
Abstract
Solitary bone plasmacytoma (SBP) is a rare hematological malignancy that usually occurs in the spine and rarely in the skull. It rarely presents in the skull base, but presenting symptoms are associated with cranial nerve involvement depending on the site of the disease. We present the case of a 61-year-old man with an unusual presentation of hoarseness secondary to vocal fold palsy. Imaging showed a large bony lesion in the temporo-occipital region with involvement of the jugular foramen. Further detailed diagnostic procedures confirmed SBP of the skull base. Radiotherapy was given with an uneventful recovery of vocal fold function. Skull base plasmacytoma can be considered as a differential diagnosis of causes of unilateral vocal fold palsy. Early therapeutic management may improve vocal fold function.
Introduction
Plasma cell tumors are characterized by a proliferation of monoclonal plasma cells and they can occur as multiple lesions, such as multiple myeloma (MM), or as a single lesion, such as a solitary plasmacytoma (SP). SPs, account for 5% of all plasma cell tumors, are rare hematological malignancies that grow within bone as a solitary bone plasmacytoma (SBP) or in soft tissue as a solitary extramedullary plasmacytoma (SEP), and they can disseminate to MM within 2 to 3 years or remain dormant.1-3
SBP, which is also known as osseous plasmacytoma, is more common in men, and the median age at diagnosis is 68 years. 4 The diagnostic criteria for SBP that distinguish it from MM include biopsy-proven tumor with evidence of clonal plasma cells, no other lytic lesions observed through imaging surveys, bone marrow without (or with less than 10%) clonal plasma cells, and no systemic involvement. 5 Radiotherapy (RT) is currently the mainstay of treatment for SP, with combined surgery as an option depending on tumor location. 1
More than 50% of SBPs occur in the spine, and they rarely occur in the skull. 6 However, plasmacytoma has been reported in the skull base (sphenoid, temporal, and occipital bones), and depending on the size and location of the tumor, the presenting symptoms include diplopia, hemianopia, blurred vision, hearing loss, vertigo, gait instability, and ptosis secondary to cranial nerve palsy.7-9 Herein, we described a rare case report of SBP in the temporo-occipital region presenting as hoarseness due to 10th cranial nerve (CNX) involvement.
Case Report
A 61-year-old man presented with progressive hoarseness and intermittent dizziness for 6 months, and dysphagia with easy choking for weeks. Laryngoscopy revealed a right vocal fold palsy with saliva pooling over the hypopharynx, but the rest of the head and neck examination was normal. Magnetic resonance imaging (MRI) showed a lobulated osteolytic lesion without a sclerotic rim (long axis measuring more than 6 cm) over the right occipital, temporal, and clivus bones, which was suggestive of plasmacytoma (Figure 1A). High-resolution of computed tomography (CT) imaging of the temporal bone was conducted to further evaluate the bony lesion (Figure 1B), and the patient underwent a CT-guided bony needle biopsy of this right temporo-occipital intramedullary mass (Figure 1C). The pathology showed plenty of discohesive medium-sized plasmacytoid cells with perinuclear halo aggregation (Figure 2A). These tumor cells were immunoreactive to CD138 (Figure 2B) with lambda light chain monoclonality (Figure 2C), but negative to kappa light chain and were not immunoreactive to CD3 and CD20, which indicated a plasma cell neoplasm. To exclude systemic MM, a whole-body positron emission tomography/CT scan was performed, and no other lesions were found. A bone marrow biopsy was conducted which indicated no myeloma involvement. Laboratory examinations revealed the following: red blood cell count 4.18 × 106/μL, hemoglobin 13.5 g/dL, white blood cell count 4.64 × 103/μL, platelets 139 × 103/μL, creatine 0.9 mg/dL, total serum protein 7.4 g/dL, albumin 4.0 g/dL, total calcium 8.8 mg/dL, and free calcium 4.93 mg/dL. Other serum electrolytes were also normal. Serum protein immunoelectrophoresis was conducted, with results indicating the following levels of immunoglobulins (Igs): IgG 1780 mg/dL, IgA 261 mg/dL, IgD <48 mg/dL, IgE 262 mg/dL, and IgM 103 mg/dL. Serum-free light chains of kappa and lambda were 32.43 and 97.81 mg/L, respectively. In accordance with the clinical manifestation, imaging results, lesion tissue-proven biopsy, and bone marrow biopsy, the patient was given a diagnosis of SBP of the skull base. The patient underwent definitive intensity-modulated RT to the involved field at a dose of 50.4 Gy in 28 fractions over a 6 week duration. At the post-RT 3 month follow-up, hoarseness was found to be relieved with movement of the right vocal cord. The patient demonstrated a partial response to RT with clinical recovery and residual SBP remained in skull base but without further radiographic progression in the following 3 years.
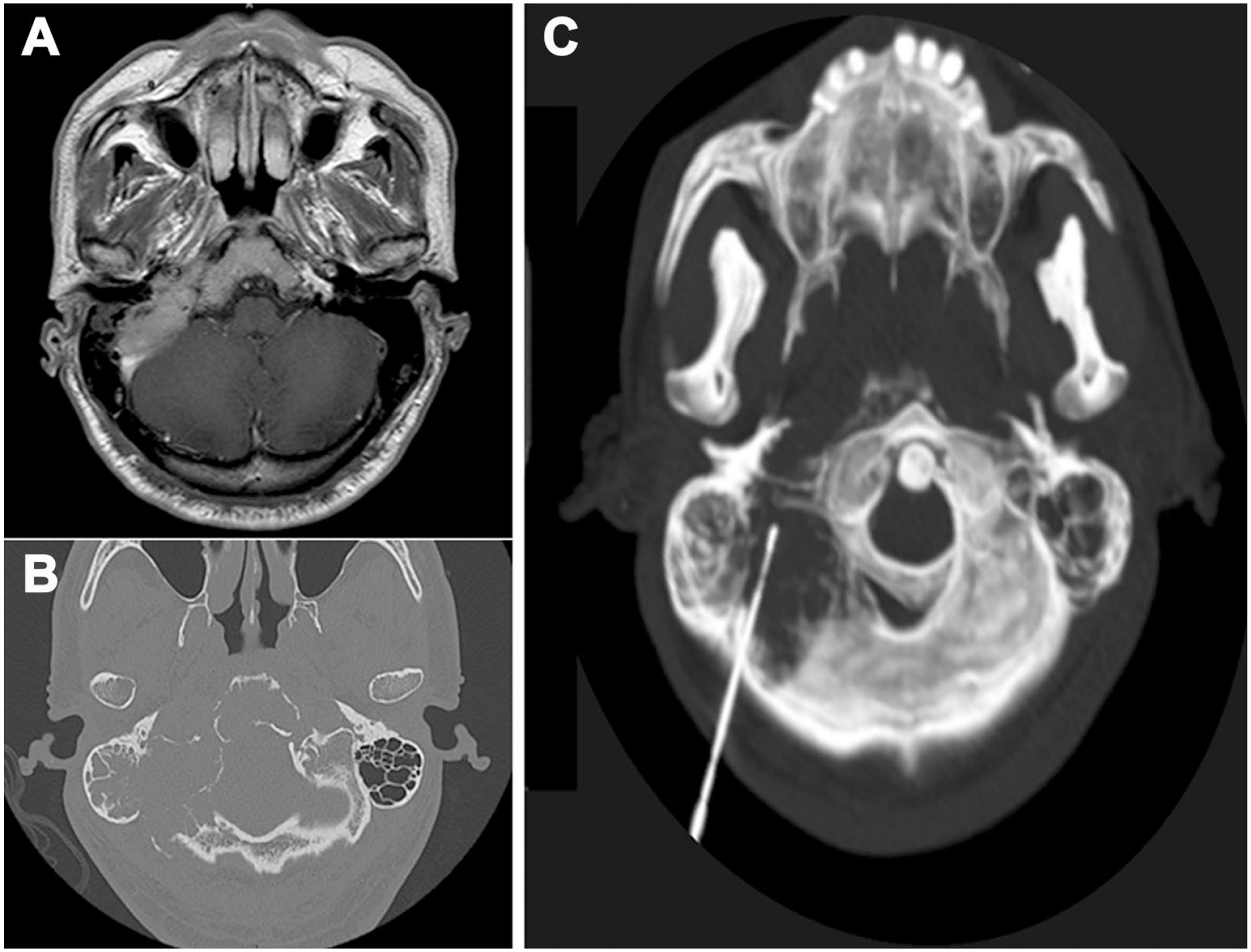
(A) Gd-enhanced T1-weighted MRI with homogenous contrast enhancement showing large lobulated tumor involving the right occipital bone, clivus, and temporal bone with bone erosion. (B) Temporal bone CT revealing lytic lesion involving the right mastoid air cells, occipital bone, and clivus with bony destruction. (C) 3D reconstruction of CT-guided core needle biopsy of intramedullary mass using a 17G coaxial needle and the introduction of an 18G soft tissue biopsy needle. MRI, magnetic resonance imaging; CT, computed tomography.
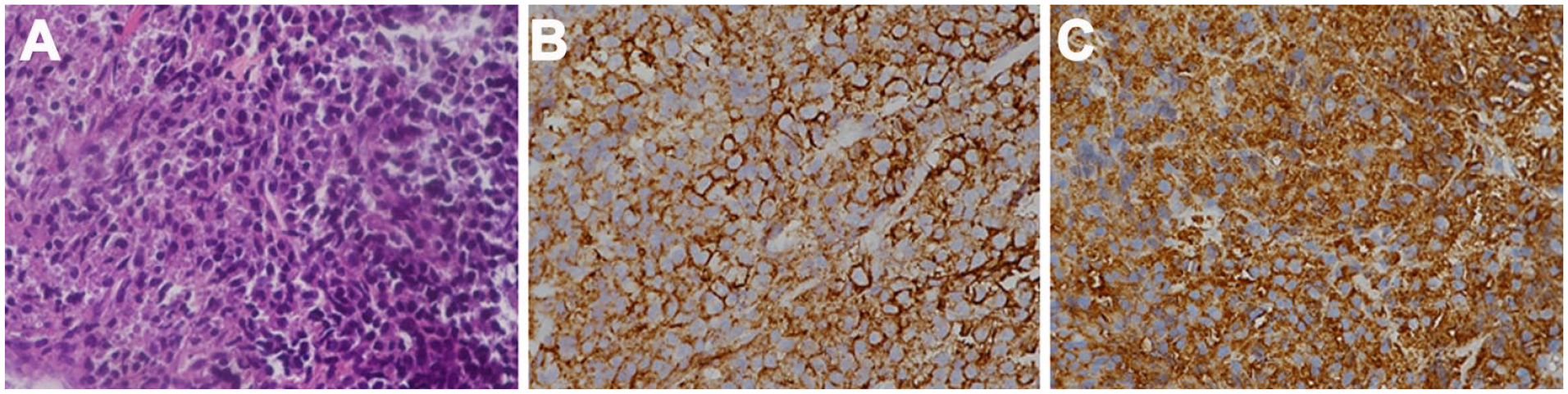
The images of histopathologic lesions (original magnification ×200) showing the following: (A) the aggregation of numerous plasmacytoid tumor cells with no specific arrangement pattern identified by hematoxylin and eosin staining. (B) Tumor cells exhibiting diffusely cytoplasmic immunoreactivity to CD138. (C) Tumor cells exhibiting diffusely cytoplasmic immunoreactivity to lambda light chain.
Discussion
SP, including SBP and SEP, is a rare plasma cell disease, with a cumulative incidence of 0.15 per 100,000 persons/year. 10 The occurrence of SP in the skull base is relatively rare, and SBP is extremely rare with few cases described in the literature. 11 While diagnosis includes imaging, a final diagnosis cannot be confirmed without final tissue proven. The differential diagnosis includes carcinoma of the nasopharynx, chordoma, meningioma, osteosarcoma, lymphoma, pituitary adenoma, metastatic carcinoma, eosinophilic granuloma, and MM. 12 In the case presented here, we conducted a CT-guided needle biopsy of the skull base lesion, and an adequate sample of tissue was obtained to confirm the diagnosis. This avoided any complications relating to open biopsy. 13
The symptoms of skull base SP relate to direct compression or involvement of the cranial nerves, both of which cause neurological symptoms. The most common nerve involvement is the sixth cranial nerve, followed by the second, fifth, seventh, and eighth cranial nerves. 12 However, vagus nerve involvement in SBP is rare, and the presenting symptom of hoarseness caused by the plasmacytoma has only been reported in 1 previous report. 14
The vagus nerve innervates the laryngopharynx and is involved in voice production. It exits the skull through the jugular foramen, which is formed anterolaterally by the petrous part of the temporal bone and posteromedially by the occipital bone. In the case presented here, involvement of the vagus nerve at this level caused vocal cord palsy and dysphagia. However, skull base tumors do not usually cause isolated hoarseness, as the vagus nerves also innervates the palate and pharynx. Moreover, the adjacent cranial nerves (glossopharyngeal and accessory nerves) leave the skull through the jugular foramen and can also be affected. For example, jugular foramen syndrome, also known as Vernet syndrome, causes paralysis of the 9th, 10th, and 11th cranial nerves traversing the jugular foramen. In the case presented here, jugular foramen syndrome could have developed if delayed diagnosis.
MM and plasmacytoma are 2 ends of the same disease spectrum, and both are characterized by the malignant proliferation of plasma cells. Because SBP may convert to MM, a complete and thorough workup is required to exclude MM prior to locally treating plasmacytoma. The number of lesions, bone marrow biopsy results showing less than 5% plasma cells, a monoclonal protein level less than 2 g/dL, the absence of Bence Jones proteins in the urine, no anemia or hypercalcemia, and normal renal function tests are all used to support the diagnosis of plasmacytoma. 12 By contrast, the characteristics of MM are bone marrow biopsy results showing more than 10% plasma cells, an M protein level greater than 3 g/dL, multiple lytic bone lesions, hypercalcemia, renal failure, and anemia (CRAB figures).5,12 Patients with no evidence of clonal bone plasma cells receive a diagnosis of SP, whereas those with limited clonal bone marrow plasma cells (<10% of marrow cellularity) receive a diagnosis of SP with minimal marrow involvement that has a greater probability of developing into MM. 11 Early diagnosis and periodic follow-up evaluations for local recurrence or development to MM are mandatory in patients with SBP.
As a highly radiosensitive disease, excellent local control rates (greater than 80%) can be achieved when treating SBP with RT alone. The mainstay treatment for MM is chemotherapy, whereas that of for SBP is RT, although surgical intervention may be required for bone instability or rapidly progressing neurological symptoms. 15 In patients with SP, 5 year local control rate is approximately 86% following definitive RT. 10 During the treatment course in our case, hoarseness was relieved with improved vocal fold function following the RT course. After definitive RT for 3 years, the lesion remained without further progression, and the patient demonstrated functional recovery with radiographic stable status to date.
Conclusion
This case illustrates an unusual presentation of SBP in the temporo-occipital region diagnosed with a CT-guided needle biopsy which avoid exploratory biopsy-related complications. SBP is uncommon in this anatomical location, and the incidence of jugular foramen involvement presenting as unilateral vocal cord palsy has only ever been presented in our case study. Therefore, early recognition and therapeutic management may result in the recovery of vocal fold function and positive outcome without disease progression.
Supplemental Material
sj-tif-1-ear-10.1177_01455613241249039 – Supplemental material for Solitary Bone Plasmacytoma of the Skull Base With an Unusual Presentation
Supplemental material, sj-tif-1-ear-10.1177_01455613241249039 for Solitary Bone Plasmacytoma of the Skull Base With an Unusual Presentation by Tien-Ru Huang, Chun-Shu Lin and Hsin-Chien Chen in Ear, Nose & Throat Journal
Footnotes
Data Availability
All data generated or analyzed during this study are included in the published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by grants from the Tri-Service General Hospital (TSGH-A-113006 to Hsin-Chien Chen).
Ethics Approval
This case report was approved by Institutional Review Board of Tri-Service General Hospital for Biomedical Research (TSGHIRB No.: C202215124). The authors have obtained the prior informed consent from the patient for use of images, medical information, and video.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.