
Abstract
Objective:
Patulous Eustachian tube (PET) is a clinical condition that is associated with troublesome aural symptoms and is difficult to be treated successfully. The purpose of this review is to examine the published literature regarding the therapeutic value of the current treatment options for PET.
Methods:
We searched Web of Science, PubMed and Medline from 1999 to 2019. The search focused on papers concerning the clinical evaluation of treatment methods in PET patients. Statistical techniques were not used.
Results:
Prospective and retrospective case series were the types of trials available for review. We included 28 articles that evaluated the efficacy of various conservative and surgical therapeutic options. The recovery rates ranged from 50% to 100%. In most studies the assessment of efficacy was based on the subjective improvement of patient symptoms as there is no validated outcome tool available. No severe adverse events were observed in any study.
Conclusion:
On the basis of the available literature, it seems that conservative treatments can be considered as a primary therapeutic option for PET. Concerning the surgical interventions they seem to be a safe and valuable solution in patients with refractory disease. Finally, given the low level of evidence, prospective case–control studies with long follow-up and robust setting looking into the therapeutic approach of PET are required. The need for establishment of standard criteria of PET recovery should be underlined.
Introduction
Patulous eustachian tube (PET) was first described by Schwartze in 1864. 1 The Eustachian tube (ET) remains ordinarily closed and opens transiently during swallowing, yawning, and other voluntary or involuntary efforts. Patulous eustachian tube is a clinical condition characterized by abnormal patency of the valve of ET at rest. It results in annoying symptoms that often have a severe negative impact on the patient’s quality of life. 2 Namely, PET typically presents with autophony, tinnitus, aural fullness, and mild hearing loss. The diagnosis is clinical and is based on verification of synchronous movement of the tympanic membrane (TM) in response to forced breathing or sniffing. 3 Patulous eustachian tube is an uncommon otologic condition that has an estimated incidence from 0.3% to 6.6% in general population. 4,5
With regard to the etiology of PET several theories have been proposed, including loss of tissue within the cartilaginous portion of ET (weight loss, pregnancy, use of high-dose oral contraceptives, and estrogen therapy) and atrophy or scarring within the nasopharynx or involving the musculature associated with ET function (adenoidectomy, radiation therapy, poliomyelitis, and other iatrogenic trauma). 2,6,7
Various treatment modalities for PET, both conservative and surgical, have been proposed with no standard protocol universally accepted. Noninvasive treatments include nasal saline irrigation, orally administered tranquilizers, topical estrogen drops, insufflations of salicylic acid–boric acid powder, and mucus thickening agents. 8 -10 However, most of these interventions are only of temporary benefit. For refractory cases of PET, several surgical interventions have been proposed to control the symptoms. Surgical procedures can be classified according to the site of intervention into 2 main categories: tympanic membrane manipulation techniques, and ET occlusion treatment techniques. The objective of this review was to assess the therapeutic value and efficacy of the current PET management options.
Materials and Methods
We searched PubMed and MEDLINE databases from 1999 to 2019 for original articles, and case series concerning the management options of PET. To be included in this review, studies had to be original published reports evaluating any intervention to treat the symptoms of PET. No minimum follow-up was required. Only articles published in English were reviewed. Non-English articles, animal studies, case reports, and letters to the Editor were excluded. The following search terms were used: patulous eustachian tube, eustachian tube dysfunction, autophony, and eustachian tube. Limiting search term were medical treatment and surgical treatment. Additional articles were identified by hand searching the reference lists of the retrieved articles. Cases reports were excluded. Two authors (P. K. and E. P.) independently graded the articles for eligibility criteria, and any disagreement was resolved by discussion. A disagreement emerged on the eligibility of 3 articles with a small sample size. 11 -13 However, it was finally decided that all these studies will be included in the review as the available literature on PET management is rather limited.
The found articles were analyzed with regard to the therapeutic procedure that was followed (conservative measures or surgical approach), the success rate of each treatment protocol, the criteria of improvement used to evaluate the results, and the associated complications.
Results
Twenty-eight studies met the inclusion criteria of this review. The initial search using the term “Patulous Eustachian tube” yielded 200 citations, of which, 103 failed to meet the inclusion criteria and 28 were not published in the English language. Moreover, 42 articles were excluded because they were case reports, animal studies, letters to the Editor, or replies. The remaining 27 studies were included in the review. The use of the rest search terms and the hand search yielded 1 additional study, bringing the number of articles meeting the inclusion criteria to 28. Eighteen of the papers were retrospective case series and 9 were prospective case series (Figure. 1). There was just 1 author who performed a controlled trial. 14 However, in this trial no mention of randomization was made in its methods at all.
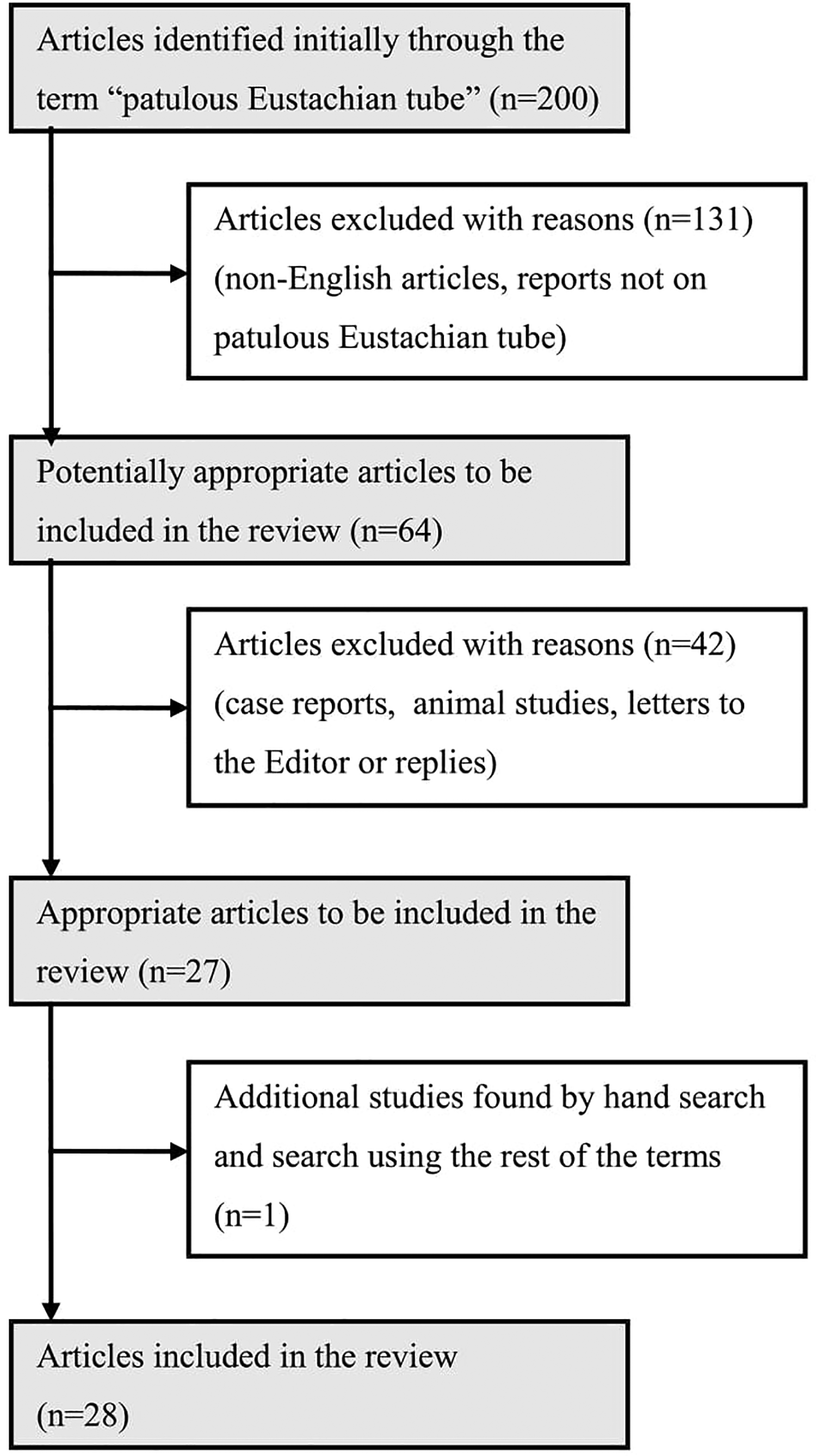
Flow chart of the reviewing process.
Most of the studies used surgical techniques for PET patients who failed the initial conservative therapy. 15,16 Some of the articles assessed the therapeutic value of surgical methods as a primary therapy. The rest of the articles studied the efficacy of noninvasive treatments. 10,14,17 In the majority of the trials, the diagnosis of PET was made based on the presence of typical aural symptoms (autophony to voice, autophony to respiration, and/or aural fullness) combined with visible excursions of the TM on respiration. In some studies patients were diagnosed by the diagnostic criteria proposed by the Japan Otological Society. 18
Treatment Modality
Various methods of treatment for PET, including conservative therapy and surgical procedures, have been found. The described surgical techniques differed in many aspects, including the anatomical site of intervention (TM or ET), and the type of used anesthesia (general or local). The procedure type most authors applied was plugging of ET. Several materials were used for this reason, including silicone plug, catheter, tragal cartilage, and fat. There were 7 articles that studied the efficacy and safety of plugging of ET using a silicone plug for PET. 11,15,19 -23 Four authors used other materials for plugging the ET, such as catheter, tragal cartilage, and shim filled with bone wax. 16,24 -26 A number of authors applied other methods of ET occlusion. Namely, 6 studies investigated injection of bulking substances at the ET orifice, and 3 investigated cautery or suture ligation of the ET orifice. 12,13,27 -33 Four articles studied the efficacy of eardrum thickening approach either via myringoplasty or via paper patching. 14,17,34,35 Two authors described the patulous ET reconstruction (PETR) technique. 2,36 One article described nasal instillation of saline for the treatment of patients with symptoms of PET. 10 The rest of the articles used combination approaches.
Efficacy - Complications
The criteria of recovery that were used in the included articles varied considerably. In most studies, the assessment of efficacy was based on subjective improvement or resolution of patient symptoms. A small number of authors used additional objective findings and measurements, including TM movement, auscultation of voice sounds, sonotubometry, audiometry, and tubotympano-aerodynamography. In some studies, success was defined as a sum of complete and significant improvement, while in others, patients with partial recovery (both significant and slight) were included in the overall symptom resolution rate. The recovery rates range from 50% to 100%. 24,33 Six studies reported symptomatic improvement in 100% of study participants. 11 -13,23 -25 However, most of these studies included small patients’ populations. Overall rates of improvement for ET plugging techniques varied between 64.3% and 100%. 24,26 Eustachian tube plugging technique with the lowest reported efficacy included tragal cartilage chip insertion (64.3%). 26 The efficacy of ET orifice injection technique ranged between 50% and 100%. 13,33 Studies investigating cautery and suture ligation of ET orifice reported symptomatic improvement in 60% to 100% of patients. 12,28 Two studies performing PETR reported complete relief in 7% to 72.7%. 2,36 Effectiveness of paper patching approach varied between 76.2% and 87%. 14,17 Few complications were reported, such as middle ear effusion (mostly transient), TM perforation, plug descent, pain, tinnitus, foreign body sensation, and facial or tongue numbness. No severe adverse events were observed in any study. Table 1 summarizes the results of each study, describes the criteria of recovery each author used, and reports the caused complications (Table 1).
Results of Therapy in 28 Clinical Studies on Patulous Eustachian Tube.
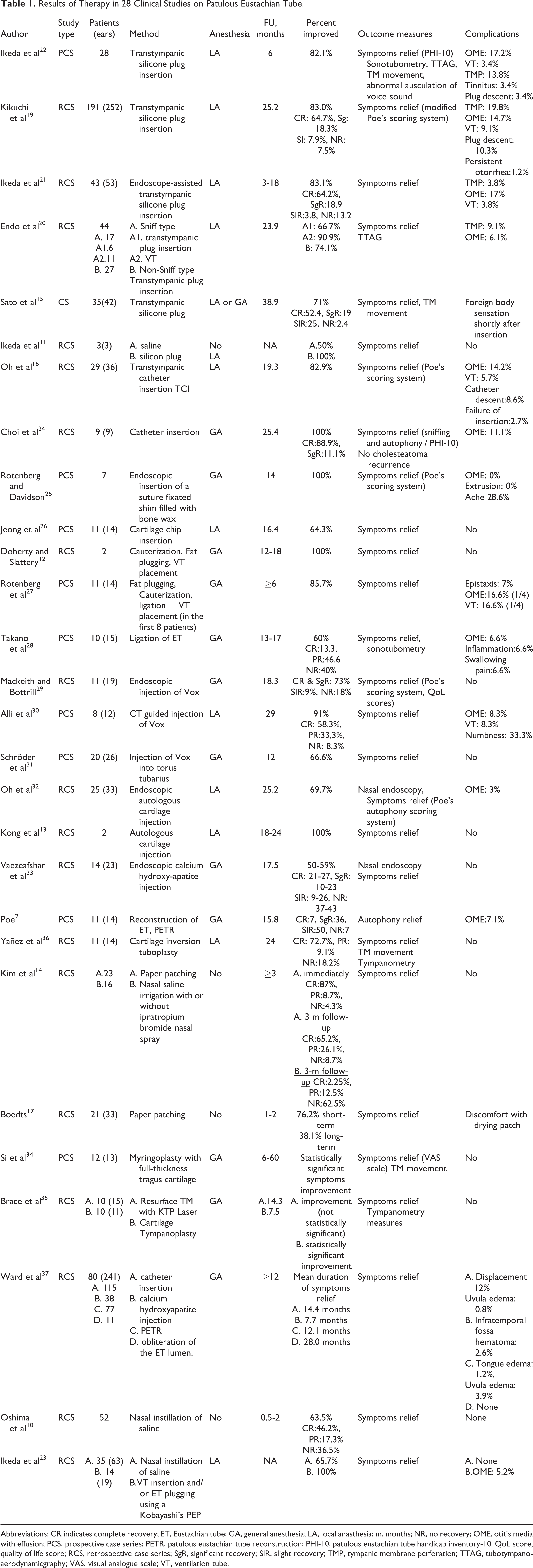
Abbreviations: CR indicates complete recovery; ET, Eustachian tube; GA, general anesthesia; LA, local anasthesia; m, months; NR, no recovery; OME, otitis media with effusion; PCS, prospective case series; PETR, patulous eustachian tube reconstruction; PHI-10, patulous eustachian tube handicap inventory-10; QoL score, quality of life score; RCS, retrospective case series; SgR, significant recovery; SlR, slight recovery; TMP, tympanic membrane perforation; TTAG, tubotympano-aerodynamicgraphy; VAS, visual analogue scale; VT, ventilation tube.
Discussion
Best Method
Management of the PET continues to be a challenge. It is obvious that the optimal treatment goal for this medical condition would be to achieve normal ET function and good middle ear aeration without the need for a ventilation tube. Thus, ET reconstruction without luminal obliteration would theoretically be the ideal therapeutic option. However, such procedures are technically challenging, have a relatively high cost, and are time consuming in the operating room. 2 Moreover, PET is a benign medical condition that is not associated with serious complications. This means that the anticipated benefits of a proposed surgical treatment modality must be weighed against potential risks. Thus, extremely complicated surgical techniques performed under general anesthesia should be met with skepticism. As long as conservative treatment of PET is sufficient in most patients, surgical treatment should be considered only in refractory cases.
To date, various surgical methods have been devised for refractory PET. 38 Poe introduced the PETR technique using autologous cartilage block and presented good results. 2 However, this intervention is not easy because it requires a combined endoscopic transnasal and transoral approach under general anesthesia. The technique most authors applied is transtympanic or transnasal ET plugging, using a catheter, cartilage, or silicone plug. Multiple studies have demonstrated promising results with this method, which has the advantage of being reversible, less invasive, safer, and more cost efficient than others. 16,19 A disadvantage is the potential otitis media with effusion resulting from complete closure of ET. Moreover, it should be noted that there is no perfect method to select a suitable plug size for each case. Finally, the plug can descend to the nasopharynx.
Another method for narrowing the ET involves the injection of a bulking agent at its nasopharyngeal orifice. 29,30 The main advantage of this technique is the fact that it is minimally invasive, relatively easy, and is performed under local anesthetic. On the other hand, it is difficult to estimate the optimal volume of agent to be injected. This is due to the fact that the material is injected into a fat-filled tissue space without clear boundaries and the leaching out of the agent occurs in an unpredictable manner. It should be underlined that through this intervention a static augmentation of a complex dynamic structure is performed. 29 Finally, such treatment is associated with potentially severe complications due to inadvertent injection into the carotid artery.
Eardrum thickening approach via myringoplasty without intervention of the ET can also be used for the management of PET symptoms. 34 Tympanic membrane is more easily accessible compared to the nasopharyngeal ET orifice, and tympanoplasty as a surgical technique is safe and familiar to the otolaryngologist. In addition, the preoperative patching test could be a valid way to predict the outcome of the procedure. However, this surgical intervention is performed under general anesthesia, and further studies are needed to investigate whether or not TM manipulation leads to hearing loss. Paper patching of the TM, a recently developed minimally invasive treatment option, has been reported to yield rapid symptomatic relief that is temporary. 14,17 Finally, ventilation tube insertion resolves mainly the symptom of aural fullness and seems to be effective in specific groups of patients, such as PET cases with associated habitual sniffing. 20 Conclusively, in recent years, there has been increasing preference for ET plugging techniques apparently because of the several key advantages that they provide.
Percent Improved—Long-Term Effectiveness
The range of recovery rates in patients with PET is very wide. 13,33 This is primarily related to the fact that the included reports assess the efficacy of different treatment modalities. Another possible reason may be the small sample size in some of the studies. However, the best explanation may lie in what is considered a successful treatment outcome. The criteria to which the authors define recovery were variable between studies. It is obvious that the different criteria of symptoms improvement and the absence of a validated outcome tool hinder the interpretation of the results and make difficult the comparison of different published case series. Apart from the small patient samples, the high variability of treatment modalities, and the lack of a validated assessment tool, it should be underlined that none of the studies included in this review rose above fourth Oxford Centre for Evidence-Based Medicine (OCEBM) level of evidence. However, some general conclusions can be drawn. Namely, conservative treatments seem to be effective for more than half of the patients. 10,23 This means that they could be considered as a valuable primary therapeutic option. On the other hand, most of the proposed surgical methods seem to be beneficial for refractory PET. Thus, such interventions could be used as salvage treatment in patients with persistent disease after conservative therapy. The most commonly reported surgical technique is ET plugging. 19,22 As numerous studies have shown good results with insertion of silicone or catheter in the ET, it appears to be an established way of dealing with PET. 16,21 Consistent with this conclusion are the results of the study reported by Kikuchi et al in which trans-tympanic plugging of the ET using the Kobayashi Plug was performed for 252 ears. 19
The goal of therapy for PET is to achieve long-lasting normal ET function, that is, no PET symptoms and good middle ear aeration. However, because of the fact that most of the studies have relatively short follow-up period, there are little data on long-term outcomes of the treatment methods for PET. It has been established that most of the conservative modalities are of temporary benefit. The same problem seems to occur in a number of surgical treatments. Namely, some autologous materials (fat, cartilage) used for ET occlusion have a high resorption rate. Ligation of ET is also possible to loose gradually compromising the long-term effect. Moreover, the beneficial effect of paper patching seems to decrease over time. 14,17 On the other hand, in one of the largest series of patients available in the literature Kikuchi et al reported that Kobayashi Plug induced long-term effectiveness for over 80% of the cases with chronic and severe PET. 19 Ward et al reported that shim insertion and obliteration have more enduring symptom resolution in comparison with hydroxyapatite injection or patulous ET reconstruction. 37
Complications
Ιn the nonendoscopic surgical era, some treatment modalities were associated with serious complication, such as the inadvertent injection of filler material into the internal carotid artery. In contrary to that no severe or life-threatening adverse events were observed in any of the included studies of this review. A possible explanation for this would be the fact that imaging technologies have been improved and endoscopic sinus surgery has been developed facilitating the completion of most of the surgical techniques for PET with a high level of precision and control.
One of the most commonly reported complications was otitis media with effusion (OME). However, the incidence of this adverse event was lower than expected, especially in surgical methods based on the occlusion of ET. 15,27 Although it would be expected that OME would occur in almost all cases of plug or catheter insertion, its rate did not exceed 20% in any of the included studies. Namely, rates of OME in patients who underwent transtympanic silicon plug insertion varied from 6.1% to 17.2%. 20 -22 In patients who performed transtympanic catheter insertion, the incidence ranged between 11.1% and 14.2%. 16 -24 The surgical intervention of ET occlusion with the lowest reported rates of OME was ET orifice injection technique (up to 8.3%). 30 Actually, most of those cases are transient and VT insertion is rarely required. This interesting finding can be explained either by the fact that many of these methods narrow the ET and a small lumen remains sufficiently patent or by the fact that the epithelial mucosa lining the middle ear being proficient enough in the role of gas and fluid exchange to prevent an effusion. However, acute change of atmospheric pressure is mainly regulated by the ET. Therefore, patients who are often exposed to acute changes of barometric pressure such as aircraft flight or scuba diving are not considered good candidates for ET occlusion surgical techniques.
A potential limitation of the ET plugging techniques is the possibility of plug dislodgement. Rates of plug descent varied from 3.4% to 12%. 22,37 However, according to some recent reports, this problem has been resolved. Namely, Kikuchi et al designed a new type of silicone plug with wider tail that had 2 small protrusions to each side. According to them plug descent to the nasopharynx completely ceased to occur after introduction of the new Plug. 19 As a result, the rate of reinsertion was minimized. Rotenberg and Davidson proposed suturing of the catheter to the anterior cushion of the torus using an endoscopic needle driver. 25 Finally, tympanic membrane perforation was reported in studies, in which transtympanic ET occlusion was performed. The rates of this complication ranged between 3.8% and 19.8%. 19,21 In general, most of the currently used surgical methods for PET have a good safety profile.
Conclusions
On the basis of the available literature, although conservative treatments are only of temporary benefit, they can be considered as a primary therapeutic option for PET. With regard to surgical interventions, they seem to be a safe and valuable solution in patients with refractory disease. Surgical methods, especially ET plugging techniques seem to yield long lasting improvement. However, given the low level of evidence, prospective studies with long follow-up and robust setting looking into the therapeutic approach of PET are required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.