
Abstract
Importance
Lingual thyroglossal duct cysts (LTGDCs) are rare congenital anomalies that necessitate proactive surgical intervention due to their potential for life-threatening airway obstruction. The challenging anatomical location of LTGDCs complicates their surgical management, and there are currently no standardized surgical modalities in place.
Objective
To analyze the clinical features of LTGDCs and evaluate the feasibility, safety, and efficacy of coblation-assisted transoral endoscopic excision of LTGDCs.
Design
Retrospective case series (2009-2022) analyzing preoperative, intraoperative, and postoperative data.
Setting
Tertiary academic center.
Participants
Twenty-nine patients (20 males, 9 females; ages 3-70, with a median age of 34 years) were diagnosed with LTGDCs, including 7 (24.1%) with recurrent LTGDCs following prior surgeries at other institutions.
Intervention
Coblation-assisted transoral endoscopic excision of LTGDC using FK retractors and a 30° Hopkins telescope for optimal visualization and manipulation.
Main Outcome Measures
Complete cyst excision, postoperative recovery, recurrence rates, complications, and surgical feasibility.
Results
All LTGDCs were completely excised. During the procedure, it was found that the LTGDCs abutted but did not adhere to the hyoid bone, which allowed for their dissection from the periosteum of the hyoid bone using coblation. Postoperative recovery was uneventful, with an average postoperative stay of 3.1 days (range 1-5 days). No complications, such as bleeding, infection, or airway obstruction, occurred. The mean follow-up period was 5.3 years (range 6 months to 12.4 years), with no recurrences observed during this time.
Conclusions
Coblation-assisted transoral endoscopic excision is a reliable, effective, and minimally invasive approach for managing LTGDCs. It ensures complete removal with low recurrence and complication rates, aided by superior visualization and manipulation space provided by FK retractors and a 30° Hopkins telescope.
Relevance
This technique offers a safe alternative to traditional surgeries, reducing trauma and enhancing recovery. Future studies should explore comparisons with other surgical modalities to validate their broader applicability.

Introduction
Thyroglossal duct cysts (TGDCs), the most common congenital midline neck masses, originate from remnants of the thyroglossal duct that do not completely disappear during the descent of the thyroid gland in the fetal period. 1 They can occur at any location from the foramen cecum of the tongue to the thyroid gland, encompassing the thyroglossal region, the suprahyoid region, the suprasternal fossa, and the tongue base. 2 Most TGDCs arise between the hyoid bone and the thyroid cartilage, whereas lingual TGDCs (LTGDCs), located at the tongue base, are a rare variant of this disease, representing approximately 2% to 8.5% of all TGDCs.3 -5
The typical clinical manifestations of LTGDCs differ from those of TGDCs found in other locations, including symptoms such as airway obstruction, dysphagia, and even sudden infant death.6 -8 Surgical excision is effective for LTGDCs. However, due to its difficult-to-access anatomical location, exposing and completely excising LTGDCs presents a significant challenge. Currently, reports on the surgical management of LTGDCs are limited, and standardized surgical modalities have yet to be established. The Sistrunk procedure has traditionally been the most commonly used surgical technique for managing TGDCs. 9 Nonetheless, excising LTGDCs along with the central hyoid bone via a neck approach not only results in considerable trauma but also, due to the deep-seated location of the cysts, increases the difficulty of complete excision. In recent years, several studies have shown the feasibility of transoral endoscopic excision for LTGDCs, including cystectomy and marsupialization.5,10 -13
Since 2009, coblation-assisted transoral endoscopic excision of LTGDC using FK retractors alongside a 30° Hopkins telescope has been utilized for treating LTGDCs at the study institution, demonstrating favorable outcomes. This retrospective study was conducted to assess the feasibility, safety, and efficacy of coblation-assisted transoral endoscopic excision of LTGDCs and analyze the advantages of this surgical technique.
Methods
Study Subjects
A total of 29 patients diagnosed with LTGDCs via pathological examination and undergoing coblation-assisted transoral endoscopic surgery between January 2009 and December 2022 were retrospectively analyzed. Demographic data, symptoms, imaging findings, surgical procedures, and clinical outcomes were collected from the case records. The study was approved by the Ethics Committee of Peking Union Medical College Hospital (Ethics number: I-24PJ0568).
Preoperative Workup
The preoperative evaluation included flexible laryngoscopy, cervical computed tomography (CT), and/or magnetic resonance imaging (MRI). These examinations aided in determining the location and extent of the cyst, clarifying the relationship between the cyst and the hyoid bone, and confirming the presence of the cervical thyroid gland.
Operative Technique
All patients underwent coblation-assisted transoral endoscopic excision of LTGDCs under general anesthesia.
Intubation and positioning
Intubation was performed transorally or transnasally under video laryngoscopy, with a preference for nasotracheal intubation. After intubation, the patient was positioned supine with the head extended.
Exposure
Exposure of the base of the tongue, vallecula, and epiglottis was achieved using FK retractors secured by a stand, while visualization was provided with the aid of an assistant employing a 30° Hopkins telescope.
LTGDC excision
For cysts that were too large, some cystic fluid was suctioned in advance to decompress the cyst. The cyst wall was grasped by a laryngeal micro-grasper to delineate the boundary and maintain a certain tension. Coblation, a temperature-controlled plasma radiofrequency (EIC5874-01; Smith & Nephew, Austin, TX, USA), was utilized to excise the cyst along its boundary to the depth of the hyoid bone. If necessary, an assistant could press the body of the hyoid bone in a posterior and upward direction from the anterior neck. This maneuver helped to displace the hyoid bone into the transoral field, thereby better exposing the deep part of the cyst wall. Care was taken to ensure complete removal of the cyst. Hemostasis was primarily achieved using coblation. A suction coagulator was utilized as needed to help manage arterial bleeding effectively. In recurrent cases, extended excision was performed on the cyst wall and previous surgical scars.
After excision, the cavity was meticulously examined with a Hopkins telescope. Any suspected residual cyst tissue was precisely ablated with coblation to prevent recurrence. The wound at the base of the tongue was left open to epithelialization. The decision to extubate immediately after the operation depended on the degree of swelling at the base of the tongue observed at the end of the surgery.
Results
The demographic data, disease characteristics, and treatment details of the enrolled patients are presented in Table 1.
The Characteristics of the Enrolled Patients.
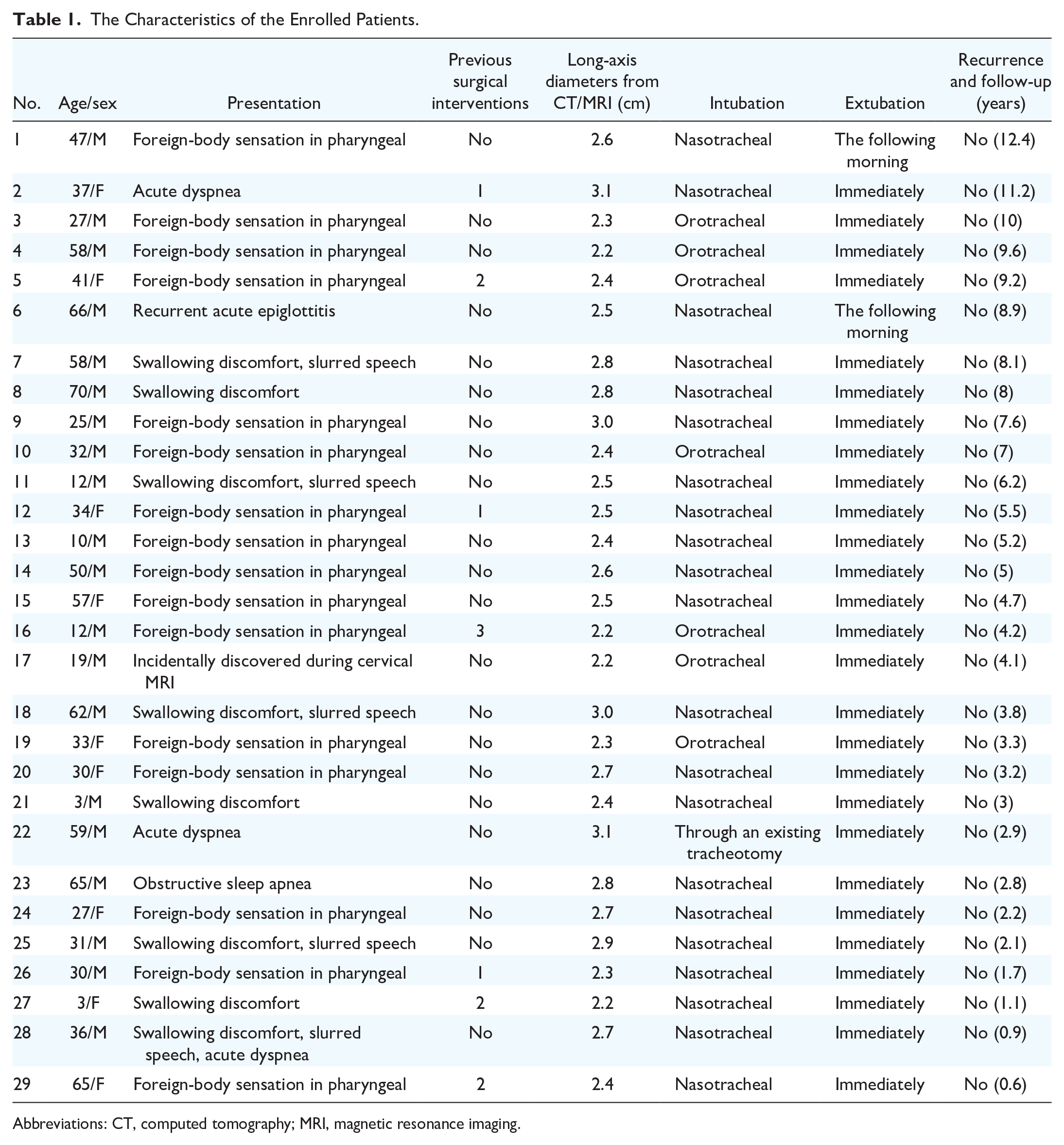
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging.
General Information
Among the 29 patients with LTGDCs, 20 (69.0%) were males, and 9 (31.0%) were females. The patients’ ages ranged from 3 to 70 years, with a median age of 34 years. Five patients were under the age of 14 years.
Clinical Presentation
Among all patients, 16 (55.2%) complained of pharyngeal foreign-body sensation. Eight (27.6%) experienced swallowing discomfort (odynophagia or swallowing obstruction), including 4 (13.8%) with slurred speech. Three patients (10.3%) reported acute dyspnea, with one requiring emergency tracheotomy. In addition, 1 patient (3.4%) presented with recurrent acute epiglottitis, another (3.4%) had obstructive sleep apnea, and 1 (3.4%) LTGDC was incidentally discovered during cervical MRI for another indication. Seven patients (24.1%) were referred to our hospital due to recurrent cysts at the tongue base following prior endoscopic marsupialization or cystectomy in other hospitals. The duration of the illness ranged from 0.5 to 36 months, with a mean of 4 months.
Preoperative Assessment
During flexible laryngoscopy, an LTGDC typically appears as a round, dark brown, cyst-like mass, with a thick wall located in the posterior region of the tongue, either at the midline or unilaterally. Larger cysts may compress the epiglottis toward the posterior pharyngeal wall (Figure 1).

A flexible laryngoscopic view of an LTGDC. A large cyst at the base of the tongue compressing the epiglottis toward the posterior pharyngeal wall. LTGDC, lingual thyroglossal duct cyst.
The presentation of LTGDCs on CT is a low-density cystic lesion located at the posterior tongue. On MRI, it appears hypointense on T1-weighted imaging and hyperintense on T2-weighted imaging. Sagittal views on both CT and MRI demonstrated a cystic mass at the base of the tongue, posterior to the foramen cecum and adjacent to the hyoid bone. CT and/or MRI can assist in determining the depth of the cyst’s root within the tongue base (Figures 2 and 3). The long-axis diameters of the cysts ranged from 2.2 to 3.1 cm.
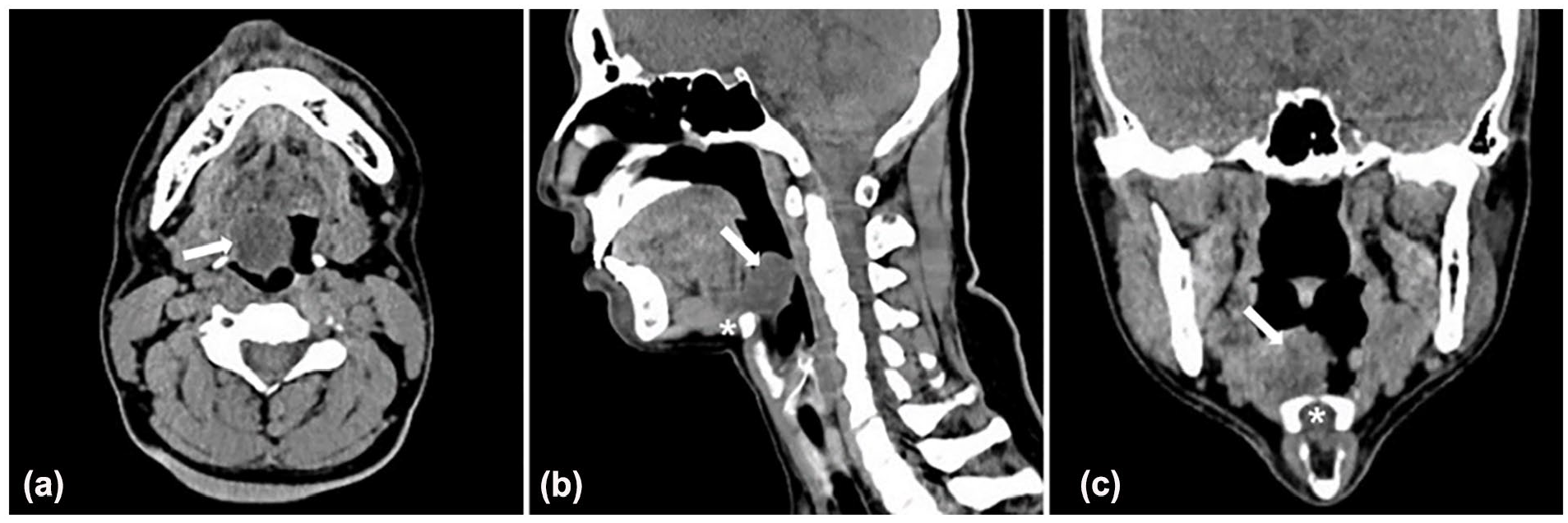
CT findings for LTGDCs. (a) Axial CT image showing a cyst (arrow) at the base of the tongue. (b) Sagittal CT image displaying a cyst (arrow) posterior to the foramen cecum, adjacent to the hyoid bone (asterisk). (c) Coronal CT image illustrating a cyst (arrow) at the base of the tongue, abutting the hyoid bone (asterisk). CT, computed tomography; LTGDC, lingual thyroglossal duct cyst.
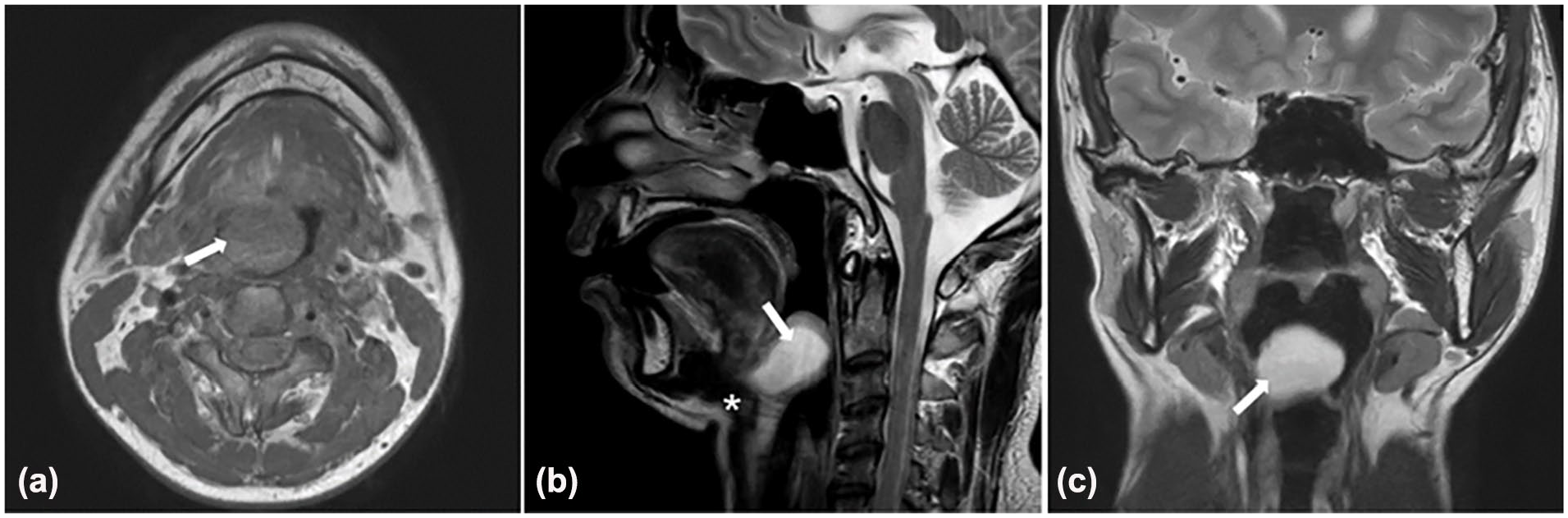
MRI findings for LTGDCs. (a) Axial MRI displaying a cyst (arrow) at the base of the tongue, which appears hypointense on a T1-weighted sequence. (b) Sagittal MRI showing a cyst (arrow) closely adjacent to the hyoid bone (asterisk). (c) Coronal MRI illustrating a cyst (arrow) at the base of the tongue, appearing hyperintense on a T2-weighted sequence. LTGDC, lingual thyroglossal duct cyst; MRI, magnetic resonance imaging.
Operative Findings
Of the 29 patients, 21 patients (72.4%) received general anesthesia via nasotracheal intubation, 7 (24.1%) via orotracheal intubation, and 1 (3.4%) via intubation through an existing tracheotomy. During the operation, normal tongue base tissue and the cyst were readily differentiated under magnification with a Hopkins telescope. We observed that the cysts abutted but did not adhere to the hyoid bone. The hyoid bone could be palpated with coblation, and the cyst could be dissected from the periosteum of the hyoid bone (Figure 4). Bleeding was minimal and easily controlled with coblation. A suction coagulator was occasionally used for uncontrollable vascular bleeding.

Endoscopic image following the removal of an LTGDC. The body of the hyoid bone (arrow) and the greater horn of the hyoid bone (asterisk) are identifiable. LTGDC, lingual thyroglossal duct cyst.
Postoperative Course
Twenty-seven patients (93.1%) were extubated immediately after surgery. Two patients (6.9%) remained intubated in the intensive care unit overnight for airway protection and were extubated the following morning. Perioperative antibiotics were administered for 5 days to prevent infection. Pain was minor, and no analgesics were required. No immediate postoperative complications, such as airway obstruction, bleeding, or infection, were observed in any of the patients. Patients were placed on a liquid diet for 3 days followed by soft food for 2 to 3 weeks postoperatively. The duration of hospitalization for observation postoperation ranged from 1 to 5 days, with an average of 3.1 days.
Flexible laryngoscopy was usually performed 2 weeks after surgery to assess the development of pseudomembranes in the wound (Figure 5). Typically, the surgical wound was replaced by normal mucosa within 3 to 4 weeks postoperation.

Flexible laryngoscopic image acquired at 2 weeks post-surgery. The pseudomembrane showed satisfactory growth on the wound surface.
Postoperative Pathology
The postoperative pathological results of all the patients indicated that the excised cyst wall tissue was lined with epithelium, often respiratory epithelium, including non-keratinized stratified squamous epithelium, and/or simple squamous epithelium, and/or pseudostratified ciliated columnar epithelium. Partially observed were minor salivary glands and skeletal muscle tissue. These characteristics were consistent with LTGDCs.
Follow-Up
The 29 patients with LTGDCs were followed up for 6 months to 12.4 years, with a mean of 5.3 years. No recurrences were observed during the postoperative follow-up period. Symptoms related to LTGDCs significantly improved in all patients. No long-term complications, such as tongue movement disorders, dysgeusia, dysphonia, or dysphagia, were detected throughout the follow-up period.
Discussion
LTGDCs are a rare congenital anomaly that can occur in both children and adults. Among the patients included in this study, there were 24 adults and 5 children. While some LTGDCs may be discovered incidentally, many patients experience clinical symptoms, including sensation of a foreign body in the throat, swallowing discomfort, dysphonia, sleep-related issues, and, in severe cases, life-threatening dyspnea, or even asphyxia. Hemorrhage or infection of LTGDCs can also lead to sudden pain or obstruction symptoms.14,15 In our study, the majority of patients presented with pharyngeal foreign-body sensation, while 3 patients sought medical attention for dyspnea, with one undergoing emergency tracheostomy. This indicates that regardless of whether patients with LTGDCs are symptomatic or not, early surgical excision is recommended to prevent sudden volume expansion of the cysts caused by acute inflammation, which may lead to urgent airway obstruction. When patients with LTGDCs encounter acute upper airway obstruction, preparing for intubation or tracheotomy is imperative. In addition, suctioning cystic fluid to reduce the size of the cyst is also a method of alleviating dyspnea.
Preoperatively, it is crucial to ascertain the precise diagnosis of LTGDCs and thoroughly evaluate the extent of the cysts. Flexible laryngoscopy serves as the primary diagnostic tool for these patients. Further confirmation of the morphology and extent of the cyst, as well as its relationship with the hyoid bone, can be achieved through imaging examinations. Both CT and MRI examinations provide more detailed anatomical information for the cyst at the base of the tongue. In a sagittal view, a cyst located posterior to the foramen cecum and abutting the hyoid bone is the most valuable imaging feature for diagnosing LTGDCs. These characteristics facilitate the differentiation of LTGDCs from simple vallecular cysts and other lesions originating from the base of the tongue, enabling clinicians to better prepare for the surgery.
The surgical approaches for LTGDCs include the traditional Sistrunk procedure, the more conservative procedure of marsupialization, and several techniques of transoral endoscopic resection.10,16 -18 The Sistrunk procedure, aimed at removing the cyst, duct, and central hyoid bone via open surgical access to minimize recurrence rates, may result in unnecessary trauma and subsequent potential complications. Due to the absence of ducts in LTGDCs 4 and the considerable distance between the tongue base and the cervical incision site, some investigators have proposed the utilization of transoral surgical approaches. Marsupialization under endoscopy is a relatively minimally invasive procedure;10,16 however, it may leave residual cyst tissue at the base of the tongue. Recurrences have often been reported in such cases.17,19 To minimize recurrence, some investigators suggest complete removal of all pathologic tissues. Several endoscopic cystectomy techniques for LTGDCs, including electrocautery, microelectrodes, lasers, and coblation, have been described in previous studies.5,11,19,20 In the present study, 29 patients underwent coblation-assisted transoral endoscopic cystectomy using FK retractors alongside a 30° Hopkins telescope, which is a novel approach never reported before.
The challenge of transoral surgery arises from the constrained visual field and the limited operating space. When operating within such confined spaces, sufficient exposure to the surgical field and improved working area are prerequisites for the complete excision of the cyst. In terms of anesthetic intubation, nasotracheal intubation was preferred, as it allows for maximum exposure of the operative field, making surgical manipulation convenient. For exposing the operative field, FK retractors can provide a superior field of view and a larger working space for precise procedures. The 30° Hopkins telescope, which can be adjusted to a wide range of angles, offers a comprehensive field of view and excellent magnification for visualization. In this study, we found that pressing the hyoid bone from the neck to displace it into the transoral field helps to better expose the deep root of the cyst. The aforementioned recommendations can assist in achieving an optimal surgical field, ensuring the best visualization, facilitating precise maneuvers, and ultimately enabling complete excision of the cyst.
Coblation, temperature-controlled plasma radiofrequency, is a relatively new technique that was first introduced in otolaryngology for tonsillectomy. It integrates multiple functions, including ablation, cutting, hemostasis, suction, and irrigation with saline. The design of an angled cutting head makes it easier to reach the surgical site and enables manipulation with exceptional flexibility and accuracy. With the assistance of a 30° Hopkins telescope, coblation can target lesions located in relatively “hidden” positions. Compared with other common techniques used for these procedures, such as electrical cautery or lasers, coblation offers superior efficiency in tissue cutting and hemostasis. 20 Additionally, coblation works at a lower temperature (typically 40°C-70°C), 21 which could minimize thermal damage to the surrounding tissues and thereby alleviate postoperative pain. Due to these advantages, the utilization of coblation helps maintain a clear surgical field, enhance the precision of maneuvers, reduce the operation duration, and shorten the recovery time. Thus, we suggest coblation as an ideal tool for excising LTGDCs.
Complete excision of the cyst, especially the epithelium around the hyoid bone, is crucial for preventing recurrence. In this study, all cysts were dissected from the hyoid periosteum and completely excised, with no recurrence. Zhang et al held that recurrence of LTGDCs was closely correlated with residual epithelium around the hyoid bone, and suggested that the Sistrunk procedure was needed for recurrent cases. 17 In this study, 7 recurrent LTGDCs were also completely excised using the mentioned surgical method, and no further surgeries were needed. In our view, the choice of surgical approach should take into account the patient’s prior surgical history, imaging results, exposure condition, and the patient’s preferences, rather than whether it is a recurrent case. However, in specific cases, such as a double cyst above and below the hyoid bone, though not encountered in this study, an open transcervical approach is recommended.
There have also been reports of transoral endoscopic excision of LTGDCs with coblation,20,22 but the operative field was exposed with microscopes and suspension laryngoscopes, which differ from the methods used in this study. Microscopes rely on a line of sight and suspension laryngoscopes have a smaller diameter with a tubular field of view, restricting the visualization of the operative field and manipulation space. Furthermore, these reports did not involve recurrent cases, which could potentially complicate the surgical procedure.
Other reports have suggested transoral robotic surgical excision of LTGDCs,12,23,24 which provides superior 3-dimensional visualization, a wide operating field, and increased precision and maneuverability in this difficult-to-access location. However, robotic surgery is costly, and surgeons require specialized training to perform it. As a result, its widespread adoption has been limited. Moreover, although the robotic system offers a high-definition 3D view, it lacks tactile feedback, which can be extremely useful in certain situations. 25
This study has several limitations. First, due to the rarity of LTGDCs, the sample size of this study is relatively small. Second, constrained by the retrospective nature of the study, data such as self-reported pain ratings were unavailable. Third, at the study institution, coblation is the primary method used for excising LTGDCs, lacking comparison with other surgical techniques.
Conclusions
With the benefits of FK retractors alongside a 30° Hopkins telescope, coblation-assisted transoral endoscopic excision of LTGDCs stands as a reliable, effective, and minimally invasive surgical method, with a reduced risk of complications or recurrence.
Footnotes
Acknowledgements
None.
Authors’ Contributions
Y.N. analyzed and interpreted data, drafted the article.
T.C. conducted data collection and data analysis. YN and TC contributed equally to this work.
W.L. interpreted the results.
X.J. collected data.
H.H. conceived and designed the study, edited the final version of the manuscript for publication.
J.W. conceived and designed the study, reviewed and critically revised the manuscript.
All authors read and approved the final manuscript.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent Statements
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Peking Union Medical College Hospital (Ethics number: I-24PJ0568).