
Abstract
Introduction
Tympanic membrane perforations caused by trauma, infection, or sequelae of ventilation tube insertion are commonly encountered in ear-nose-and-throat (ENT) outpatients. ENT surgeons use paper patching, myringoplasty, or tympanoplasty to repair perforations. Myringoplasty is a simple technique used to repair uncomplicated small perforations. 1 Skin, perichondrium, a vein, temporalis fascia, and fat have been used to close tympanic membrane perforations; the most popular autograft is temporalis fascia. Fat-graft myringoplasty (FGM) affords many advantages compared to myringoplasty employing temporalis fascia: FGM is rapid, simple, cost-effective, minimally invasive, and an outpatient procedure. 2 FGM promotes tissue repair and revascularization; fat tissue contains angiogenic and growth factors and adipose-derived stem cells. In Korea, the indications for FGM include the absence of acute inflammation and middle ear discharge for at least 3 months, no evidence of perforation regeneration over this time, perforation size < 30%, air-bone gap (ABG) < 30 dB, and no evidence of cholesteatoma. 3 However, the factors that may affect FGM outcomes remain unclear. We thus evaluated the closure rates of perforations differing in terms of size and location, and the effects of patient factors and surgical technique.
Materials and methods
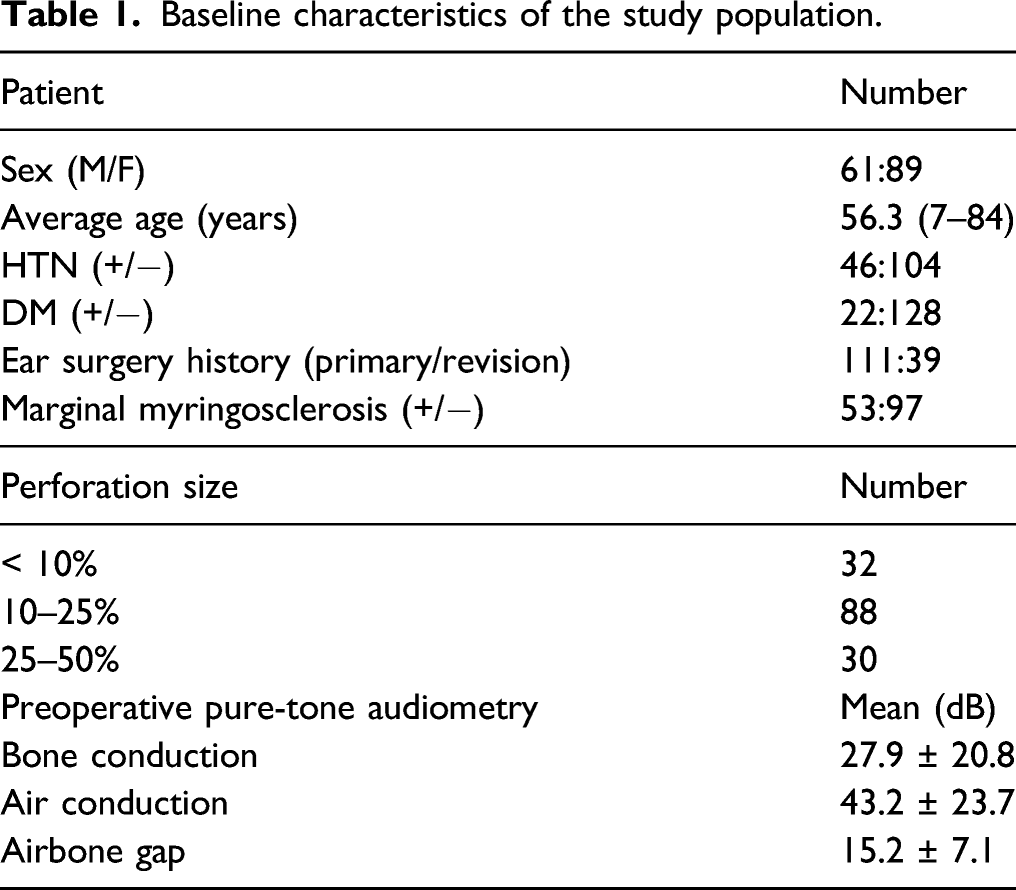
We retrospectively studied patients with tympanic membrane perforations who underwent FGM from March 2015 to March 2019. All procedures were performed by a single senior surgeon at our tertiary hospital. We included patients with perforations at least 6 months in duration, a middle ear that had been dry for at least 3 months, an ABG < 30 dB, and no evidence of mastoiditis or cholesteatoma. Patients whose perforations involved over 50% of the tympanic membrane, and who had middle ear discharge, an ABG ≥ 30, and a negative Valsalva test were excluded. A total of 150 patients (61 males and 89 females; mean age: 56.3 years) were enrolled and followed up for at least 6 months after surgery. All underwent otoendoscopy, pure-tone audiometry (PTA), and medical history taking. All ages were recorded; all were screened in terms of hypertension, diabetes, any prior ear surgery, calcific plaques adjacent to the perforation, and perforation size and location. Surgical success was considered to be an intact epithelialized neodrum without any perforation or retraction.
Surgical technique
Fat tissue for myringoplasty was obtained from the earlobe on the same side as the operated ear. Lidocaine with 1:100,000 (w/w) epinephrine was infiltrated into the four quadrants of the osseocartilaginous junction of the external ear canal. The perforation margin was trimmed using a Rosen needle and removed with the aid of microforceps. Gelfoam soaked in ciprofloxacin and dexamethasone was inserted through the perforation into the middle ear. Fat tissue was then placed on the Gelfoam (covering the perforation) and shaped to resemble an hourglass (Figure 1). The external ear canal was packed with Gelfoam. (A) There was a small perforation near the annulus of anterior tympanic membrane. (B) The perforation margin was trimmed. Afterwards Gelfoam soaked in ciprofloxacin and dexamethasone was inserted via the perforation into the middle ear. (C) Fat tissue shaped like an hourglass was placed on the Gelfoam to cover the perforation.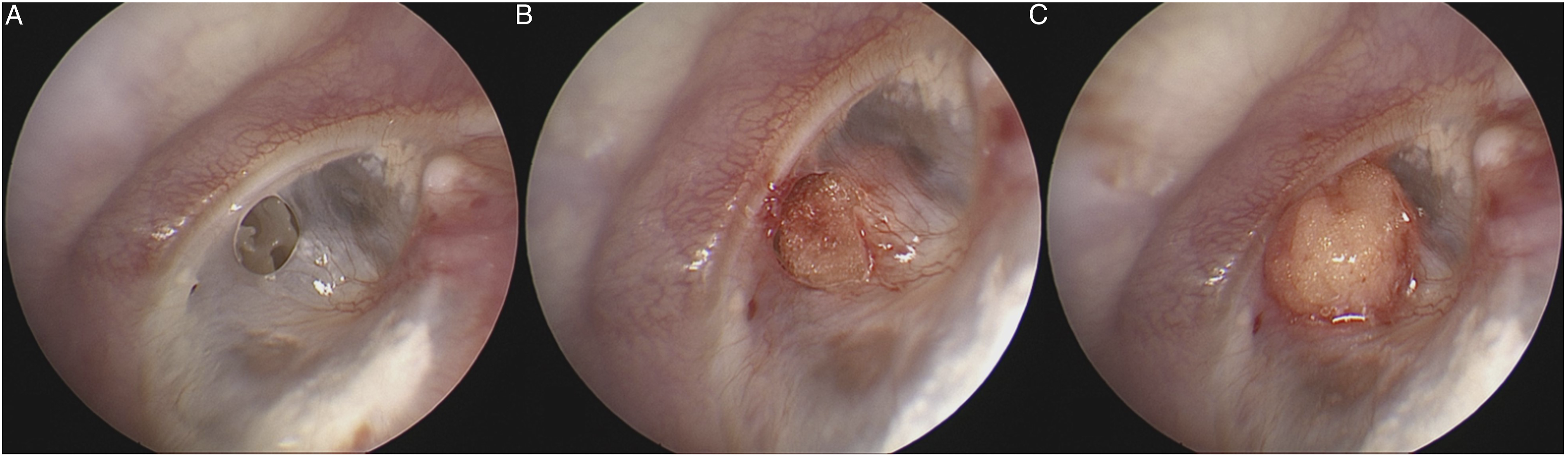
Statistical analysis
The Fisher exact test and one-way ANOVA were used to analyze the data (IBM SPSS Statistics ver. 20; IBM Corp., Armonk, NY, USA). A P-value < .05 was considered significant.
Ethics approval
This study was approved by the ethics committee of our hospital (IRB approval no. CNUH-2020-057).
Result
Baseline characteristics of the study population.
Outcomes
Success and failure rates according to the cause of tympanic perforation.

Perforation closure rate by patient factors.
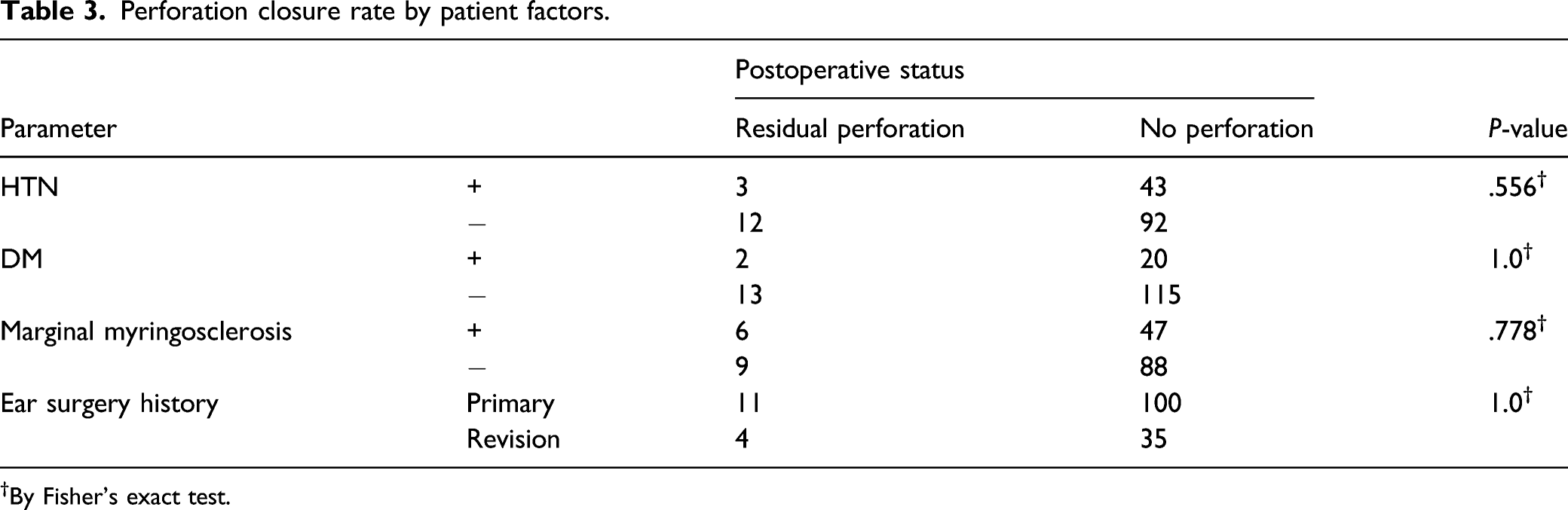
†By Fisher’s exact test.
Perforation closure rate by size, location, and age.
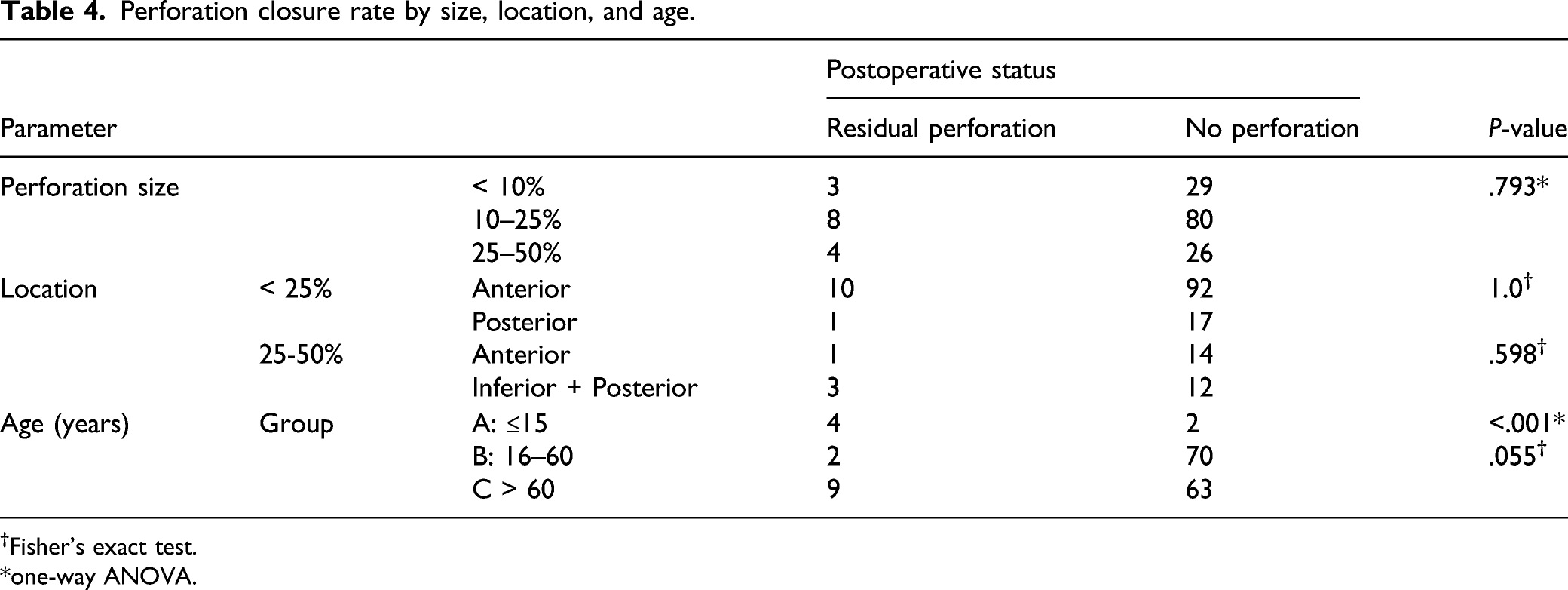
†Fisher’s exact test.
*one-way ANOVA.
Discussion
FGM was first introduced to close small perforations in 1962 by Ringenberg. 1 The reported success rates range from 76 to 92%.4,5 The success rate may improve if fat is combined with other material. Saliba et al 6 reported that the addition of hyaluronic acid to FGM increased the overall success rate to 90%. It was suggested that hyaluronic acid stimulated epithelial cell migration over fat tissue, preventing dehydration of the perforation margins. 7 Tolga et al 8 reported that the application of autologous platelet gel during FGM was associated with a higher success rate than FGM alone, particularly when the perforation was large. It was suggested that platelet-rich plasma accelerated TM perforation healing. We obtained similar surgical results by inserting Gelfoam soaked in ciprofloxacin and dexamethasone into the tympanum.
Antonelli et al 9 found that topical dexamethasone hindered TM healing in a chinchilla model of acute otitis media. However, Starkweather et al 10 suggested that intraoperative application of ciprofloxacin plus dexamethasone did not compromise tympanic membrane healing. Baklaci et al 11 showed that inflammation, adhesion, and new bone formation decreased when Gelfoam was used in conjunction with a steroid compared to Gelfoam alone. We believe that Gelfoam soaked in ciprofloxacin and dexamethasone increased the success rate of FGM by improving graft stability, and preventing retraction, and adhesion between the middle ear mucosa and adipose tissue.
Many studies have shown that larger perforations reduce the FGM success rate; one meta-analysis suggested that the figures 3 to 5 mm and 30% should serve as cutoffs, 12 but we disagree. Our success rate in the group with perforations of 25–50% was slightly lower than those of other groups, but statistical significance was not attained. We believe that insertion of Gelfoam in the tympanum may increase the success rate in patients with large tympanic membrane perforation.
Previous studies found that anterior tympanic membrane perforation closure rates after FGM were poor (with or without statistical significance) because of poor visibility of the anterior margin, inadequate graft support, and poor vascular supply.13,14 We found no significant difference in closure rate according to the location of tympanic membrane perforation. We believe that endoscopy was helpful in cases with limited microscopic visibility. Even if the ear canal is tortuous, narrow, and has a bony overhang, the endoscopic approach provides a wider and magnified view for entire tympanic membrane.
Most studies did not mention hypertension, diabetes, prior ear surgery, or myringosclerosis. Such factors might affect revascularization of the recipient bed, and would thus be negatively prognostic. We found that no such factor affected the success rate probably because adipose tissue can generate new microvessels and it expresses various growth factors.15,16 Adipose tissue is appropriate for TM perforation repair, supporting the growth of remnant tissue.
Older age may be associated with poorer surgical outcomes because of a poor vascular supply, underlying diseases, and reduced wound-healing ability. However, Ahn et al 17 reported that the rates of recurrence, reperforation, and healing did not differ between older and younger patients with chronic otitis media. We also found no significant difference in the FGM success rate between younger (aged 16–60 years) and older (aged > 60 years) patients. Moreover, FGM was successful in all nine patients aged over 80 years. Thus, older age did not compromise FGM outcomes.
Limitations
The success rate of our pediatric patients was poor (33%). This may reflect Eustachian tube dysfunction (which known as an important failure factor both myringoplasty and tympanoplasty). 18 The muscular opening of Eustachian tube is significantly poorer in children (particularly younger children) than adults. 19 Actually, five of six cases in pediatric group were patients with remnant perforation after ventilation tube insertion to treat persistent (> 3 months) otitis media with effusion. Also, children are more likely to develop colds or engage in vigorous exercise after surgery. Although the pediatric outcomes were significantly poorer than those of the other groups, we treated few pediatric patients. Unfortunately, we could not consider the effects of possible confounding factors such as chronic sinusitis, nasal allergy, and adenoidal status due to a lack of data.
Conclusion
FGM is a fast, safe, and efficient method for repairing TM perforation. The surgical outcome is not significantly affected by underlying disease, perforation size or location, or by the condition of the tympanic membrane or older age. However, it may be poor in children with dysfunctional Eustachian tube.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Technology development Program(S2972485) funded by the Ministry of SMEs and Startups and a grant (HCRI20015) Chonnam National University Hwasun Hospital Institute for Biomedical Science.