
Abstract
We report a case of primary temporal bone diffuse B-cell non-Hodgkin lymphoma, which is a rare entity. A 71-year-old male with a history of dementia and hemicraniectomy presented due to 1 month of a pronounced left ulcerative mastoid lesion. Strikingly, there were no cranial nerve deficits which was unexpected due to the degree of the lesion. Initially, infectious mastoiditis was suspected based on physical examination alone. Due to the patient being a poor historian, it was difficult to determine whether this was an acute or chronic issue. Temporal bone squamous cell carcinoma, infectious mastoiditis, and actinomycosis were on the differential, but biopsies revealed non-Hodgkin lymphoma.
Introduction
Primary head and neck extranodal non-Hodgkin’s lymphoma (NHL) comprise 4% to 5% of all extranodal NHL’s. Furthermore, NHL represents only 3% of all malignant bone tumors, and is even more rarely discovered in the skull base. 1 Although reports of primary skull base lymphoma (PSBL) have begun to better understand this rare entity, less than 10% are discovered in the temporal bone. 2 Without a previous history of lymphoma, PSBL can mimic infectious, malignant, or autoimmune entities. 2 Herein, we report a rare case of PSBL with an impressive clinical presentation and noteworthy differential diagnosis.
Case Report
A 71-year-old male presented with a left neck and mastoid lesion. In addition to prostate cancer, hepatitis C virus (HCV), and well-controlled type II diabetes, the patient had aphasia and right hemiparesis after traumatic brain injury requiring left hemicraniectomy 9 years prior. His caregiver reported that a small bump appeared behind his left ear 1 month before presentation. The area became swollen and erythematous until the skin eventually ruptured and drained serous fluid. Upon presentation, the patient was afebrile with normal vital signs. Physical examination revealed a protruding left auricle with stenotic left external ear canal (EAC) draining pus, and an ulcer over the left mastoid and upper neck measuring 3.0 × 2.0 cm (Figure 1). Neurological examination did not reveal any cranial nerve deficits. A wick was inserted into the EAC and ciprofloxacin and dexamethasone otic drops were initiated.

Patient with 4 cm × 3.5 cm necrotic lesion at left mastoid adjacent to angle of mandible. The auricle is edematous with a swollen external auditory canal and is displaced anteriorly.
Laboratory studies showed normoglycemia, no leukocytosis, however lactate dehydrogenase (LDH; 315 IU/L), C-reactive protein (44.0 mg/L), and erythrocyte sedimentation(SED) rate (65 mm/h) were elevated. Computed tomography scan of the temporal bone with contrast showed diffuse inflammation, a 5.0 × 7.8 × 5.5 cm area of necrotic tissue versus abscess, complete obliteration of the EAC, opacified middle ear cavity, bony erosion of the tegmen, and coalescence of the mastoid air cells (Figure 2). The otolaryngology service was subsequently consulted for diagnosis of acute mastoiditis.
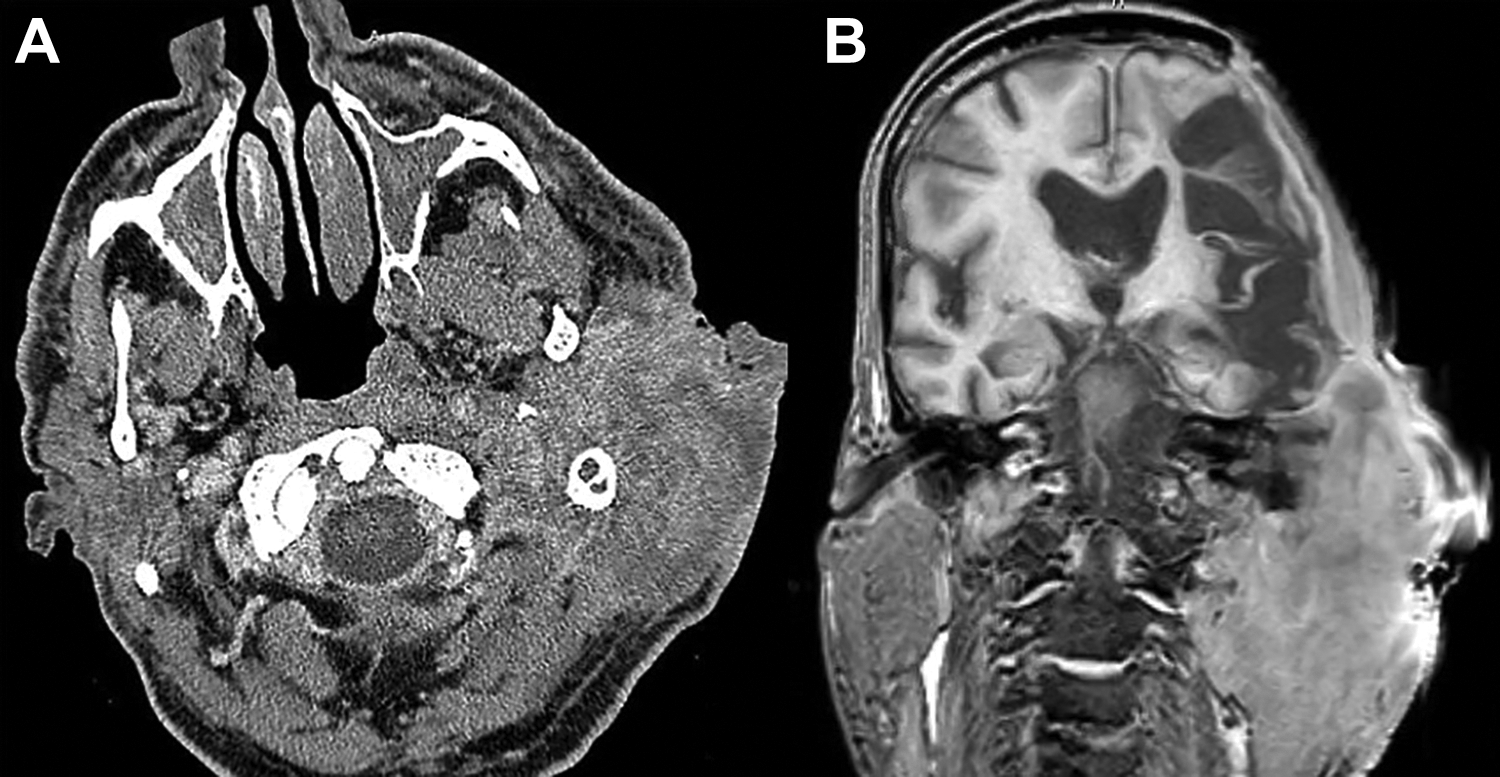
A, Axial computed tomography (CT) soft tissue displaying left large soft tissue mass. B, Magnetic resonance imaging (MRI) coronal section T1 with gadolinium displaying left mastoid opacification and erosion through mastoid tegmen and tegmen tympani.
The patient was begun empirically on cefepime, vancomycin, and metronidazole. Magnetic resonance imaging of the brain with contrast did not reveal intracranial extension (Figure 2). In the operating room, multiple biopsies and cultures were taken. Frozen section analysis suggested malignancy but was not definitive. Aerobic cultures grew Staphylococcus epidermidis and Enterococcus faecalis. Anaerobic cultures grew Actinomyces europaeus. Antibiotic therapy was transitioned to meropenem. Immunohistochemical stains of the biopsied tissue confirmed diffuse large B-cell lymphoma (DLBCL) positive for CD20, CD30, BCL-2, BCL-6, MuM-, and Ki-67. The patient was seen by the oncology service and scheduled for outpatient chemotherapy.
Discussion
Temporal bone malignancy is most commonly due to skin or parotid gland invasion rather than primary malignancy. Squamous cell carcinoma (SCC) accounts for 60% to 80% of temporal bone tumors. 3 In our patient’s case, SCC was considered most likely, although secondary invasion could not be excluded. Imaging was able to delineate the tumor and invasion into other structures including through the tegmen, consistent with a malignant destructive process such as SCC.
Given the extent of this patient’s disease, the absence of cranial neuropathies was striking. In a review of PSBLs, Marinelli et al reported the most common neuropathy was abducens nerve palsy. 2 Primary skull base lymphomas can also present with trigeminal hypoesthesia, headache, facial nerve weakness, and subjective hearing loss.
In light of the rapid evolution of symptoms, an infectious etiology was also considered likely. Actinomyces europeus was among the organisms cultured from the discharging ear and wound base and can present with craniofacial necrotic cutaneous lesions. McCann et al presented a rare case of actinomycosis of the anterior skull base and temporal bone requiring long-term intravenous antibiotics and multiple surgeries including maxillectomy, pterygopalatine fossa debridement, and radical mastoidectomy. 4 Actinomycosis presents in the cervicofacial region 55% of the time, including lesions located at or near the angle of the mandible. 4
Diffuse large B-cell lymphoma is an aggressive NHL, treated with combination chemotherapy depending on molecular subtyping. When performing a biopsy on PSBL’s, it is prudent to be aware of neurovascular structures while ensuring a generous specimen for subtyping. Additionally, timely surgical biopsy is crucial in patients with an acute cranial neuropathy being treating with systemic corticosteroids due to the potential for a lower diagnostic yield. 2
Hepatitis C virus has been associated with DLBCL. 5 As in our patient, HCV-positive patients with DLBCL are typically older, with higher incidence of extranodal involvement and elevated LDH. Although unconfirmed, an HCV-related antigenic process toward lymphoma progression has been suggested, similar to Helicobacter pylori in mucosa-associated lymphoid tissue. 5 Additionally, current data suggests HCV status does not impact treatment outcomes of DLBCL. 5
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.