
Abstract
Introduction
Cartilage has become the main graft material for tympanic membrane (TM) reconstruction based on its advantages of hardness, good elasticity, and resistance to Eustachian tube dysfunction. It also allows a one-handed operation and easy placement during endoscopic tympanoplasty.1-4 Tos 1 proposed a useful classification of the cartilage types used in tympanoplasty. The most common types are cartilage island graft, 5 palisade cartilage,6,7 and a one-piece cartilage graft. 8 However, palisade cartilage usually requires uniform cartilage strips (6-8 palisades) to close a total perforation,1,9 with the drawbacks of a long preparation time, long placement time, and the inhibition of TM vibration.1,7,10 Consequently, the use of palisade cartilage in endoscopic tympanoplasty has been limited. As an alternative, the use of a broad cartilage palisades graft with only 2 or 3 palisades to cover the perforation has been proposed. 11 The objective of this study was to evaluate the graft outcome of endoscopic broad cartilage palisades graft, performed using the underlay technique, in the repair of subtotal perforations.
Materials and Methods
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethical Review Board of Yiwu Central Hospital in Yiwu, Zhejiang, China. Informed consent was obtained from all participants.
Methods
This was a prospective case series study of consecutive adult patients undergoing first-time surgery for chronic subtotal perforation from August 2019 to December 2021. The inclusion criteria were: subtotal perforation involving more than one-half and less than three-quarters of the eardrum; dry ear for at least 3 months prior to surgery, and good pneumatization of the middle ear and mastoid region, as shown by high-resolution computed tomography. The exclusion criteria were active inflammation during the 3 months prior to surgery, negative Valsalva maneuver, revision surgery, cholesteatoma, and conductive hearing loss >40 dB HL at any frequency.
Audiometry was performed by an independent audiologist. Audiometric data were obtained preoperatively and at 6 months postoperatively. Pure-tone averages (PTAs) were calculated for both air conduction (AC) and bone conduction (BC) by averaging the thresholds at 500, 1000, 2000, and 3000 Hz; in most cases, a threshold of 4000 Hz was used to interpolate the threshold of 3000 Hz, per the standards of the Hearing Committee of the American Academy of Otolaryngology—Head and Neck Surgery. The pre- and postoperative air-bone gap (ABG) was calculated by subtracting the AC PTA from the BC PTA. ABG closure was calculated as the preoperative ABG minus the postoperative ABG.
Surgical Technique
All patients underwent endoscopic palisade cartilage underlay myringoplasty without raising a tympanomeatal flap. The perforation margins were de-epithelialized. The epithelium, if any, was denuded off the malleus handle. However, the remnant TM was not elevated from the malleus handle. Tragal cartilage with a single layer of perichondrium was harvested from the ipsilateral tragus, after which the perichondrium was completely peeled off from the cartilage to form a free perichondrium graft and free cartilage graft. The latter was shaped based on the perforation size and was around 1 mm larger than the perforation margins; thinning of the cartilage graft was not performed. The cartilage graft was cut into 2 to 3 pieces of palisade cartilage based on the malleus handle. The graft was supported medially and laterally by biodegradable NasoPore.
The first piece of broad palisade cartilage was placed transperforation on the anterior side of the malleus handle, medial to the remnant TM and the annulus; the second piece was placed transperforation on the posterior side of the malleus handle, also medial to the remnant TM and the annulus (Figure 1); a third, small piece of palisade cartilage was used if a large gap was left between the 2 cartilage pieces (Figure 2). Finally, the free perichondrium was placed medial to the remnant TM, the malleus handle, and the annulus but lateral to the palisade cartilage graft.
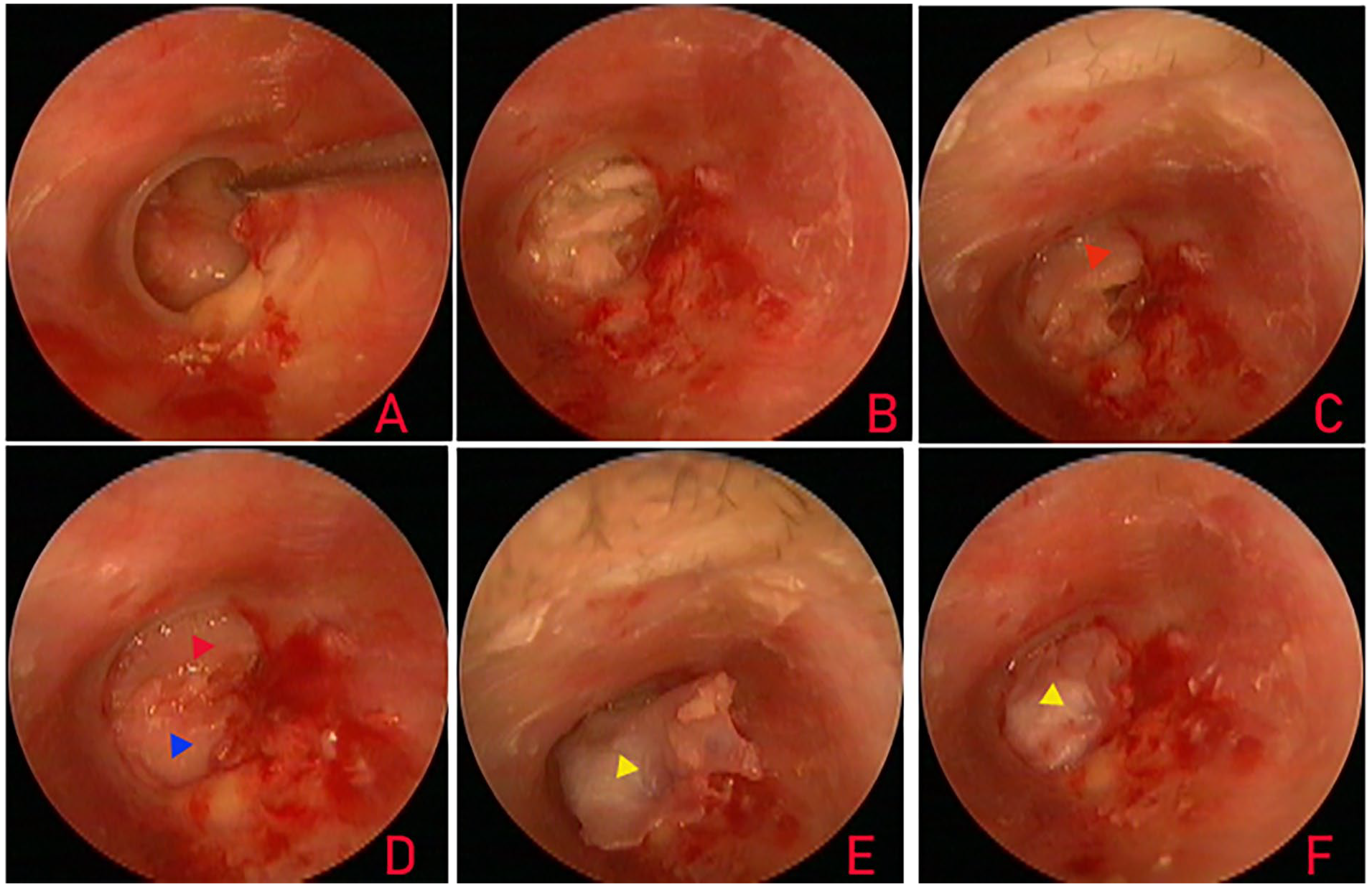
De-epithelialization of the perforation margin (A); middle ear packing (B); placement of the first piece (C, red triangle) and the second piece (D, blue triangle) of broad palisade cartilage; free perichondrium lateral to the palisade cartilage graft (E, yellow triangle) and perforation closure (F).
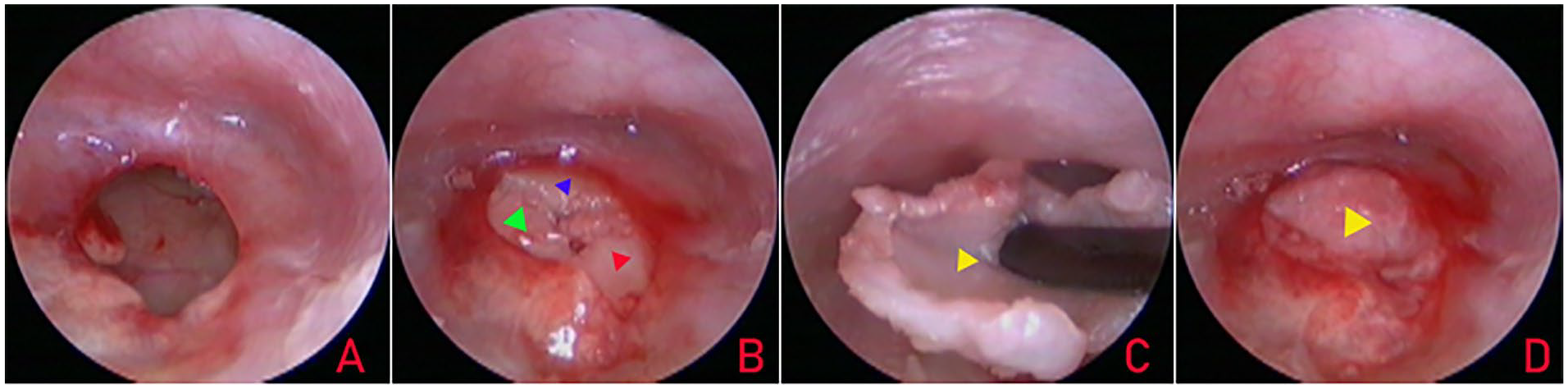
De-epithelialization of the perforation margin (A), the placement of 3 pieces of broad palisade cartilage (B, red, blue, and green triangles indicate placement of the first, second, and third piece of palisade cartilage, respectively), the free perichondrium lateral to the palisade cartilage graft (C, yellow triangle), and perforation closure (D).
Postoperative Follow-Up
Patients were discharged the day after surgery. Postoperative endoscopic follow-up was scheduled at 2 and 4 weeks and 3 and 6 months. An audiometric evaluation was performed at the 6 month examination. Graft success was defined as the presence of an intact graft, and graft failure as the presence of residual perforation or reperforation after surgery. Postoperative success based on audiometric criteria included an ABG ≤ 20 dB.
Statistical Analyses
Statistical analyses were performed using SPSS Statistics (version 20; IBM Corp). The data are expressed as the mean ± standard deviation and number (percentage). Differences between the preoperative and the postoperative ABG were analyzed using a paired samples t test. Differences with P < .05 were considered statistically significant.
Results
Demographic Data
The 43 patients (43 ears) comprising the study population included 28 (65.1%) females and 15 (34.9%) males. The mean age at surgery was 46.1 ± 3.8 years (range: 37-62 years). Surgery was performed on the left ear in 22 (51.2%) patients and the right ear in 21 (48.8%) patients. The mean duration of the perforation was 11.6 ± 2.5 years. All perforations resulted from chronic suppurative otitis media. No patient had concomitant disease. The mean operation time was 38.6 ± 7.4 minutes.
Graft Take Rate and Hearing Gain
Five (11.6%) patients were lost to follow-up, while 38 (88.4%) completed the 6 month follow-up. Residual perforation was determined in 2 (5.3%) patients and reperforation in 1 (2.6%). The graft success rate at 6 months postoperatively was thus 92.1% (35/38). The residual perforations occurred in the anteroinferior margin, and the reperforation was in the posteroinferior margin.
Audiological testing was performed in the 38 patients at 6 months postoperatively and showed no sensorineural threshold shift. The mean preoperative ABG was 28.4 ± 5.1 dB, and the mean postoperative ABG at 6 months was 13.6 ± 3.1 dB; the difference between these values was significant (P < .05; paired samples t test).
In the preoperative audiometric assessment, the ABG was ≤10 dB in 10.5% (4/38), 10 to 20 dB in 65.8% (25/38), and 20 to 30 dB in 23.7% (9/38) of the patients. The postoperative ABG was ≤10 dB in 68.4% (26/38), 10 to 20 dB in 21.1% (8/38), and 20 to 30 dB in 10.5% (4/38), The successful surgery rate (postoperative ABG ≤ 20 dB) was 89.5% (34/38).
Complications
No graft-related complications (eg, graft lateralization, significant blunting, graft medialization) were encountered during the follow-up period. None of the patients reported sensorineural hearing loss, facial nerve palsy, vertigo, or intractable tinnitus. No patient developed postoperative otitis media effusion. However, granular myringitis with minimal moistness but without infection occurred in 5.3% (2/38) of the patients.
Discussion
The cartilage graft has become the mainstream material for endoscopic TM reconstruction. In previous underlay graft techniques using cartilage palisades or strips, 6 to 8 palisades, each 0.5 to 3 mm wide, were applied in the repair of large perforations.1,9 The cartilage palisades were cut to form rectangles and placed close to each other, 9 whereas the cartilage strips were cut obliquely and placed like roof tiles. 12 The disadvantages of both included that they were time-consuming. Moreover, the use of several cartilage strips was shown to potentially suppress acoustic vibrations. 7
In the present study, subtotal perforation was repaired using the endoscopic underlay graft technique with only 2 to 3 broad cartilage palisades. In this approach, 2 broader pieces of palisade cartilage are placed on the anterior and posterior side, respectively, of the malleus handle and medial to the remnant TM and the annulus; the third, small piece of palisade cartilage is used only if a large gap is left between the 2 broad pieces. Free perichondrium is then placed medial to the remnant TM but lateral to the palisade cartilage graft. This technique shortens the cartilage palisade placement time compared to techniques requiring the placement of 4 to 6 cartilage strips6,12 or 6 to 8 palisades. 9 The present technique is similar to Sprekelsen and Barberán’s broad cartilage palisades technique, 11 in which 2 or 3 broad palisades are applied to repair a total perforation. The palisades are placed as underlay grafts.
The graft success rate in our study using broad palisade cartilage to repair subtotal perforation was 92.1%, consistent with previously published studies using palisade cartilage. Larrosa et al 6 reported a graft success rate of 85% using 4 to 6 pieces of cartilage. An anatomical graft success rate of 86.96% was reported by Li et al 13 compared with 95.7% in Kazikdas et al, 7 89.7% in Ciğer et al, 14 and 97% in Genç et al, 15 Our graft success rate was comparable to that using a one-piece composite cartilage-perichondrium graft or a cartilage island graft. Larrosa et al 6 reported a graft success rate of 86.3% using a one-piece cartilage graft. Gu 16 used a one-piece cartilage graft to treat subtotal perforation and achieved a graft success rate of 86.7%. Chen et al 17 also treated subtotal perforation, with a success rate of 92%. In this study, residual perforation occurred in the antero-inferior margins in 2 patients. The perforations may have been due to the formation of gaps in the cartilage placed in the antero-inferior annulus. In the patient with reperforation, although the free perichondrium closed the perforation early during the postoperative period, the cartilage palisades may have become displaced, causing rupture of the perichondrium and reperforation in the posteroinferior margin. Thus, the cartilage palisade must be large enough to completely underlay the anterior annulus.
A significant difference between the pre- and postoperative ABG was determined in our patients. As the broad palisade cartilage pieces support the perichondrium graft, which is placed on both sides of the malleus handle, vibration of the malleus handle is not affected. Some studies have in fact suggested that reducing the number of palisades from 6 to 3 to improves the acoustic properties.6,11 The perichondrium is placed medial to the malleus handle. In most cases, the healing TM loses the arc-shaped, protruding morphology resulting from the one-piece cartilage graft and reacquires its normal cone-shaped morphology, resulting in better hearing restoration.18,19 Leaving the TM attached to the malleus handle avoids potential trauma to the ossicular chain.20,21 Detachment of the TM may cause damage to the periosteal/perichondral vascular supply of the handle, including microtrauma. 22 In addition, unlike in our study, in most previous studies, the remnant TM was elevated from the malleus handle, and the perichondrium was placed lateral to the malleus handle.4,5,8 Vahidi et al 23 reported that placing the graft medial rather than lateral to the malleus handle resulted in better hearing restoration. Varma et al 24 found that an endoscopic broad palisade cartilage procedure yields audio outcomes similar to those achieved with a one-piece cartilage graft.
During the short follow-up time, no graft-related complications, including middle ear cholesteatoma, developed in our patients. Previous studies showed that placing the graft medial rather than lateral to the malleus handle can reduce the incidence of cholesteatoma.22,24 Leaving the TM attached to the malleus handle avoids the risk of cholesteatoma formation due to incomplete removal of the epithelium of the handle. 24 In a previous study, 30.95% of treated ears had residual epithelium over the umbo, seen on the histopathological examination, even after careful de-epithelialization. 22 In this study, graft lateralization did not occur because the graft was placed medial to the malleus handle. The supportive effect of the broad palisade cartilage was similar to that for a perichondrium graft and likewise avoided graft medialization. However, according to previous studies, push through using a one-piece cartilage graft could result in graft lateralization and medialization.7,9,17,18
A strength of our study was that only a few patients were lost to follow-up, while the limitations included the small sample size, the absence of a control group, the short follow-up time, the involvement of a single institution, and the possibility of bias due to a lack of blinding.
Conclusion
An endoscopic broad palisade cartilage graft that does not include raising a tympanomeatal flap provides a simple and feasible procedure for repairing subtotal perforations, with a high graft success rate and good hearing restoration.
Footnotes
Author’s Contribution
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.