
Abstract
Introduction
Maxillary sinus pathologies are commonly encountered in otolaryngology clinics’ daily practice. They are usually managed medically; however, surgery may be warranted, depending on the pathology’s nature and response to medical treatment.
Prior to the endoscopic era, Caldwell-Luc and inferior maxillary antrostomy (IMA) were commonly performed to address various maxillary sinus pathologies. 1 They provide sufficient access to the maxillary sinus and are relatively safe and easy to perform without requiring sophisticated technologies. However, they have some common complications. 2
Known complications after the Caldwell-Luc procedure are facial pain, numbness, and swelling. These complications can be transient or permanent. 1 IMA does not address natural and physiological mucociliary flow and could result in mucus recirculation between the natural ostium of the maxillary sinus and the IMA, with subsequent persistent postnasal drip (PND). Nasolacrimal duct (NLD) injury can also occur during IMA. 2 Such an injury is usually asymptomatic, but could lead to persistent epiphora that may require surgical intervention in some patients. Both procedures can lead to dental root injuries, which may require dental procedures in the future. With the introduction of endoscopic surgeries in the 1980s and the adoption of the concept of mucociliary transport of mucus to the natural ostium of the maxillary sinus, as Messerklinger described, the Caldwell-Luc and IMA approaches were gradually abandoned. 3
Currently, the main standard of care to surgically address various maxillary sinus pathologies is endoscopic middle meatal antrostomy (MMA). It provides optimal physiological drainage and sinus ventilation without disrupting the mucociliary flow. Orbital and nasolacrimal duct injuries, as well as the recirculation phenomenon, can be avoided by meticulous dissection and removal of the uncinate process to achieve adequate MMA that is continuous with the natural ostium. 4
Although endoscopic MMA is considered a safe, minimally invasive, and functional procedure, it does not provide full exposure to certain aspects of the maxillary sinus, such as alveolar, zygomatic, and prelacrimal recesses. 5 In these hidden maxillary sinus niches, endoscopic MMA alone may not allow sufficient access to address certain pathologies without leaving some residual disease that lead to recurrence. Therefore, for certain anatomically challenging pathologies in so-called difficult-to-access locations, an MMA combined with an IMA, Caldwell-Luc procedure, and/or prelacrimal approach may be warranted. 6 Combined approaches yield better access and facilitate the complete eradication of such pathologies, but involve known possible complications.
In this retrospective chart review, we describe and review our experience with our modified inferior antrostomy technique—submucosal temporary inferior maxillary antrostomy (STIMA)—to address lesions in difficult-to-access locations in 18 patients. In such situations, STIMA improves visualization and accessibility (as described in our published cadaveric study 5 ) and would decrease the incidence of the known complications of conventional IMA, including NLD injury and the recirculation phenomenon, with its persistent PND.
Objectives
To describe our modified IMA, STIMA.
To review different diagnoses, we encounter in difficult-to-access locations and STIMA indications.
To report maxillary sinus disease outcomes and postoperative complications.
To report the incidence of neural, orbital, lacrimal, and/or dental injuries.
To report our temporary flap’s adequacy and viability, as well as the incidence of persistent antrostomy.
Methodology
Study Design
This is a retrospective chart review of patients who underwent functional endoscopic sinus surgery (FESS) and required our STIMA.
Study Population
Inclusion criteria
Adult patients who underwent elective FESS.
The presence of a lesion or pathology in a difficult-to-access location that is inaccessible by MMA alone.
The operating surgeon deemed a combined approach necessary, which would require a conventional IMA.
STIMA was performed as a less-invasive option than conventional IMA.
Exclusion criteria
Patients who did not have a follow-up for at least 2 months after surgery.
Patients with charts lacking the required documentation about complications, STIMA indication, and/or mucosal flap status.
Study Setting
The study was conducted in a tertiary hospital in Riyadh, Saudi Arabia, between January 1, 2020, and July 1, 2023. All procedures were performed by the same consultant surgeon—a fellowship-trained rhinologist.
Ethical Considerations
An approval letter was obtained from the Institutional Review Board. All data are managed confidentially and for research purposes only. Preoperative written informed consent was obtained from all patients undergoing FESS.
Surgical Technique
The procedure is performed while the patient is under general anesthesia. Once the decision to perform STIMA is made, the anterior part of the nasal floor and the anterior part of the lateral wall of the inferior meatus are injected with approximately 1 to 2 ml of a mixture of 1% lidocaine and 1:100.000 adrenaline to achieve better hemostasis. Then, a curvilinear mucosal incision is made to elevate a mucosal flap. The incision starts at the axilla of the inferior turbinate and extends inferiorly to the nasal floor. Then, it continues medially just posterior to the nasal sill to the nasal spine. Submucosal plane dissection is performed to elevate the mucosal flap and expose the bones of the nasal floor and the lateral wall of the inferior meatus. In this way, the Hasner’s valve and the distal end of the NLD are secured, as they are elevated with the mucosal flap. The bone of the lateral wall of the inferior meatus is punctured using a J-curette or curved suction cannula to perform the submucosal IMA. The antrostomy is then widened to 15 to 20 mm using a combination of ethmoid forceps, backbiting forceps, and/or microdebrider as needed. The pathology is addressed through both the inferior and middle maxillary antrostomies. Then, the mucosal flap is redraped to close the IMA. An absorbable dressing is applied to the inferior meatus to maintain the flap in a favorable position; sutures are not required (see Figure 1).
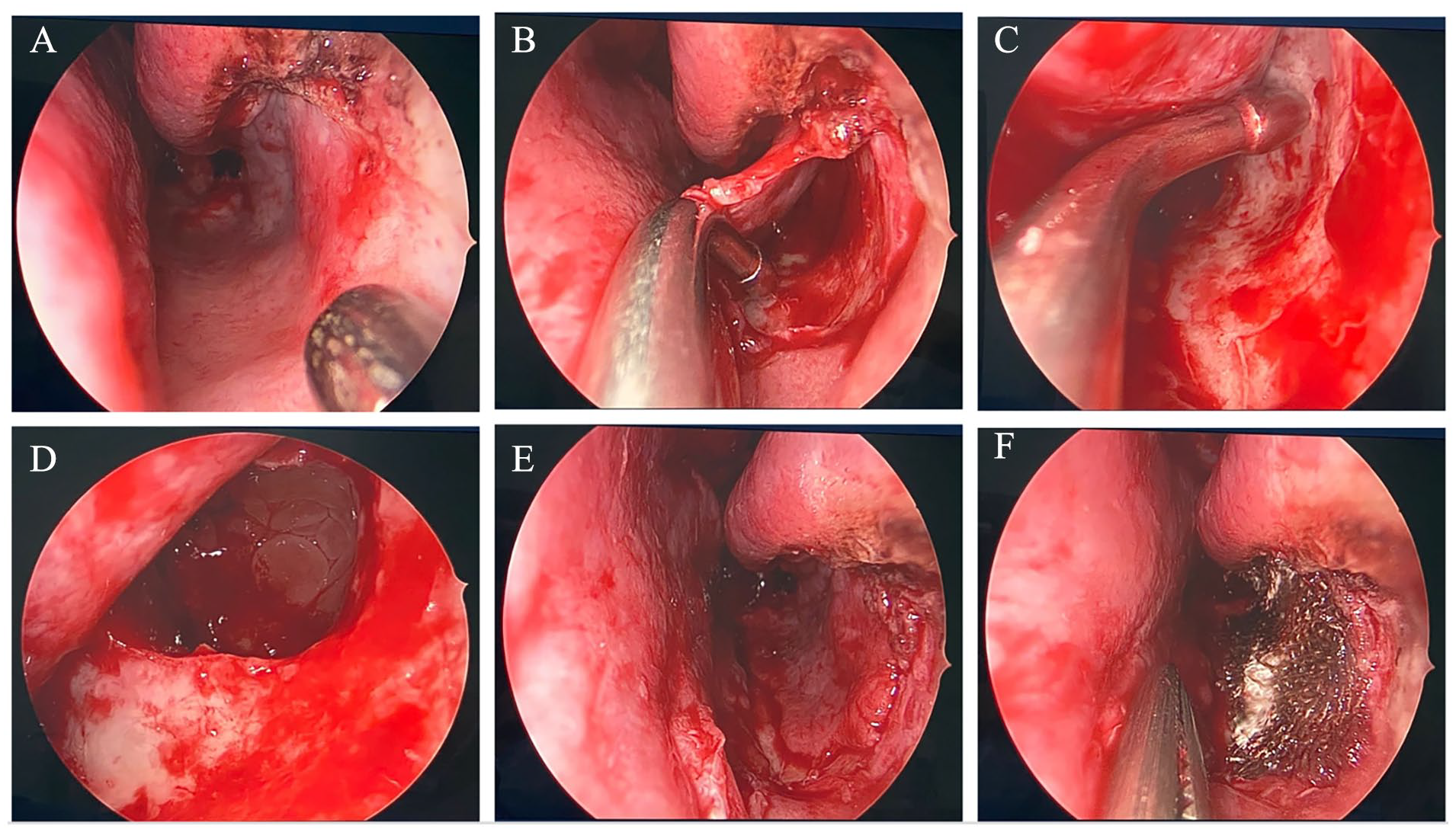
STIMA technique: (A) Site of incision. (B) Submucosal flap. (C) Submucosal antrostomy. (D) After widening the submucosal antrostomy. (E) After draping the mucosa. (F) Flap secured with absorbable packing. STIMA, submucosal temporary inferior maxillary antrostomy.
To promote a healthy flap and adequate closure in a relaxed manner, the curvilinear incision is made as anterior as possible to allow for a longer flap. A meticulous dissection of the mucosal flap has to be made to avoid mucosal tears, and the bony antrostomy is limited anteriorly, unless necessary.
To increase flap mobility, the incision may be extended posteriorly at the junction between the nasal septum and the nasal floor over the hard palate.
All patients are given postoperative paracetamol for analgesia and saline nasal sprays. If deemed necessary, some also received oral antibiotics.
Results
During the study period, 20 patients met the inclusion criteria. All patients for whom STIMA was considered and attempted were included in this review; however, 2 patients lacked sufficient follow-up visits over at least 2 months, so they were excluded. All patients had sufficient preoperative, intraoperative, and postoperative documentation.
The study included 13 males and 5 females with a mean age of 33 years and an age range between 18 and 60 years. STIMA was performed on the left side more often than on the right side, and 3 patients underwent bilateral STIMA (see Figure 2).
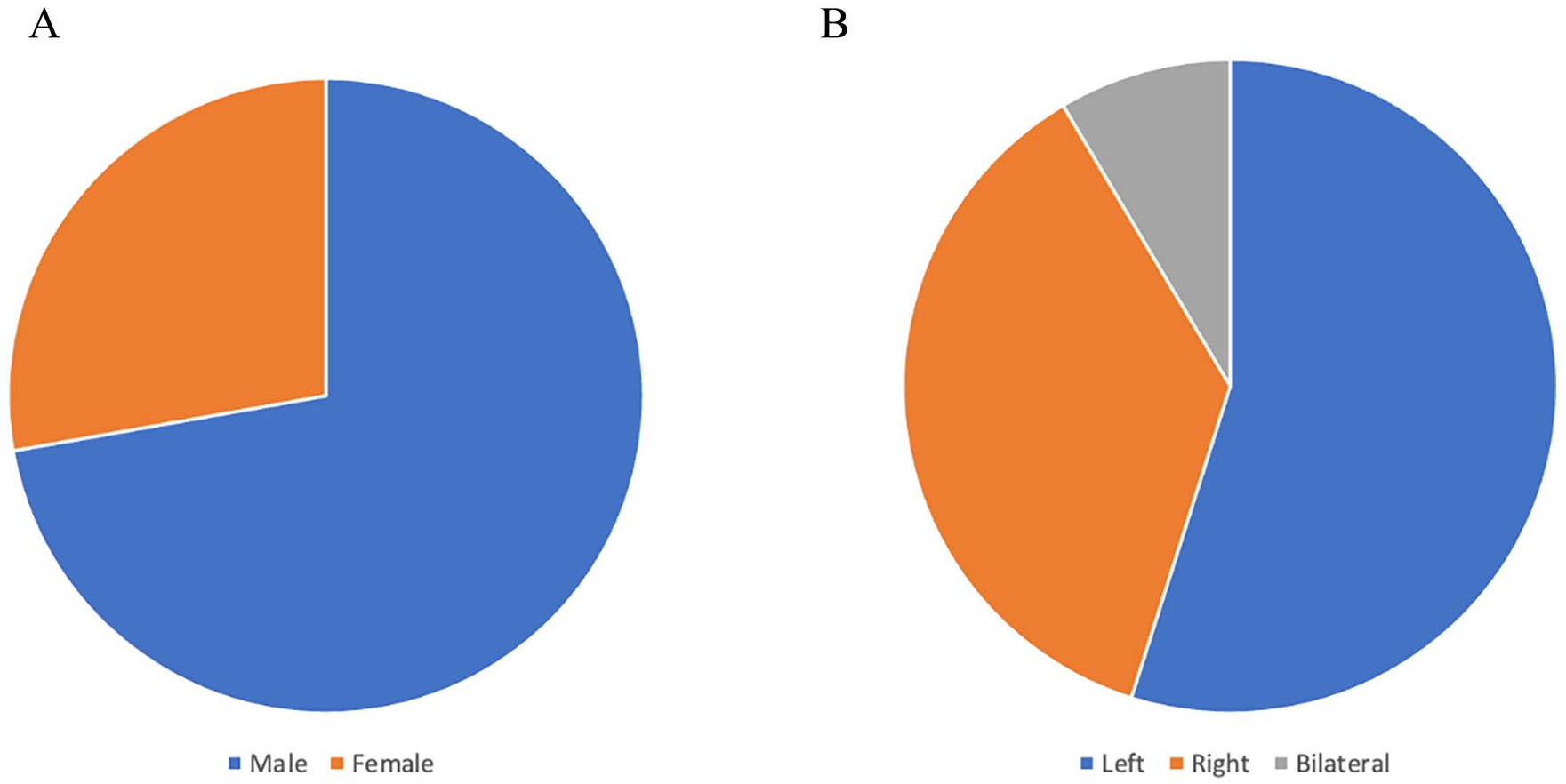
Characteristics of patients: (A) Gender. (B) Side of flap.
The most common diagnosis was chronic rhinosinusitis. The operating surgeon variously considered the anterior/inferior, posterior/medial, and floor of the maxillary sinus areas difficult-to-access intraoperatively. Each patient’s diagnosis, disease area, and STIMA indication are summarized in Table 1.
Summary of Diagnosis, Area of Disease, and Indications of IMA.
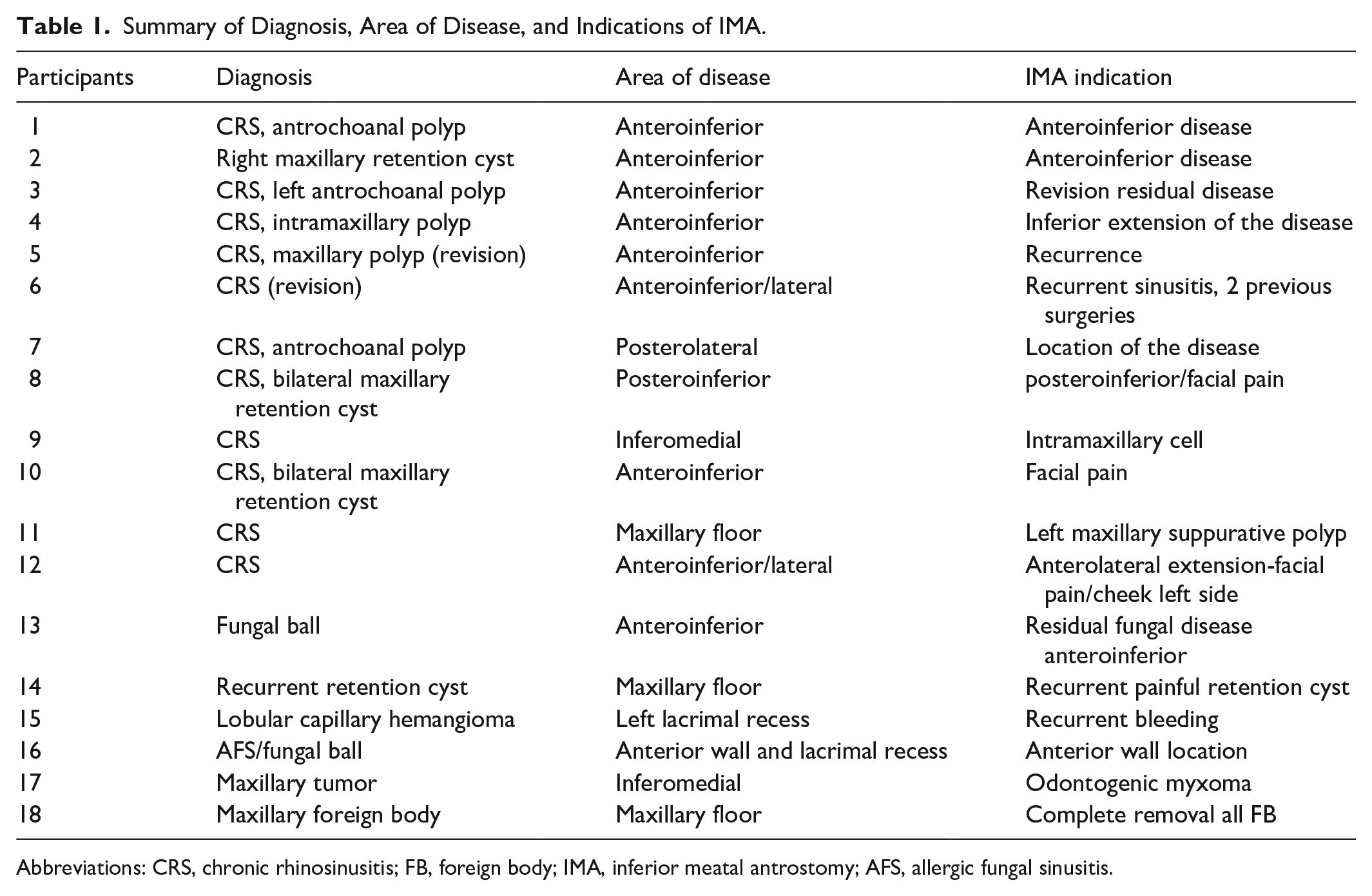
Abbreviations: CRS, chronic rhinosinusitis; FB, foreign body; IMA, inferior meatal antrostomy; AFS, allergic fungal sinusitis.
Postoperative assessments, such as disease outcomes, the presence of possible complications, and flap outcomes, were observed and documented in all patient charts. The average follow-up duration was 6 months, with a minimum follow-up duration of 3 months; the longest was 2 years (see Table 1).
The maxillary sinus mucosa outcomes were healthy in all patients, except for 4 with polypoidal mucosa. However, none of the 18 patients reported postoperative complications, except for 1 with postoperative bleeding from the contralateral side, which did not affect the STIMA outcome. No neural, orbital, lacrimal, or dental complications were reported in any of the patients (see Table 2).
Summary of Postoperative Complications of STIMA.
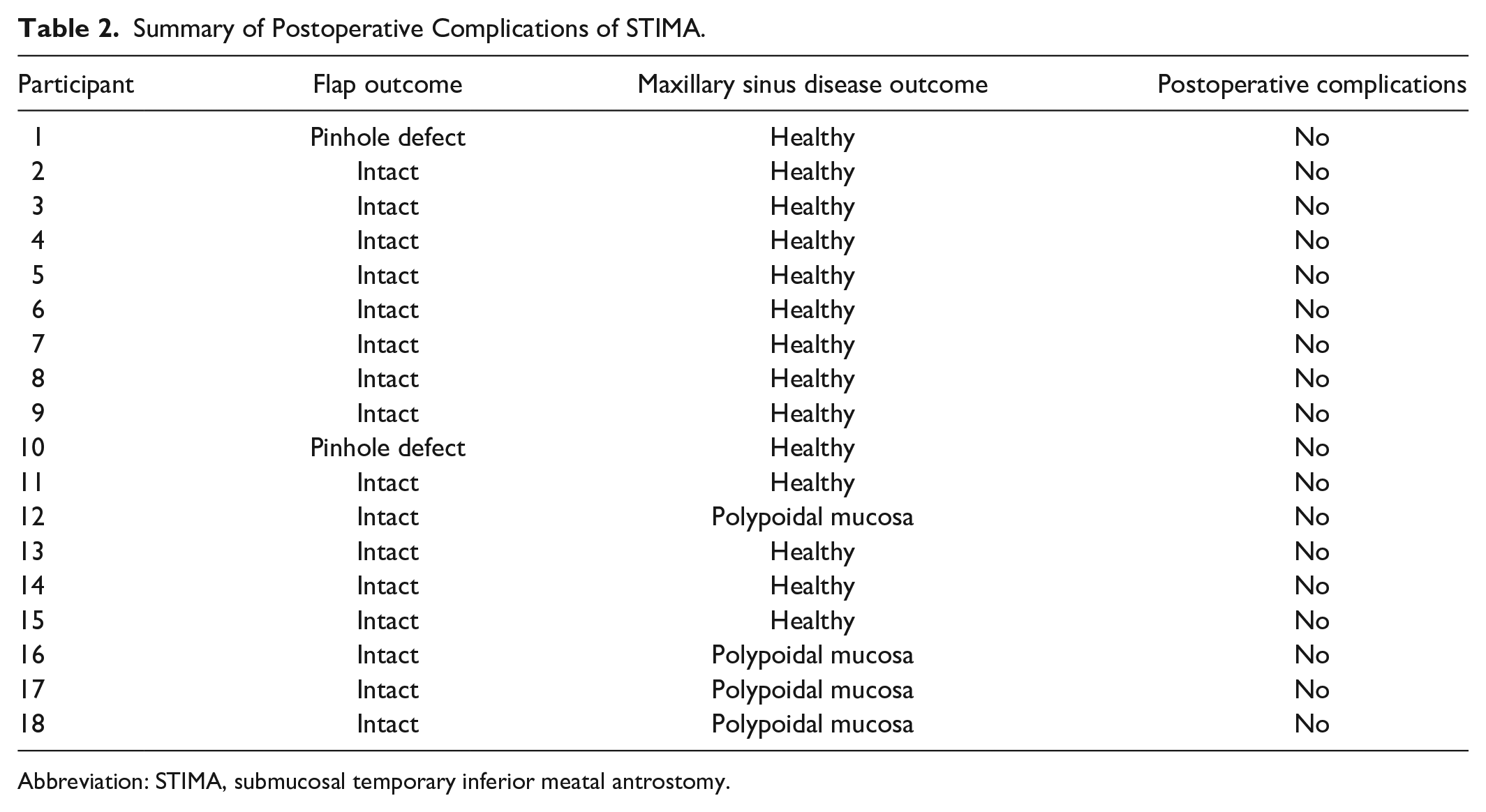
Abbreviation: STIMA, submucosal temporary inferior meatal antrostomy.
The flaps in all our 18 patients were intact with complete antrostomy site closure, with the exception of 2 patients with pinpoint asymptomatic defects in the antrostomy sites. The patients with flap defects were among the earlier cases, and this defect was subsequently avoided by creating a longer and larger flap to cover the defect in a relaxed manner (see Table 2 and Figure 1).
Discussion
Maxillary sinus diseases are extremely common and are regularly encountered in almost every otolaryngology clinic. Management ranges from simple observation and trialing of medical options to surgical interventions. 2 Observation may be sufficient, as in the case of a small asymptomatic retention cyst, but surgical intervention could be warranted depending on the pathology or its response to prior nonsurgical options. 4
In the pre-endoscopic era, IMA and the Caldwell-Luc procedure were the standard surgical approaches for various maxillary sinus pathologies because they provide easy and safe access with the use of a headlight and simple surgical tools, rather than requiring sophisticated technologies. 1 They have some known common complications, such as dental root injury, facial pain, swelling, and numbness, as in the Caldwell-Luc procedure. NLD injury and PND from the recirculation phenomenon are possible IMA complications. 7
However, after the introduction of endoscopes in the 1980s, and the adoption of the concept of the natural and physiological transport of mucus from different aspects of the maxillary sinus to its natural ostium in the middle meatus, these approaches were gradually abandoned and replaced by the endoscopic MMA.1,8
Endoscopic MMA is the current gold standard technique for addressing pathology in most cases. It includes removing the uncinate process with the aid of a maxillary sinus probe, and a combination of backbiting forceps, thru-cutting forceps, ethmoid forceps, a microdebrider, a sickle knife, and/or a freer dissector, according to the surgeon’s needs and comfort. 8 MMA provides optimal sinus ventilation and drainage, provided that the antrostomy involves the posterior aspects of the natural ostium to prevent the recirculation phenomenon, potential persistent disease, and PND. The retrograde swinging door technique is superior to the antegrade technique for avoiding orbital trauma, especially in cases of hypoplastic maxillary sinus or silent sinus syndrome, wherein the uncinate process is plastered to the medial orbital wall. However, care must be taken to avoid injury to the NLD from the backbiting forceps or powered microdebrider. 8
However, despite that MMA is considered safe and less invasive functional procedure, it has its limitations. In some cases, MMA may not provide enough access to approach certain pathologies when they are located in some hidden niches of the maxillary sinus such as lacrimal, dental, or zygomatic recesses. 5 In these difficult-to-access locations, a combined approach may be warranted. Surgeon may elect to approach them through IMA or a Caldwell-Luc procedure with the possibility of the aforementioned complications. 3 Other approaches are also available to access the maxillary sinus when the endoscopic MMA is not sufficient enough. The modified Denker’s procedure and the prelacrimal approach would provide excellent access to the anterior, posterior, and lateral walls of the sinus as well as the maxillary floor. In these approaches, partial removal of the bones of the lateral side of the pyriform aperture is needed and care has to be taken to avoid injuring the superior anterior alveolar nerve and the NLD. 9
Moreover, there have been few modifications to the IMA to avoid the recirculation phenomenon that could happen from the permanent antrostomy. Landsberg et al approached inferior antrostomy by using a 3 mm curved suction cannula around 5 mm posterior to the Hasner’s valve to penetrate the medial maxillary wall and after medializing the inferior turbinate. The hole is then widened to around 8 to 10 mm by cutting forceps. The inferior turbinate would be lateralized to its original position after clearing the lesions of the maxillary sinus. The IMA was completely closed in 8 patients out of 56 patients (14%) while it was permanently open in 48 patients (86%) and was ranging between 6 and 5 mm. They also reported palatal paresthesia, small cysts, and adhesions. 10
Zhao et al described their modified technique by elevating a small mucosal flap to allow for a small fenestration to the maxillary sinus through a bony window of about 10 mm. The flap would by repositioned back and held in place by an absorbable suture after clearing the sinus. They reported some mucosal edema postoperatively but with no recurrence of the disease and had complete closure in all of their 32 patients. 8
Choi et al also described a similar minimal inferior meatal antrostomy by generating a small mucosal flap and a minimal bone window of 10 mm. Only 76% of their 21 patients had complete closure of the IMA window in the postoperative period. 2
In this article, we described our modification of the conventional IMA. We have used a longer flap that allowed us for a larger IMA. Larger antrostomy allowed for better visualization of the pathology and easier manipulation with surgical tools to achieve optimal eradication of the disease. Since the incision is far anterior to the Hasner’s valve and the distal end of the NLD, they were securely elevated with the mucosal flap. By having a larger and longer mucosal flap, the flap was more mobile to allow for complete closure in a relaxed manner without the need for any suture. This was emphasized gradually over the course of our experience especially with the 2 cases of asymptomatic pinhole perforations which were among the earlier cases. We noticed that using the entire length and width of the nasal floor and the lateral wall of the inferior meatus as a mucosal flap would yield the optimal experience. With regard to the degree of visualization and the ease of instrumentation, we have previously demonstrated the superiority of this technique over the conventional endoscopic MMA in our cadaveric study that has been already published. 5
Our approach should also be compared to the modified Denker’s approach and the prelacrimal approach. We believe it is easier to perform and it is less invasive. In essence, it requires raising a meatal flap, very similar to raising the flap in middle ear exploration or tympanoplasty, and followed by an inferior antrostomy. As it does not require removal of the lateral wall of the pyriform aperture, drilling and/or osteotomies are not required. This should decrease the chances of lacrimal, orbital, and/or neurological injuries as well as alar collapse. 11 See Table 3 and Figure 3 for more comparative details.
Comparison Between Modified Denker, Prelacrimal Approach, and STIMA.
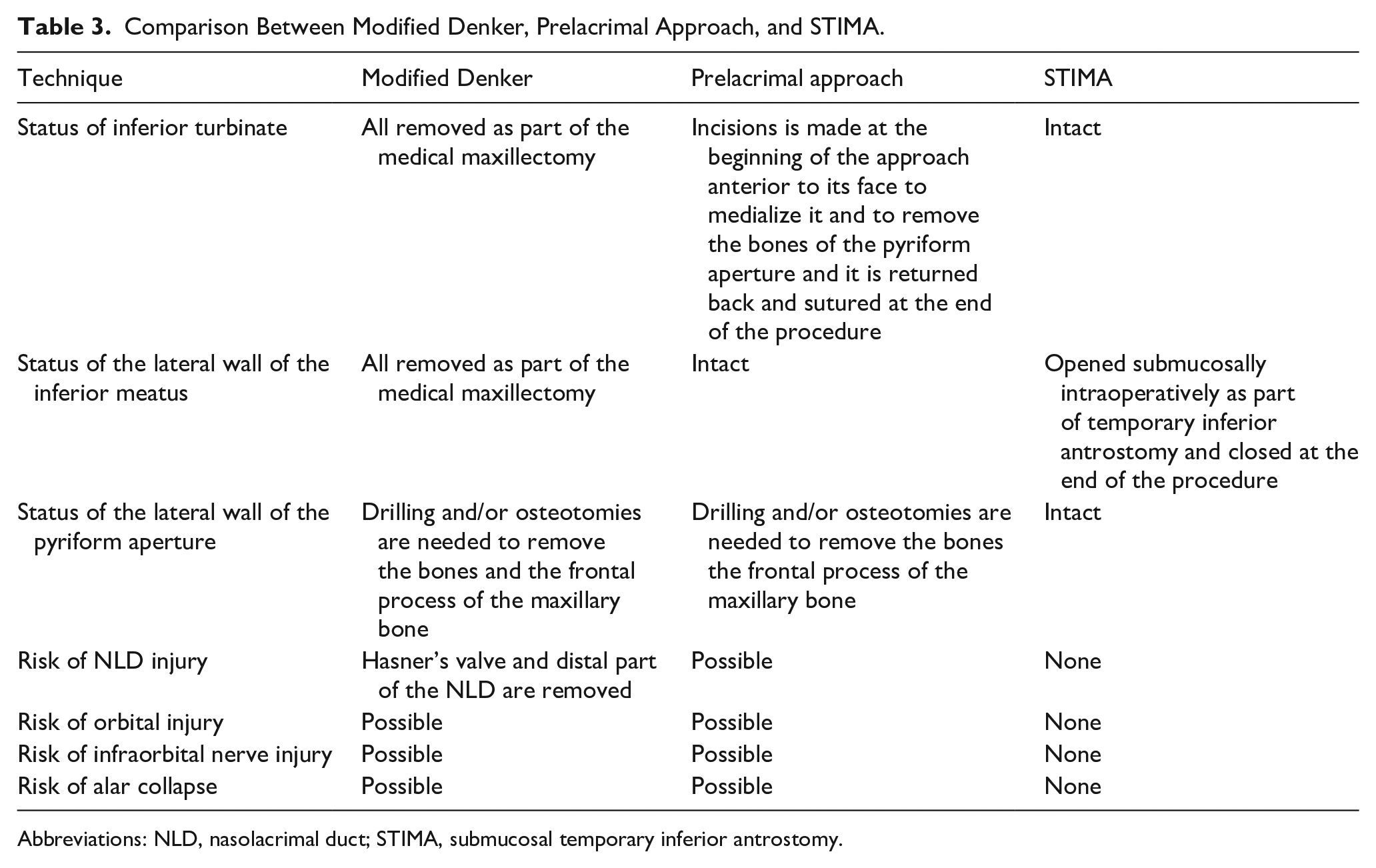
Abbreviations: NLD, nasolacrimal duct; STIMA, submucosal temporary inferior antrostomy.
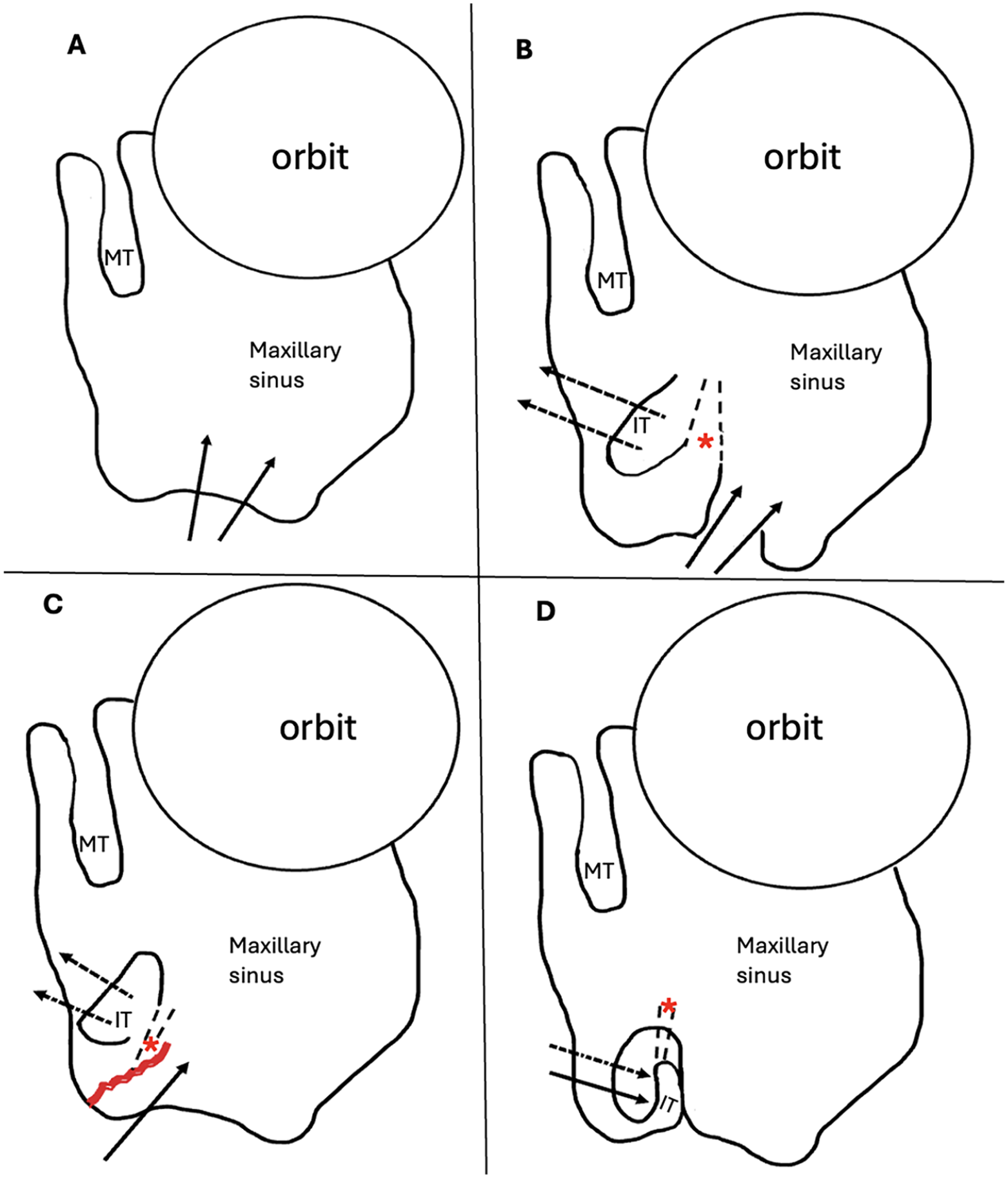
(A) Modified Denker approach (intraoperative and postoperative view are the same): Lateral wall of the pyriform aperture is removed as well as the medial wall of the maxillary sinus, including the inferior turbinate, Hasner’s valve, and the distal part of the NLD. (B) Prelacrimal approach: intraoperative view: the inferior turbinate is medialized (after an initial incision anterior to its face), the NLD is skeletonized and preserved, and the lateral wall of the pyriform aperture is removed. (C) STIMA: intraoperative view: the inferior turbinate is medialized, submucosal flap is elevated (from the nasal floor and the lateral wall of the inferior meatus, and along with it is the Hasner’s valve and distal part of the NLD) and a wide inferior submucosal maxillary antrostomy is performed. The lateral wall of the pyriform aperture is intact. (D) Prelacrimal approach and STIMA: postoperative view: the inferior turbinate is intact and the lateral wall of the inferior meatus is intact.
Last but not least, our work is not without limitations. Permanent antrostomy might be needed in some occasions and STIMA might not be appropriate. Permanent antrostomy might be necessary for optimal delivery of medications, easier instrumentation in the clinic, or in cases where direct visualization for surveillance is crucial as in the case of inverted papillomas or malignancies. However, since the antrostomy site is closed only by mucosa and lacks the bony element, it could be opened easily in the clinic under local anesthesia to achieve a permanent antrostomy, if indicated. In terms of the design of our study, our modification was performed on limited number of patients and lacks blinding, randomization, and a control group. More studies are needed to evaluate its safety, feasibility, and effectiveness.
Conclusion
In this article, we have demonstrated a surgical technique to approach maxillary sinus pathologies that are located in hidden niches and difficult-to-access locations through the conventional MMA. We presented our experience with our modification to the conventional IMA, the STIMA. We believe that it is a promising and safe technique that could be adopted when needed. However, future randomized, blinded, and controlled studies are needed on a larger number of patients to confirm its safety and effectiveness.
Footnotes
Authors’ Note
Conference Presentation: This article was presented at the IFOS Dubai January 2023.
Author Contributions
All authors agreed to be accountable for all aspect of this work. Saud Alromaih: idea, design, draft, acquired, and revised manuscript. Nouf Aloraini: idea, design, draft, acquired, and revised manuscript. Abdulaziz Alrasheed: draft, acquired and revised manuscript. Mohammad Aloulah: draft, acquired and revised manuscript. Ahmad Alroqi: draft, acquired and revised manuscript. Naif Alotaibi: draft, acquired and revised manuscript. Abdulaziz Alqahtani: draft, acquired and revised manuscript. Saad Alsaleh: draft, acquired and revised manuscript.
Data Sharing and Data Availability Statement
The data supporting our research will be available on request as per the journal guidelines.
Disclosures
We declare that this article is original, has never been published, or under the consideration for publication elsewhere (in part or in whole).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB approval was obtained from IRB committee.