
Abstract
This article presents 2 cases of extremely intractable patulous Eustachian tube following multiple transnasal shim insertion. These cases highlight the disadvantages of repeat transnasal shim operations, including enlargement of the Eustachian tube lumen, frequent dislocation, repeat surgery, recurrent middle ear infection, and shim misswallowing. The patients in these cases were successfully treated with Eustachian tube cartilage chip insertion through a postauricular approach. We describe the surgical technique and advantages of this promising management method.
Introduction
The Eustachian tube (ET) connects the middle ear space to the nasopharynx. The functions of the ET include pressure equalization, mucociliary clearance and drainage, and protection from both the nasopharyngeal environment and loud sounds. 1 Patulous Eustachian tube (PET) is a benign condition initially described by Schwartz in 1864. 2 The PET is characterized by symptoms including voice autophony, breathing autophony, and aural fullness.3,4 Possible etiologies of PET include atrophy of the peritubal fat tissue, peritubal muscular dysfunction, weight loss, and pregnancy. 3
No standard treatment strategy is available for PET. Conservative methods include weight gain, oral saturated solution of potassium iodide, and estrogen nasal spray. 2 However, some cases may require surgery. Various surgical techniques have been reported, including ET orifice plugging (shim technique), ventilation tube placement, suture ligation, endoluminal cauterization, and hamulotomy. 3 The success rate of these procedures varies from 22% to 100%. 3 Jeong et al reported transtympanic cartilage chip insertion for intractable cases. 5 Herein, we report 2 difficult cases with persistent refractory disease after numerous surgical procedures, including ventilation tube insertion, hyaluronic acid injection, and repeated transnasal shim technique. We performed ET autologous cartilage insertion through a postauricular approach as salvage management. Both the treated patients exhibited a favorable response and have remained symptom-free.
Case 1
A 40-year-old woman complained of bilateral severe autophonia and aural fullness for 10 months. She had a history of rapid body weight loss (10 kg) after delivery before symptom onset. The autophony interfered with the patient’s speech, hearing, and daily activities. Insomnia was also reported. Flexible nasopharyngoscopy revealed a large ET orifice (Figure 1A).
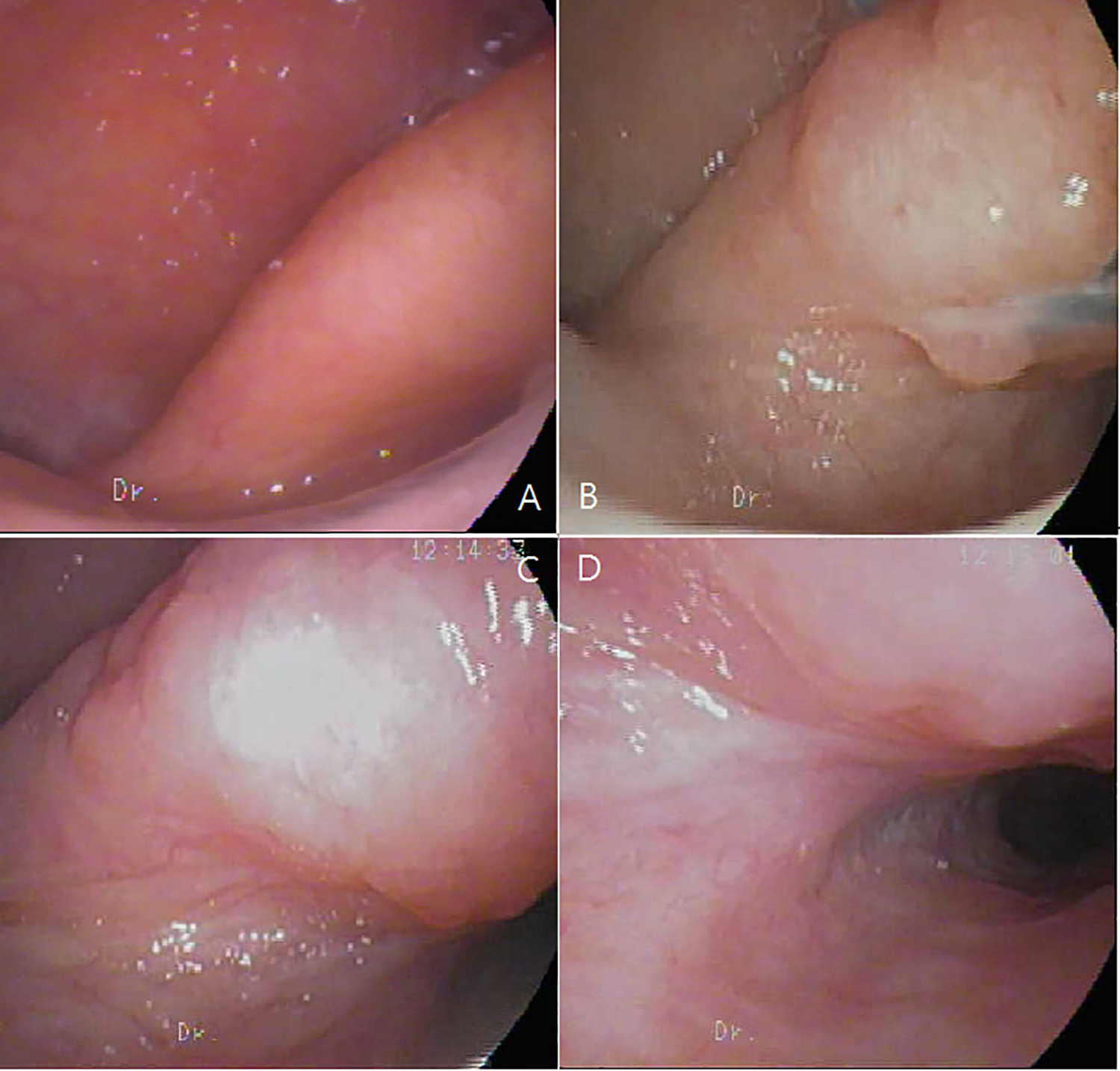
Case 1. A, Large ET orifice before treatment. B, Enlarged ET orifice after 4 shim insertions and 1 HA injection. C and D, Extremely large ET orifice after 11 surgeries. ET indicates Eustachian tube.
After treatment failure, the patient received bilateral endoscopic transnasal shim technique (transnasal endoscopic ET insertion of catheter filled with bone wax) in 2015. The right-side shim remained in position with complete symptom remission. However, frequent dislocation of the left-side shim occurred every few months after the first operation. From 2015 to 2018, the patient received a total of 8 left-side revised shim operations. Obvious ET opening dilatation was noted (Figure 1B-D) with a catheter diameter increase from 5 to 7F. We also employed different ET suture techniques to fix the catheter with silk suture and V-Loc barbed suture, but all shims dislocated within several weeks to months. Hyaluronic acid injection to the peritubal area was performed once with little effect.
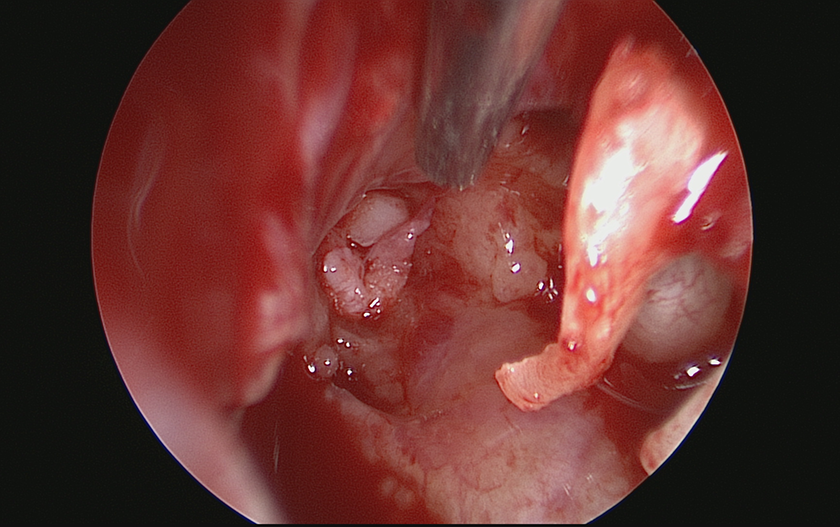
During this period, several episodes of recurrent sinusitis and acute otitis media with effusion occurred. Nasopharyngoscopy indicated that the shim was persistently coated with mucopus and fungal hyphae (Figure 2). Bacteria colonizing the catheter were highly suspected as an infection source to the middle ear. In another episode, the shim dislodged into the oropharynx and was then misswallowed. Esophagogastroduodenoscopy had to be conducted to exclude foreign body impaction.

Shim covered with fungal hyphae.
Eventually, left ET cartilage chip insertion was suggested to the patient. With a postauricular approach, the tympanomeatal flap was raised to expose the mesotympanium under a microscope. An endoscope (3 mm, 30°) was applied to identify the tympanic orifice of the ET. The concha cartilage was harvested and cut into 3 pieces (length, 15, 8, and 8 mm; width, 2 mm). The longest cartilage chip was inserted with alligator forceps to reach the isthmus. Subsequently, the shorter pieces were inserted nearby for reinforcement (Figure 3). In the follow-up 17 months after operation, the symptoms of autophonia and aural fullness disappeared completely. The endaural wound healed well without middle ear infection or effusion.
Cartilage inserted into the ET orifice. ET indicates Eustachian tube.
Case 2
A 37-year-old woman complained of right aural fullness and autophonia after skull base fracture in a traffic accident. The autophony interfered with daily activities. Flexible nasopharyngoscopy revealed a large ET orifice.
Initially, she underwent ventilation tube insertion with no improvement. Then, 3 shims (from 5 to 8F) were replaced in 2016 because of severe widening of ET lumen caused by the skull base injury. We finally had to use an 8F dilator of the central venous line as a shim to eliminate the symptoms. However, the autophonia recurred 2 years later. The shim was still in place and a further enlargement of the ET orifice was noted.
On the basis of our experience with case 1, we did not use the shim technique for this difficult case. ET cartilage chip insertion through a postauricular approach was performed in January 2019. The patient reported complete absence of autophonia 10 months after operation.
Discussion
The transnasal shim technique was described by Rotenberg and Davidson. 6 The technique involves inserting an intravenous catheter filled with bone wax into the ET under an endoscope to obstruct the lumen. The advantages of this technique include easy observation of the shim position and the ability to remove the catheter. In most scenarios, otitis media with effusion is reported as a complication with this method. 6 However, we observed several unreported complications in difficult cases. First, the catheter was easily dislodged even when fixed with sutures. We developed nasopharyngeal silk suture techniques using laryngoscopic instruments and a knot-pusher to fix the shim on the ET cushion. Because of the narrow space and difficult manipulation, we further simplified our suture technique by using V-Loc barbed suture. However, in most conditions, the sutures were unable to fix the shim for an extended period. We believe that frequent daily swallowing and palatal motility led to suture breakdown and thus shim dislodgment.
Second, we surprisingly found that the ET diameter was dilated after repeat shim insertion, which induced symptom recurrence, and we had to increase the catheter size to compensate for this dilatation. In our second patient, we shifted to an 8F dilator of the central venous line to reduce symptoms. This is the first report of the use of a central venous line dilator as a shim. However, even this shim eventually caused further ET dilatation. We believe that repeat shim insertion may exacerbate the problem. Alternative management should be strongly considered if repeated shim insertion is required.
Third, a foreign body reaction and ascending infections along the shim may cause middle ear infection. We clearly observed mucopus- and fungal-hyphae-coated shim several weeks after insertion, with clinically recurrent otitis media and sinusitis. We removed the shim in this condition.
Fourth, the risk of shim misswallowing after dislocation may be underestimated. To our knowledge, this is the first case report to reveal these rare complications.
Transtympanic plug insertion through the elevation of the tympanomeatal flap was first reported by Bluestone and Cantekin. 7 Kobayashi attempted to treat PET with silicone plug insertion through anterior–superior myringotomy. 8 They designed a 22- to 25-mm-long silicon tube as a plug and reported a success rate of 83.1%. 9 Compared with the transnasal shim technique, transtympanic cartilage insertion has more benefits, including lower risk of dislodgement and foreign body misswallowing. However, tympanic membrane perforation is a common complication with this technique, with reported rates from 3.8% to 17.5%.9,10 The Kobayashi silicone plug is not available outside Japan. Jeong et al. 5 developed a technique that uses an autologous cartilage chip as the plug. They reported 11 cases with 14 ears receiving transtympanic cartilage chip insertion with an immediate success rate of 92.9%.
In our intractable cases, repeat shim insertion failed. We selected autologous cartilage chip insertion through a postauricular approach as salvage management. We opted to elevate the tympanomeatal flap instead of myringotomy to approach the ET orifice, with the advantages of decreased tympanic membrane perforation risk and a better view. Furthermore, we harvested the conchal cartilage instead of tragal cartilage because of the high volume requirement and to avoid a tragal scar. Autologous cartilage can significantly lower foreign body reactions, subsequent pathogen colonization, and infection. Most importantly, in contrast to irreversible invasive procedures such as diathermy and suture ligation of the ET orifice,3,11 cartilage chips can be removed if needed. We thus believe that our technique can be an effective treatment choice for intractable PET.
In the surgical management of PET, we encountered a dilemma regarding the degree of ET obliteration. Underclosure of the ET lumen leads to only minor improvement in clinical symptoms. Complete obstruction of the ET without middle ear ventilation would eventually cause chronic otitis media, effusion, and even mastoiditis. In our case, no middle ear effusion was noted after surgery. We hypothesized sufficient cartilage is present to avoid autophony and adequate space between chips to allow ventilation. Long-term follow-up is required to evaluate whether any otitis media effusion or ventilation problems develop. We believe that room remains for surgical design and modification.
Conclusion
Intractable PET following multiple transnasal shim operations has several disadvantages, including enlargement of the ET lumen, frequent dislocation, repeat surgery, recurrent middle ear infection, and shim misswallowing. ET cartilage chip insertion through a postauricular approach as a salvage technique may be an effective alternative management method.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.