
Abstract
Introduction
Raising tympanomeatal flap via external auditory canal (EAC) skin incision is a basic procedure for repairing posterior marginal perforation. However, raising tympanomeatal flap had the following several drawbacks: (1) it resulted in EAC stenosis and EAC cholesteatoma.1,2 (2) It damaged chorda tympani nerve and caused taste disturbances, it is reported that the rate of chorda tympani nerve injury was 4.0% to 37.4%.3-6 (3) It increased the EAC bleeding and thus prolonged the operation time. Although some scholars applied the removal of a small rim of the EAC to repair marginal perforations, so far, although it shortened the operation time compared with raising tympanomeatal flap, the removal of a small rim still required the EAC incision. 7 Recently, we performed endoscopic cartilage-perichondrium graft underlay technique with preserving EAC skin for repairing posterior marginal perforation, that is, the cartilage graft was placed medial to the remnant TM and posterior annulus, the perichondrium was placed lateral to the EAC skin and medial to the remnant TM. The possible concern is EAC cholesteatoma. However, previous studies showed that the perichondrium overlay the epithelium of the remnant TM did not induce the graft cholesteatoma.8-11 The objective of this study was to evaluate the graft success rate and hearing gain of endoscopic cartilage myringoplasty with preserving EAC skin for posterior marginal perforation.
Materials and Methods
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethical Review Board of the First Affiliated Hospital of Ningbo University, Zhejiang, China. Informed consent was obtained from all participants.
Materials
This was a prospective case series study of consecutive adult patients diagnosed with chronic posterior marginal perforation who visited the Department of Otorhinolaryngology, Head and Neck Surgery. The inclusion criteria were posterior marginal perforations with mucosal chronic otitis media, no suspicion of an ossicular chain defect, conductive hearing loss no greater than 40 dB in any frequency, and dry ears for at least 3 months prior to surgery. The exclusion criteria included ossicular chain abnormalities, suspected cholesteatoma, and the presence of fungal otitis externa. Preoperative temporal bone computed tomography (CT) was performed to exclude ossicular chain abnormalities and middle ear cholesteatoma. Perforation sizes were classified as subtotal (involving 50%-75% of the eardrum area), large (involving more than 50% of the eardrum area), and medium (involving 25%-50% of the eardrum area).
Audiometry was performed by an independent audiologist. Audiometric data were obtained preoperatively and at 12 months postoperatively. Pure-tone averages (PTAs) were calculated for both air conduction (AC) and bone conduction (BC) by averaging the thresholds at 500, 1000, 2000, and 3000 Hz; in most cases, a threshold of 4000 Hz was used to interpolate the threshold of 3000 Hz per the standards of the Hearing Committee of the American Academy of Otolaryngology—Head and Neck Surgery. Pre- and postoperative air bone gap (ABG) was calculated by subtracting the AC PTA from the BC PTA. ABG closure was calculated as preoperative ABG minus postoperative ABG.
Surgical Techniques
All the patients underwent endoscopic cartilage-perichondrium myringoplasty under total intravenous anesthesia. During surgery, patients were placed in the supine position with the head 30° up and oriented toward the opposite side with the video equipment placed on the opposite side of the surgeon. Raising tympanomeatal flap was not performed. Not any EAC incision was applied. The perforation margins and the annulus without remnant TM were not de-epithelialized. The epithelium was removed from the distal malleus handle if any.
A single-layer, perichondrial, composite cartilage graft was harvested from the ipsilateral tragus. The lateral perichondrium was peeled circumferentially, with pedicle attachment of the cartilage graft. The cartilage graft was shaped to be 1 mm larger than the perforation margins, with the perichondrium >1 to 2 mm larger than the cartilage graft. A channel for the malleus handle was made in the cartilage graft if any. The Biodegradable NasoPore material was placed dry in the middle ear but not saturated with any medications.
The cartilage graft was placed transperforation medial to the remnant TM and posterior annulus. The channel in the cartilage graft accommodated the malleus if any. The latter part of the perichondrium was directly placed lateral to the posterior annulus and the surface of the EAC skin; the rest part of the perichondrium was placed transperforation medial to the remnant TM but lateral to the cartilage (Figures 1 and 2).

Surgical schematic diagram. Cartilage-perichondrium graft harvesting (A), cartilage-perichondrium graft shaping (B), graft placement (C). Black indicated the annulus; red indicated the perforation. PE, perichondrium; CA, cartilage; HM, handle of malleus.
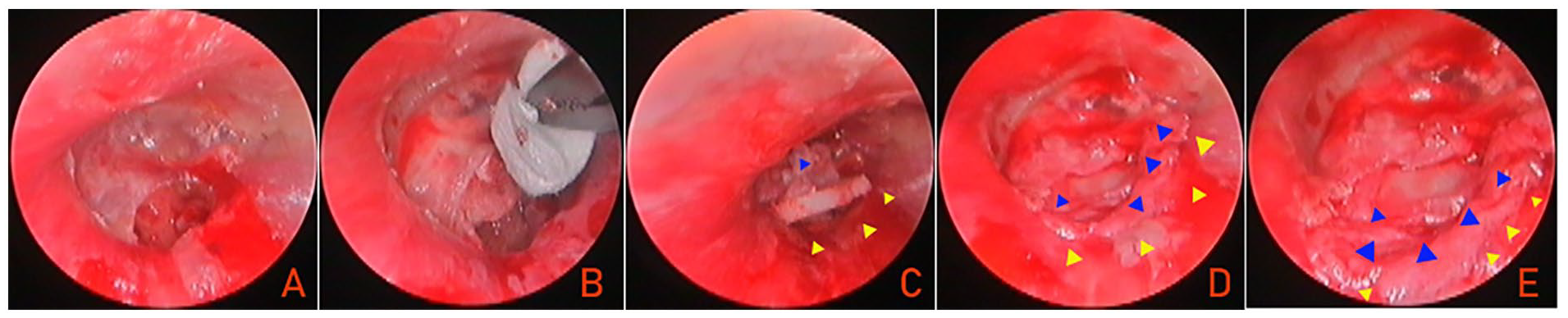
Surgical procedure. (A) Preoperative perforation margin; (B) middle ear packing; (C) graft placement; (D, E) graft completion. Blue triangle indicated the perichondrium graft; yellow triangle indicated the EAC skin. EAC, external auditory canal.
The EAC packing was not applied. The tragus incision was not sutured but pressured by gauze with antibiotic ointment, and a small dressing was applied to cover the auricle.
Postoperative Follow-Up
Patients were discharged the day after surgery. Postoperative endoscopic follow-up was scheduled at 1, 2, and 4 weeks and 6 and 12 months. An audiometric evaluation was performed at the 12 month examination. The operation time was defined as from anesthesia success to complete graft placement. Graft success was defined as the presence of an intact graft, and graft failure as the presence of residual perforation or reperforation after surgery. Postoperative success based on audiometric criteria included an ABG ≤ 20 dB.
Statistical Analyses
Statistical analyses were performed using SPSS Statistics (version 20; IBM Corp). The data are expressed as the mean ± standard deviation and number (percentage). Differences between the preoperative and the postoperative ABG were analyzed using a paired-samples t test. Differences with P < .05 were considered statistically significant.
Results
Demographic Data
The study population consisted of 36 patients with unilateral marginal perforation (19 males and 17 females; average age 47.2 ± 10.6 years), 22 patients had left side involvement, and 14 had right side involvement, and the mean duration of perforation was 11.3 ± 5.2 years. Perforations were medium in 7 (19.4%) patients, large in 26 (72.2%) patients, and subtotal in 3 (8.4%) patients. The mean operation time was 26.8 ± 5.1 minutes.
Endoscopic Observation and Graft Take Rate
The blood vessels of the remnant TM and flaccid part were dilated and congested at 1 to 2 weeks postoperatively. Subsequently, clinical inosculation of the perichondrium graft and remnant TM occurred at 2 to 3 weeks postoperatively. Simultaneously, neovascularization was initiated at the perichondrium graft margins or most of the perichondrium graft surface showed neovascularization. The perichondrium became clinically integrated with the EAC skin to the extent that the “border” was difficult to identify endoscopically at 2 to 3 weeks postoperatively (Figure 3).
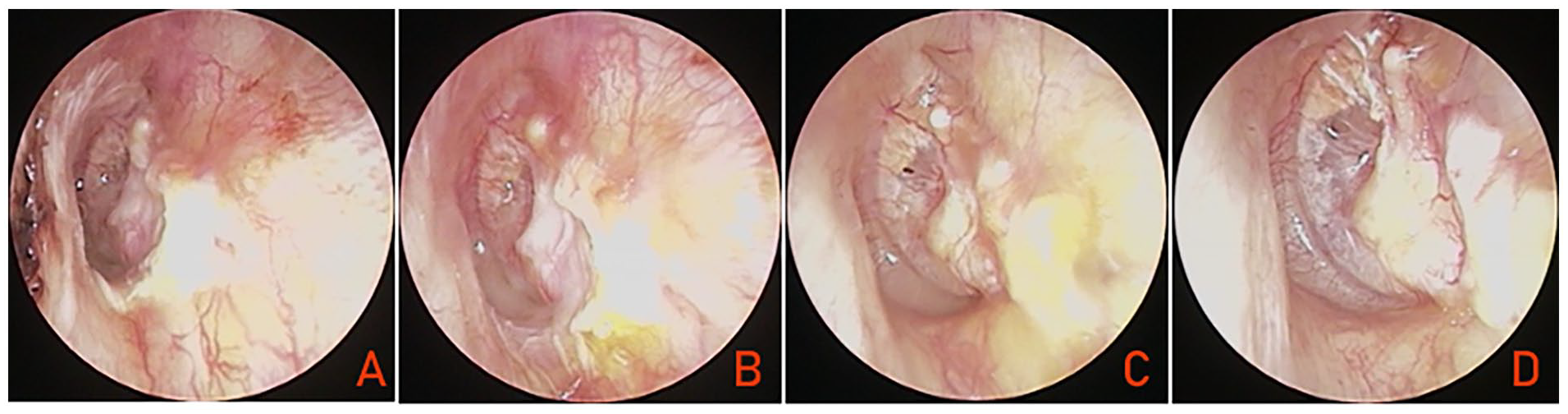
(A) At 1 week postoperatively; (B) at 10 days postoperatively; (C) at 4 weeks postoperatively; (D) at 6 weeks postoperatively. Figures 2 and 3 are the image of the same patient.
The tragal incision was closed completely in all patients. At 12 months, residual perforation was seen in inferior margin in one but reperforation was not. The graft success rate was 97.2% (35/36) (Figure 3).
Hearing Gain
Audiological testing was performed in the 36 patients at 12 months postoperatively and showed no sensorineural threshold shift. The mean preoperative ABG was 29.7 ± 3.8 dB, and the mean postoperative ABG at 12 months was 15.2 ± 3.1 dB; the difference between these values was significant (P < .05; paired-samples t test).
In the preoperative individuation audiometric assessment, the ABG was ≤10 dB in 5.6% (2/36), 10 to 20 dB in 58.3% (21/36), and 20 to 30 dB in 36.1% (13/36) of the patients. The individuation postoperative ABG was ≤10 dB in 52.8% (19/36), 10 to 20 dB in 38.9% (14/36), and 20 to 30 dB in 8.3% (3/36); the successful surgery rate (postoperative ABG ≤ 20 dB) was 91.7% (33/36).
Complications
There were no complications, such as iatrogenic sensorineural hearing loss, altered taste, vertigo, or tinnitus, during the follow-up period. There were no cases of graft lateralization, significant blunting, graft atelectasis, or graft adhesions, or effusion. No any intratympanic or EAC cholesteatoma was noted.
Discussion
Although the development of endoscopic myringoplasty, the repairing of posterior marginal perforation still required raising tympanomeatal flap via EAC incision to increase the graft stability and improve the graft survival rate, However, raising tympanomeatal flap is not only time-consuming but also easy to cause complications.1-6
In this study, we applied endoscopic cartilage underlay technique with preserving EAC skin for posterior marginal perforation. EAC skin incision and raising tympanomeatal flap were ignored in this study, the lateral perichondrium was peeled with pedicle attachment of the cartilage graft. Subsequently, the cartilage graft was placed medial to posterior annulus and the perichondrium was placed lateral to the posterior EAC skin. This technique has a shorter operative time and a similar graft success rate compared with raising a tympanomeatal flap technique reporting by literatures. The mean operation time was 26.8 minutes in this study. Saraf et al 12 reported the mean operation time of 36.83 minutes, Wang and Wang 13 43.89 minutes, Mahaseth et al 14 64.53 minutes, and Sun et al 15 42.4 minutes. In this study, the graft success rate was 97.2%. Cohen-Vaizer et al 16 reported a graft success rate of 92.4% for repairing marginal perforations. Gozeler and Sahin 9 94.9%, Bluher et al 17 94.2%, Lou 18 92.2%, and Tseng et al 19 93%. This technique was also comparable to butterfly myringoplasty by Alain et al (88%) 20 and our previous removal of a small rim of EAC technique for repairing marginal perforations (100%). 7
In this study, trimming perforation margin was not performed. Previous studies had demonstrated that preserving perforation margins did not affect the graft survival.21,22 On the contrary, preserving perforation margins increased the graft contact areas and thereby improved the graft success rate.21,22 The graft success depended on the graft survival, graft size, and postoperative infection. Postoperative infection was not found. Our endoscopic observations found that with the dilation of the blood vessels of the remnant TM, the perichondrium graft clinically fused with the remnant TM and neovascularization was initiated, thereby resulted in the graft survival.
The perichondrium became clinically integrated with the EAC skin to the extent that the “border” was difficult to identify endoscopically at 2 to 3 weeks postoperatively. Previous studies have shown that the use of a large perichondrial flap in contact with the vascular strip and undersurface of the TM preserves cartilage viability, 23 while the greater activity in the periphery may lead to early proliferation of blood vessels.23-25 The proliferation of blood vessels further provides nutrition for the EAC perichondrium.
Just as worries have been that the graft overlay the epithelium of the TM would induce the graft cholesteatoma, what is most worrying of the perichondrium graft overlay the EAC skin is EAC cholesteatoma. However, we did not find the EAC cholesteatoma. Recent some studies had proved that the graft overlay the epithelium of the TM did not increase the risk of the graft cholesteatoma.8-11 In addition, EAC cholesteatoma is instead seen in the raising tympanomeatal flap technique.1,2,26
EAC cholesteatoma is produced more often in the raising tympanomeatal flap technique due to the accumulation of EAC excretion caused by graft folds. 11 However, in this technique, the perichondrium graft overlay the EAC skin is smaller and only 1 to 2 mm, which is slight and insignificant compared with EAC area. EAC excretion can be discharged at will, it is not affected by the perichondrium. Previous studies reported that EAC cholesteatoma mainly occurred at postoperative 6 to 12 months,1,2,26 thus, 12 months follow-up is relatively adequate in this study. Even EAC cholesteatoma occurred, it may be observed and removed by endoscope in outpatient service. Although this technique has not yet been applied to other marginal perforations in this study, we speculate that it is also suitable for anterior and inferior marginal perforations.
The advantage of this study is that no patient was lost to follow-up from each group, thus supporting the results. In addition, the graft change may be clearly observed at different follow-up points by endoscope because of the absence of EAC packing of biodegradable synthetic polyurethane foam. The limitations of this study included the small sample size, short follow-up time (only 12 months), and no randomized controlled trial.
Conclusion
Endoscopic cartilage modified inlay technique with preserving EAC skin for repairing posterior marginal perforation is simple and minimally invasive technique, which had shorter operative time, similar graft success rate compared with raising a tympanomeatal flap techniques.
Footnotes
Author Contributions
C.L.: interpretation of data for the work, design of the work, analysis of data for the work, design and drafting the work, agreement to be accountable for all aspects of the work; final approval of the version to be published.
Data Availability Statements
All data generated or analyzed during this study are included in the published article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.