless slow-growing swelling and lesion without any neurological symptoms, and usually manifested as unilateral isolated lesions.3,5 They are rarely reported cases, and in this study, we describe a patient with nasal vestibule neurilemmoma who underwent an endonasal endoscopic treatment for complete resection and review the literature about it. We aim to make physicians aware of the rare case of nasal vestibule neurilemmoma to guide clinical decision-making.
Case Report
A 30-year-old female patient was admitted to the Department of Otolaryngology of the First Hospital of Jiaxing with a 3 years history of left nasal vestibule painless tumor. She presented with swelling sensation of the left nose, accompanied by itching of the region. More than 1 year ago, the left-sided mass in the nasal vestibule gradually increased without any associated symptoms such as nasal obstruction, epistaxis, or rhinorrhea. The patient did not experience other abnormal sensations or numbness. She once visited to the ENT department of the First Hospital of Jiaxing. And after physical examination, she was diagnosed with “nasal vestibular cyst” and surgical intervention was suggested. Recently, the patient visited our outpatient clinic for a second opinion. She denies any other systemic diseases history and had never undergone surgery, and denies intaking any medication/food that could cause allergic manifestations. The external nose is slightly deformed and deviated to the right. Endoscopic examination revealed a 1.3 cm × 1.3 cm sized, skin-colored, smooth-surfaced, moderate texture mass in the left nasal vestibule. No evident ulcers or necrosis were found. Computed tomography (CT) scan revealed a clearly demarcated round-like slightly hypodense shadow measuring about 1.3 cm diameter in size occupying the left nasal vestibule region. The maxillary sinus, frontal sinus, septal sinus, and pterygoid sinus on both sides were well pneumatized, no abnormal density shadow was seen in the cavity. And no abnormality in the nearby tissues or bone destruction were observed (Figure 1). Both the endoscopic and radiological features suggested the possibility of soft tissue benign tumor. Indicators of routine blood, serum biochemistry, and coagulation function revealed no abnormalities. The chest radiograph, cardiac ultrasound, and electrocardiogram were all normal. There are no clear surgical contraindications, so the endoscopic surgery was performed under general anesthesia. An incision was made in the left nasal vestibule, a blunt separation was carried out then. During the operation, the yellowish oval-shaped tumor with smooth capsule was detected and completely removed. A repetitive Antoni A type pattern with clumped fusiform cells and an Antoni B type pattern with fewer cells were both seen during a histologic examination. What’s more, the tumor cells were immunoreactive for S-100 protein (Figure 2). These features confirm the final diagnosis of neurilemmoma. The disease showed no recurrence during a subsequent 28 month follow-up period (Figure 3).
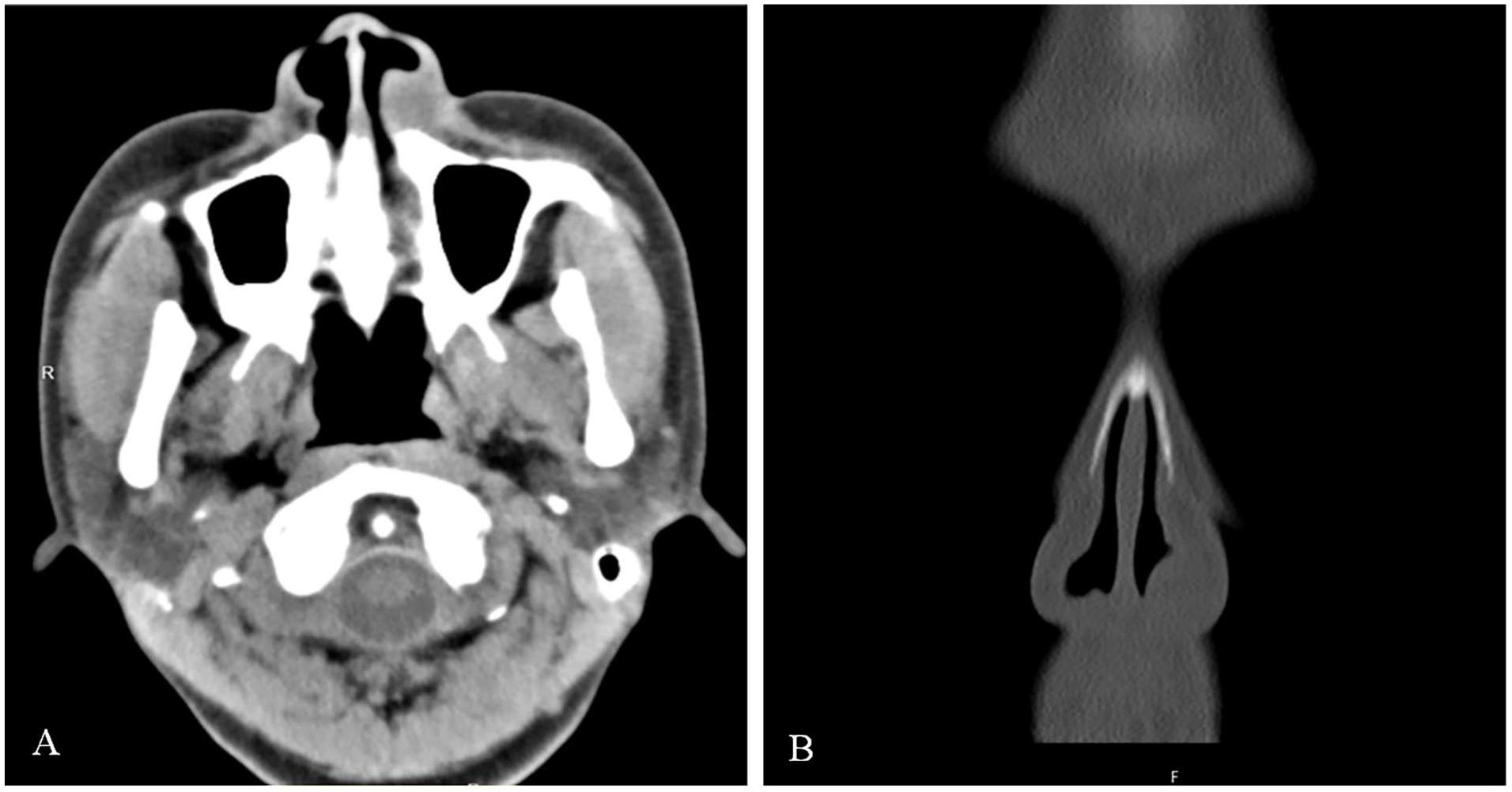
Axial (A) and coronal (B) computed tomography scan of the paranasal sinus revealed well-defined heterogeneous enhancing soft tissue mass arising from the left nasal vestibule.
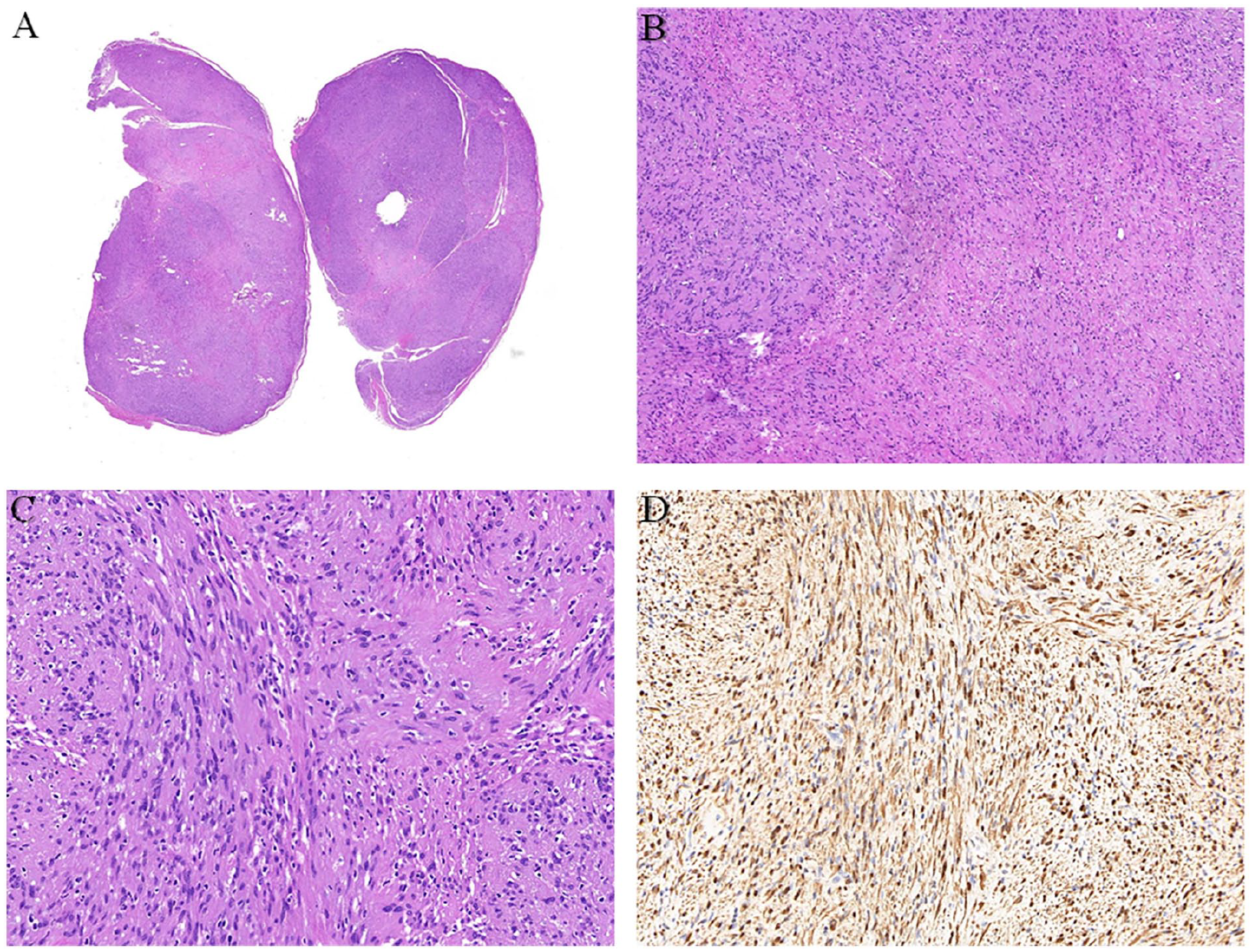
(A) Hematoxylin-eosin staining (×4 magnification). (B) Hematoxylin-eosin staining of the mass showing remarkable features of neurilemmoma consisting of Antoni A and Antoni B areas (×40 magnification). (C) Hematoxylin-eosin staining showing numerous cellular spindle cells form palisade structure (×100 magnification). (D) The mass cells expressed strong reactivity for S100 (×100 magnification).
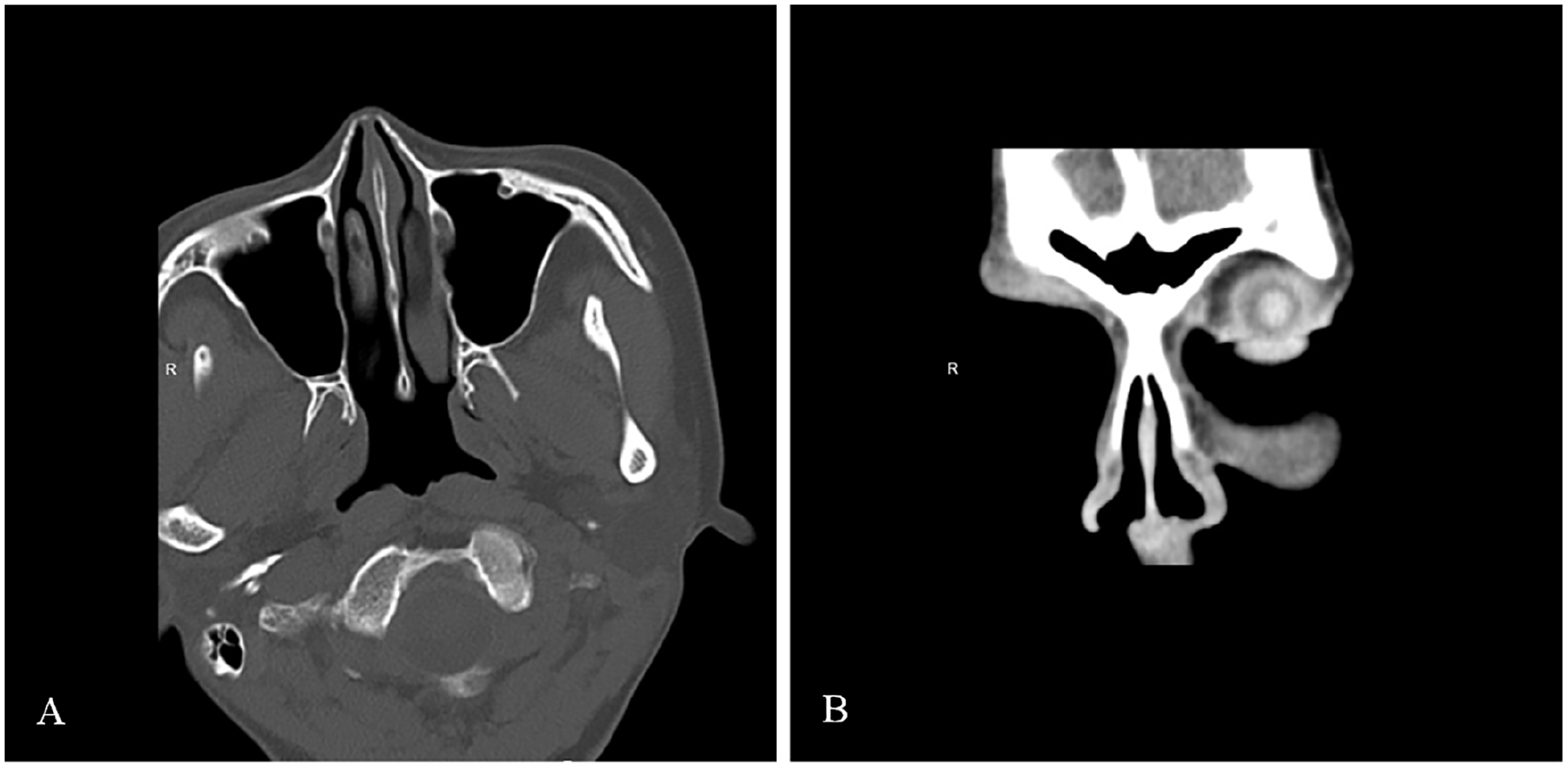
Postoperative axial (A) and coronal (B) computed tomography scan of the paranasal sinus showed complete resection of the left nasal vestibule mass without recurrence.
Discussion
The majority of neurilemmoma occurred in patients aged 20 to 60 years, with equal frequency in either sex. 8 Most of them are solitary. 9 A typical feature of it in the head and neck is the clear capsule, except for tumors in the nose and paranasal sinuses. 8 Neurilemmomas are rare (<4%) in the nasal cavity, paranasal sinuses, and pterygopalatine fossa. 10 Nasal septum is the most commonly affected portion of neurilemmoma in the nasal cavity and paranasal sinus. 11 Min et al reviewed literature since 2000 and 18 cases of nasal septum neurilemmoma reported in the English literature were found. 12 In 2016, solitary nasal tip neurilemmoma have been found reported in 4 cases. 9 There are currently few relevant English literature on nasal vestibule neurilemmomas since they are essentially uncommon. The vagus nerve is the most common origin of head and neck neurilemmomas. 3 When tumors occur in the paranasal sinuses, the origin nerve is postulated to be the peripheral nerve sheaths of the ophthalmic and maxillary branches of the trigeminal nerves. 13 Anterior ethmoid nerve and nasopalatine nerve are the origin of nasal septal neurilemmoma. 14 For the lateral nasal wall, it may be dominated by the posterior superior and inferior lateral nasal branches of the maxillary nerve. 15 In addition, nasal vestibule neurilemmomas may originate from these nerves. There are several other diseases included in the differential diagnosis of nasal vestibule neurilemmoma, including abscess, fibroma, inverted papilloma, pleomorphic adenoma, lipoma, hemangioma, melanoma, olfactory neuroblastoma, granuloma, polyps, and mucocele.9,11,10,16 Infectious diseases, benign and malignant tumors, and other pathologic conditions may occur in the nasal vestibule. Although rare, nasal neurilemmomas also have the malignancy potential about 2%.14,17 The benign tumors have a favorable prognosis and no recurrence, while malignant transformations cases have also been reported, which may show lytic lesions and invasion.3,13 The symptoms of nasal neurilemmoma can be progressively unilateral nasal obstruction and bulging, painful sensation, mucopurulent discharge, nasal swelling, anosmia, and intermittent epistaxis, which were determined by the location and size of the neoplasm.11,18,19 The most typical complaints were unilateral nasal congestion, which is nonspecific and can be observed in many other benign tumors, some patients even without notable symptoms.10,19-21 Nasal vestibule neurilemmoma can cause localized facial hypesthesia or paresthesia due to nerve compression.16,22
A well-defined contrast-enhanced homogenous soft tissue density mass is the most common CT manifestation of nasal neurilemmoma, However, on CT alone, it may be difficult to distinguish neurilemmoma from inflammation or other tumors.11,14 Magnetic resonance imaging (MRI) findings can help with preoperative parent nerve assessment. 3 And on T2-weighted MRI, nasal neurilemmomas are isointense with the brainstem, with lower signal intensity than neurilemmomas from other parts of the body, presumably because nasal neurilemmomas show more cellular characteristics. 15 Although nasal neurilemmoma is uncommon and imaging features are nonspecific, CT and MRI scans are beneficial for detecting the area of tumor extension and bony destruction, which are valuable for preoperative diagnosis and surgical planning.15,19
The gold standard for accurate neurilemmoma diagnosis is histopathological examination, which revealed 2 distinct histologic patterns of Antoni A and Antoni B.11,19 Antoni A has a high cell density region with spindle-shaped cells and tightly arranged nuclear palisade tissue termed Verocay bodies.16,19 Antoni B type only has a few cells, contains a loose stroma with no obvious pattern.3,19 However, if no diagnostic histological characteristics of neurilemmoma are present, immunohistochemistry staining of S-100 protein may be useful. 12 But it can also be positive in neurofibromas, melanomas, as well as myoepithelial tumors, making it nonspecific indicators for nasal neurilemmoma. 23 Neurilemmoma should be considered in the differential diagnosis of nasal vestibule masses. It frequently manifests as a whitish-yellow, circumscribed lesion. 3 Their endoscopic appearance does not like traditional polyp tissue. 13 However, nasal vestibular neurilemmoma is uncommon, it is easily mistaken as a nasal vestibular cyst.
It is radioresistant, and chemotherapy is ineffective, complete excision is the preferred and curative treatment, which has a high success and low recurrence rate.11,18,22 The surgical approach is determined by the size, position, and invasion of adjacent structures of the tumor, it is vital to preserve as much of the major nerve as possible.3,20 Transnasal endoscopic surgery may be the most suitable approach.12,14 For patients with malignant neurilemmoma, to completely remove the tumor, simultaneous nerve resection and postoperative radiotherapy are required. 24 Preoperative biopsy is a strategy to exclude the malignant tumor lesions, although it is one protocol and not a guideline. 21 We need a follow-up period after the surgery to confirm the recurrence of tumor. After complete excision of a benign nasal neurilemmoma, postoperative recurrence is uncommon. 15 Due to the anatomical characteristics of the nasal vestibule, the diagnosis and treatment of nasal vestibular masses are often frequently difficult. This case improves the understanding of nasal neurilemmoma and adds nasal neurilemmoma included in the differential diagnosis for cystic lesions in this region.
Footnotes
Acknowledgements
The authors are grateful to the support from the Key Support Project of Jiaxing (no. 2023-FC-004). We would like to thank all reviewers and editors for their professional review work, constructive comments, and valuable suggestions on our article. Yi Zhou wrote the article and prepared figures, Yao Sun participated in the guidance and revision of the article. All authors were involved in editing and agree to the published version of the article. Thank all authors for their hard work.
Data Availability
Data and materials can be obtained from the corresponding authors on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant from the Key Support Project of Jiaxing (no. 2023-FC-004).
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for anonymized information to be published in this article.