
Abstract
Introduction
A patulous Eustachian tube (PET) is a condition in which the Eustachian tube (ET) remains open, causing a continuous sensation of fullness or autophony. For diagnosis of PET, before considering nasal endoscopy, the patient has to have a history of autophony that gets improved with gravity-dependent position, in some cases but not all mobility of tympanic membrane with or without closure of contralateral nostril and breathing through the ipsilateral nostril with a closed mouth. Kawamura et al proposed diagnostic criteria by the Japan Otological Society for PET, including subjective symptoms such as voice autophony and aural fullness, along with objective findings like respiratory fluctuation of the tympanic membrane. Meeting all 3 criteria results in a diagnosis of “Definite PET,” while meeting 2 criteria leads to a diagnosis of “Possible PET.” 1 In our usual procedure, we assess the mobility of the tympanic membrane using endoscopy. We instruct the patient to close the contralateral nostril and breathe through the ipsilateral nostril. This allows us to observe the mobility of the tympanic membrane. However, it is important to note that not all patients with symptoms of a PET exhibit tympanic membrane mobility during this maneuver. During our observations, the tympanic membrane immediately recoils after performing the Valsalva maneuver while the patients are in a sitting position. However, when they change to a supine position in the level, they report relief from symptoms of autophony. Interestingly, we have observed a delay in the recoil of the tympanic membranes after the Valsalva maneuver in these cases when they change to supine position. The management of PET can be challenging, and various conservative and surgical techniques are available. One such method involves using a shim, a thin, flexible, and biocompatible material inserted into the ET to occlude it partially. A simple shim can be prepared with different sizes of intravenous catheters ranging from 20 to 14 gauge, with lengths between 31 and 44 mm; it is available from other manufacturers as a Kobayashi plug. 2 The shim creates a mechanical obstruction in the ET to reduce the volume of sound and air flow transmitted to the middle ear. Several studies have reported the use of shims in PET management. The study also noted that the shims did not cause significant adverse effects, such as infection or perforation of the eardrum. 3 Ward et al 4 showed good long-term shim results with a higher need for a pressure equalization tube. The use of a shim for PET management is a minimally invasive procedure that can be performed in an outpatient setting, most of the time with a pressure equalization tube. This process involves inserting the shim into the ET through the nose under local anesthesia. Shim insertion can be performed using various methods, such as a catheter or forceps. However, it is essential to note that using a shim is not always effective for managing PET. Given the paucity of reports on the management of PET, we present our institutional management approach to PET with shim insertion in addition to a modified shim with hydroxyapatite injection and review the literature.
Methods
We conducted a retrospective case series of patients presented with PET in a single institution from February 2021 to March 2023. Institutional Review Board exemption was obtained.
Results
Case 1
A 42 year-old female with a history of sleeve gastrectomy 5 years ago that resulted in a 30 kg reduction of her weight within the first 6 months presented to our clinic after 4 years of surgery with complaints of left ear fullness, voice distortion with autophonia, and intermittent headache, which improved in a supine position. An ear examination revealed a normal external auditory canal with a moving tympanic membrane during breathing. Nasal endoscopy showed a deviated nasal septum, a hypertrophied inferior turbinate, and a concavity of mucosal valve of the anterolateral wall of the ET using a 45° rigid nasoscope. The computed tomography (CT) scan of the temporal bone was done to rule out other causes, but it was unremarkable. The patient underwent septoturbinoplasty and size 16 gauge shim insertion with a length of 35 mm on the left side. The patient was discharged without complaints. During the 20 month follow-up, her symptoms ear fullness and voice distortion with autophonia markedly improved, with a reduction in both the severity and frequency of headaches to date.
Case 2
A 42 year-old female previously diagnosed with migraine and had undergone sleeve gastrectomy presented to our clinic with bilateral headache and autophonia that improved in gravity-dependent position. The symptoms started 3 months post-surgery after she lost 25 kg. An ear examination revealed a mobile tympanic membrane during breathing through the ipsilateral nostril, and the membrane immediately recoils after Valsalva; otherwise, the membrane was normal. Nasal endoscopy showed a deviated nasal septum, a hypertrophied inferior turbinate, and a concavity of mucosal valve of the anterolateral wall of the ET using a 45° rigid nasoscope. Her CT scan of the temporal bone was unremarkable. Subsequently, the patient underwent septoturbinoplasty and size 14 gauge shim insertion with a length of 32 mm on both sides. The patient was discharged with no issues; however, after 2 months of follow-up, the shim on the left side fell off, and the patient had to visit the emergency department multiple times with symptoms of severe headaches. During the clinical follow-up, topical anesthesia (2% lidocaine) was applied with a xylometazoline nasal pack in contact with the ET orifice for 10 minutes. A shim with a smaller size of 16 gauge was reinserted bilaterally, and the headache disappeared on the same day. During this period, she was doing fine, with no complaints, no more ear fullness, or signs of otitis media with effusion (OME). Four months later, the patient gained 2 kg in weight and developed OME on the left side. The shim was subsequently downsized to 18 gauge under topical anesthesia. Finally, her symptoms improved with no signs of OME recurrence without the need for a myringotomy and ventilation tube, and the patient showed overall satisfaction during regular clinical follow-ups.
Case 3
A 38 year-old female complained of bilateral ear fullness, voice distortion, and autophonia with pulsatile tinnitus that improved in the supine position. Ear examination revealed a normal external auditory canal with a mobile tympanic membrane during the Valsalva maneuver and with breathing on the right side. Nasal endoscopy revealed a deviated nasal septum and a concavity of the mucosal valve of the anterolateral wall of the ET using a 45° rigid nasoscope. CT scan of the temporal bone was unremarkable. The patient underwent septoturbinoplasty with bilateral 16 gauge shim insertion with 35 mm length. Postoperatively, the symptoms of ear fullness, voice distortion, and autophonia with pulsatile tinnitus on the right side were markedly reduced. However, in the left ear, the patient had less satisfaction regarding her symptoms of authophonia. During regular clinical follow-ups over the next 6 months, postoperation showed both shims in place with intact tympanic membranes bilaterally. The right side was only mobile with the Valsalva and Toynbee maneuver, while the left side was mobile with ipsilateral nasal breathing, so we upsized the left side to 14 gauge with the same previous length of 35 mm under local anesthesia. The patient felt improvement immediately, with no further mobility of the tympanic membrane with ipsilateral nasal breathing. The patient followed up for 6 months with high satisfaction.
Case 4
A 37 year-old male complained of left ear fullness, voice distortion, and autophonia, which improved in the supine position. Ear examination revealed a normal external auditory canal with a left mobile tympanic membrane during breathing. Nasal endoscopy showed a normal nasal septum and turbinate and a mild concavity of the ET’s mucosal valve of the anterolateral wall using a 45° rigid nasoscope. CT scan of the temporal bone was unremarkable. The patient underwent shim insertion with a 16 gauge length of 35 mm on the left side. Postoperatively, he was highly satisfied with his symptoms for over 4 weeks. However, he later complained of pain in his left ear. On examination, OME was apparent on the left side, and the patient did not benefit from the downsizing of the shim. A few weeks later, a thick biofilm had developed around the shim (Figure 1), which had a poor response to medical management, including nasal steroid spray and antibiotics. Despite the OME and biofilm formation, the patient refused to remove the shim to avoid the recurrence of his previous PET symptoms; however, with time, his secretions worsened, and he developed ear tinnitus. Therefore, he agreed to alternative management (injection of hydroxyapatite), so after 2 weeks of removal of the shim and resolution of OME, injection of calcium hydroxyapatite was performed under local anesthesia. The patient reported partial improvement after 2 weeks. Another injection was administered (Figure 2); the patient improved but was not fully satisfied compared to the shim insertion, which was performed earlier, with no report of middle ear effusion symptoms.
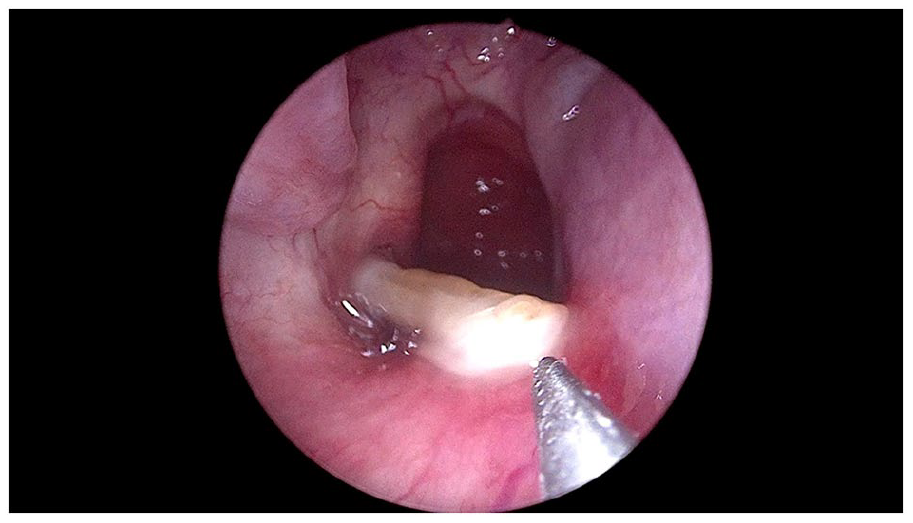
Biofilm secretion around the right Eustachian tube orifice, partially pulled out shim after trail of antibiotics.
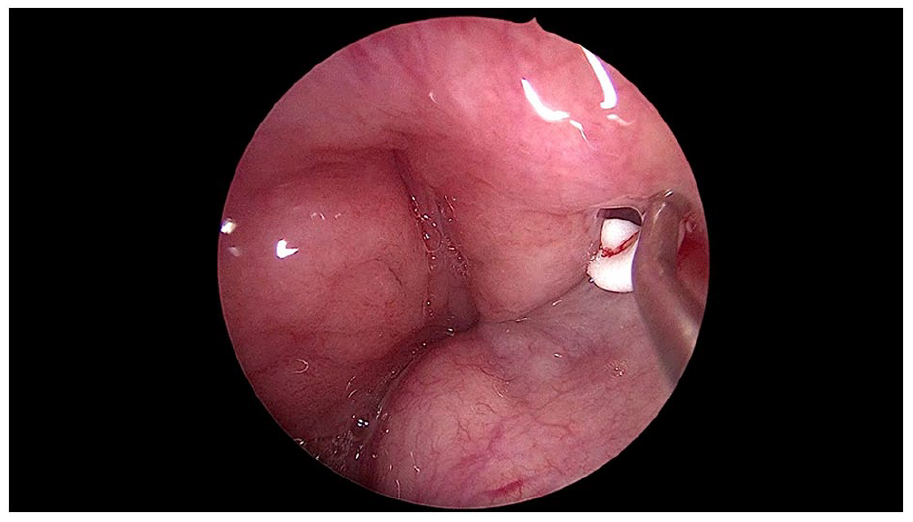
Hydroxyapatite injection in the left Eustachian tube orifice.
Discussion
Symptoms of PET may be managed medically by discontinuing medications that aggravate the symptoms, such as caffeine and diuretics, when appropriate. 4 Furthermore, during the surgical treatment of PET, a tympanostomy tube can be placed in the middle ear to address the middle ear issue, which can aggravate symptoms in approximately 50% of patients. 5 It is also possible to insert an angiocatheter surrounded by bone wax at the nasopharyngeal end of the ET to obliterate the ET lumen, augment the ET valve with calcium hydroxyapatite cement, or surgically obliterate it permanently. Nevertheless, there was a noticeable difference in the duration of symptom resolution between the procedures. 6 Compared with the hydroxyapatite injection and reconstructed ET lumen procedures, a shim placed 12 months after surgery had lower failure rates. Three-quarters of patients undergoing shim placement as their first procedure for ET experienced symptom resolution 12 months later, noting that the shim can remain in place for years. 4 Our approach includes temporary measures, such as nasal strips to correct compromised nasal valves, short-term nasal steroid spray, lifestyle modification, proton pump inhibitors, and smoking cessation. Furthermore, endoscopic shim placement is considered in patients who have not improved adequately after conservative treatment measures. If there is no septal deviation with a normal size inferior turbinate, we sometimes go with shim insertion under local anesthesia protocol. We observed the patient who underwent shim insertion under local anesthesia while in a sitting position had an easier insertion compared to those who had the procedure under general anesthesia while lying down in a supine position; this observation is consistent with the findings of Yoshida et al, 7 who previously made a similar observation when comparing CT scans taken in sitting and recumbent positions, and found that the air space in ET lumen was larger in sitting position. If the septum or turbinates are hypertrophied, we do it under general anesthesia by correcting deviated nasal septum and turbinoplasty. Different intravenous catheter sizes can be used to prepare a shim, from size 20 gauge to size 14 gauge, ranging in length from 31 to 44 mm. 2 A patient’s gender and head size determine the length of the shim, whereas the ET opening determines the size of the shim. In our practice, we usually start with 16 gauge; if symptoms persist, we increase the size to 14 gauge; and if a patient develops effusion, we decrease the size to 18 gauge in the clinic under topical anesthesia. In some patients, topical or local anesthesia was not administered. In this procedure, the ET is partially closed, and the shim size is adjusted until the symptoms of PET are eliminated while, at the same time, avoiding effusion of the middle ear by completely closing the ET without inserting pressure-equalizing tubes; therefore, foregoing the need for an additional procedure. In our experience, shim failure usually occurs due to biofilm formation and thick secretions, which leads to the shim being pulled out into the nasopharynx while swallowing. However, there have been no cases of a shim falling or causing aspiration due to the adherence of the shim to the nasal mucosa, which prevents it from falling into the lower airway. In such cases, alternative management with an injection of hydroxyapatite is also performed under topical anesthesia using the same protocol as for shim insertion. This technique has been used as a late management option to avoid complications. At our tertiary center, 45 patients with PET sought treatment. Nine patients improved with conservative measures, while the others underwent surgical interventions ranging from shim placement to septoturbinoplasty, with or without shim placement, to the injection of hydroxyapatite.
In this case series, we chose 4 cases that reflected our overall practice. We used shims in all 3 cases combined with septoturbinoplasty. In the first case, the patient’s symptoms improved without complications. We found that patients who developed PET after weight reduction had a better prognosis than those who developed idiopathic PET. This finding is consistent with a study conducted by Wu et al, 8 who reported that patients with rapid weight loss (RWL) were significantly more likely to achieve symptom improvement after the intervention than patients with non-RWL. During follow-up, some patients experienced resurfacing PET symptoms after shim failure. In such cases, different methods are used, such as changing the size of the shim under topical anesthesia. In the second case, the symptoms improved immediately, and the patient’s voice changed in pitch.
Furthermore, patients who underwent shim insertion were more likely to develop OME than those who did not. Downsizing the shim under topical anesthesia is a suggested approach for patients who complain of OME following shim insertion. The advantages of this technique are that it can be performed in a clinical setting, with or without topical anesthesia, with immediate symptom improvement, thereby avoiding the need for myringotomy and ventilation tube insertion. We noticed that the size of the shim does not play a significant role in displacement. Regardless of the size of the shim, we noticed in all cases, the displacement is related to the presence of thick mucus around the shim, which pulls it with swallowing out of ET. Injection of hydroxyapatite is used as a late option because it is less effective than shims in treating the symptoms of PET, as reported by Vaezeafshar et al, 9 where endoscopic hydroxyapatite injections relieved autophony and ear fullness in 57% to 63% of patients. Our study used it in cases of biofilm formation and thick secretions. It is usually administered under local anesthesia after shim removal, as in the fourth case. Size adjustment of the shim is a suggested method to avoid middle ear effusion while reaching the maximum level of symptom relief without needing tympanostomy tube insertion; it is safe, effective, and usually performed under local or topical anesthesia in the clinic.
Conclusion
Shim insertion for the treatment of PET is considered safe, reversible, and adjustable, giving satisfactory results while avoiding middle ear effusion. It can be performed under local or topical anesthesia in the clinic, and size adjustment is a suggested method to get maximum relief without middle ear effusion.
Footnotes
Data Availability
The data used to support the findings of this study are included within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.