
Abstract
Background:
Myeloma of laryngeal cartilage (MLC) is a rare plasma cell neoplasm which has not been well characterized. However, it is an important differential diagnosis of laryngeal cartilage mass as it can indicate the presence of underlying systemic hematological diseases, such as multiple myeloma (MM), that is associated with poor prognosis. This article is the first of its kind and aims to educate clinicians on future diagnosis and management of similar cases.
Methods:
Search of MLC was performed on the medical literature databases of Medline, PUBMED, and EMBASE. Additionally, institutional database at Gold Coast University Hospital Radiology Department was queried for relevant cases. Based on 16 cases that met the inclusion criteria, the etiology, epidemiology, clinical evaluation, investigations, management, and prognosis of MLC was summarized.
Results:
Of all, 94% of MLC occur in males and 81% in those older than 60 years. It is more commonly a manifestation of systemic MM, rather than localized extramedullary plasmacytoma (EMP), 81% and 19% respectively. Additionally, 67% of laryngeal EMPs progress to MM within 3 years from initial diagnosis. Although treatments involving both local and systemic therapy were effective at relieving local symptoms, 39% of MLC patients died during the follow-up period—all of which were due to septicemia caused by secondary infections.
Conclusion:
Myeloma of laryngeal cartilage is a relatively rare condition that requires accurate diagnosis in order to promptly manage the potentially underlying systemic hematological disease. Currently, more case reports and analytical studies are required to provide evidence-based guidance on etiology, diagnosis, and management of this condition.
Introduction
Laryngeal cancers account for 0.8% of all new cancer cases and is associated with huge psychosocial burden for patients due to their impact on activities of daily living including speech, swallow, and breathing. 1 Although the most common primary malignancy of a laryngeal cartilage mass is squamous cell carcinoma, approximately 80% of extramedullary plasmacytomas (EMPs) occurs in the head and neck region, thus making myeloma of laryngeal cartilage (MLC) an uncommon but important differential diagnosis that should be considered for new laryngeal cartilage lesions. 2
Plasma cell neoplasms (PCNs) are a group of hematological malignancies, including systemic multiple myeloma (MM) and localized solitary plasmacytoma, which accounts for 80% and 5% of all PCNs, respectively. 3,4 Solitary plasmacytoma can further be divided into EMP and solitary bony plasma (SBP) according to their site of occurrence: EMP occurring in soft tissues and SBP occurring in the bone marrow. In the absence of systemic disease, all hematological lesions arising in laryngeal cartilage are considered to be EMP. 5
Due to its localized nature, EMPs are associated with relatively better prognosis than MM, with most cases remaining free of further disease progression at 10 years. 6 The main diagnostic differentiation of EMP from MM is the lack of systemic manifestation of disease in EMP, as these 2 disease entities appear same on histology. 7 Since 20% to 30% of EMPs eventually progress to MM, 8,9 these conditions are often thought to be different stages of the same disease spectrum.
This article presents a review of 16 known MLC cases from 15 published articles 5,10 -23 (Table 1) and one case from institutional records. Since patient management, as well as prognosis, vary widely depending on different PCN entities, accurate diagnosis is vital for optimal management. 24 This article aims to educate, as well as to guide, clinicians on future diagnosis and management of similar cases.
Publications Analyzing MLC.
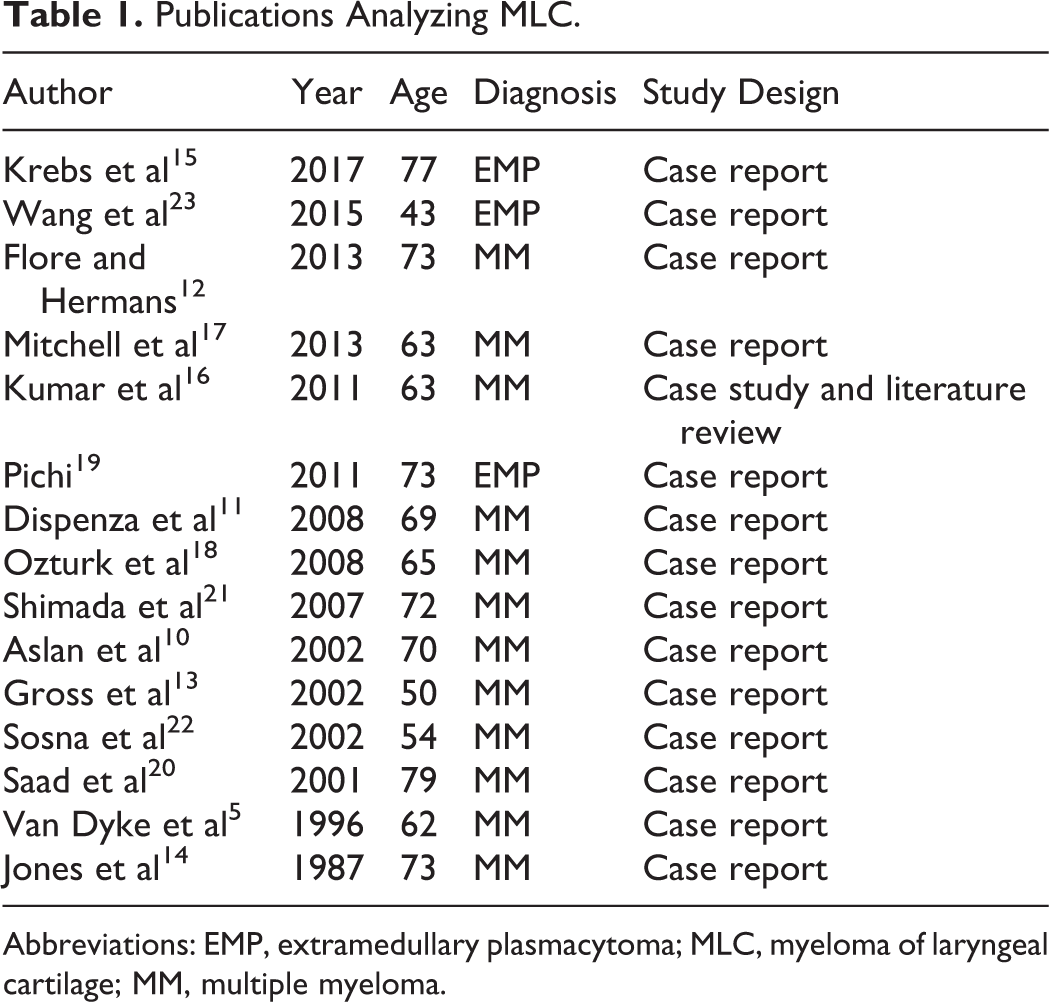
Abbreviations: EMP, extramedullary plasmacytoma; MLC, myeloma of laryngeal cartilage; MM, multiple myeloma.
Case Report
A 68-year-old male was referred to Gold Coast Hospital Radiology Department for a computed tomography (CT) of neck and thorax due to recent voice changes and possible neck mass. This was on background of kappa immunoglobulin G (κ IgG) MM that was in remission for past 11 years following successful treatment with 2 courses of bone marrow transplant and subsequent chemotherapy. There was no other significant past medication history. There was no significant social history, including alcohol or smoking history.
The CT showed a 6-cm soft tissue mass that was causing destruction of thyroid cartilage and invading into underlying left vocal cord and aryepiglottic fold. This mass was most likely to be a myelomatous deposit. Both cricoid cartilage and thyroid gland appeared to be normal. There were no obvious bony or lymphatic spread.
Ultrasound-guided fine needle aspiration and core biopsy of this hard mass from left thyroid laminar showed no malignant cells on cytology. However, on histopathology, findings of fibromuscular tissue infiltrated by sheets and nests of atypical plasmacytoid cells correlated with clinical diagnosis of MM.
Laboratory investigations were significant for low hemoglobin and low white cell count, with hypersegmented neutrophils present on blood film. Urinary Bence-Jones proteins and serum monoclonal proteins were detected. Raised κ IgG levels and low γ globulins were suggestive of progression of his previous MM. Beta-2 microglobulin levels were unremarkable.
Initially, he was started on intravenous (IV) chemotherapy; however, he was subsequently admitted to intensive care unit due to development of sepsis and acute renal failure. He was then changed to oral chemotherapy regime of Lenolidomide + dexamethasone administered 3 weeks on with 1 week off. He did not receive any local therapy to his laryngeal region.
Despite chemotherapy, he continued to deteriorate with symptomatic anemia, worsening renal functions, and peripheral neuropathy progressing from initial leg weakness, numbness of chin, to eventual development of acute ophthalmoparesis of cranial nerve III. By this stage, bone marrow biopsy confirmed the progression of his MM with heavy bone marrow involvement with 70% plasma cells.
His treatment was changed again to IV cyclophosphamide, velcade, dexamethasone (CVD) chemotherapy. However, after completing 3 of 4 cycles, the patient passed away due to sepsis and general deterioration. This was 1 year and 2 months after the diagnosis of myelomatous involvement of his thyroid cartilage.
Method
Medical databases of Medline, PUBMED, and EMBASE were searched for “Myeloma of Laryngeal Cartilage” and “Plasmacytoma of Laryngeal Cartilage.” These article abstracts were then assessed according to the inclusion criteria. Inclusion criteria included articles registered on medical databases specified above, published in English language, and cases where there were histological evidence for diagnosis of myeloma. For completeness, citations in all publications were also cross-referenced. Fifteen published articles, all case reports and one literature review, were yielded for analysis.
Separately, institutional database at Radiology Department of Gold Coast Hospital was also queried for cases of MLC. One case was found, and the patient data were added to the summary of cases from current literature. Consent was appropriately obtained to use this case as part of the review.
Therefore, total of 16 cases were analyzed to summarize the etiology, epidemiology, clinical evaluation, investigations, management, and prognosis of MLC.
Results
Etiology
Two main origins of MLC that are proposed in the literature are summarized below. Currently, both are widely accepted as the likely etiology. However, due to its rare nature, and consequently the lack of adequate control studies, the exact mechanism of MLC remains elusive. 5,25
Direct invasion by adjacent plasmacytoma
Myeloma of laryngeal cartilage arising from direct invasion of laryngeal cartilage by adjacent soft tissue EMP has been proposed by multiple authors. 5,16,25,26 This theory has been supported by radiological features of MLCs that indicate likely invasion of laryngeal cartilage from adjacent structures. 16,19,20
Gerry and Lentsch found that larynx is involved in 4.7% of head and neck EMP cases. 27 However, given that most EMPs are clinically silent and only found on postmortem autopsy, 16 this figure is likely to be an underestimate. To completely rule out adjacent EMP as the etiology, an autopsy of MLC patients, even those without clinically identifiable EMP, would need to be performed. Therefore, head and neck EMPs may be a more common etiology of MLC than expected.
Osseous metaplasia of cartilage into bone marrow
Second proposed mechanism is osseous metaplasia of cartilage resulting in formation of hematopoietic bone marrow within the laryngeal cartilage. Osseous metaplasia of cartilage is often found among elderly as part of normal aging process; however, they rarely involve myelomatous changes to become the site of abnormal plasma cell proliferation, such as in MLC. 5
This etiology was first supported by histopathology findings by Jones et al in 1987. 14 Since then, multiple radiological images characterized by thin and expanded cartilage lamina of laryngeal cartilage have also suggested a primary mass originating within the cartilage. 11,13,21 However, there have not been any further cases with histological confirmation of osseous metaplasia with myelomatous involvement. This may again be due to the rarity of these conditions or due to biopsies of insufficient depths that miss the osseous metaplasia center within the cartilage. 14,17 Therefore, more observational studies and case reports with biopsies of adequate depth are required to confirm this theory.
Epidemiology
The demographic information gathered is demonstrated below in Table 2. There was a clear elderly male predominance, with 94% (15/16) being male, and 81% (13/16) of cases being older than the age of 60. There was only one female reported among the cases analyzed. 11
Demographics of MLC Patients.
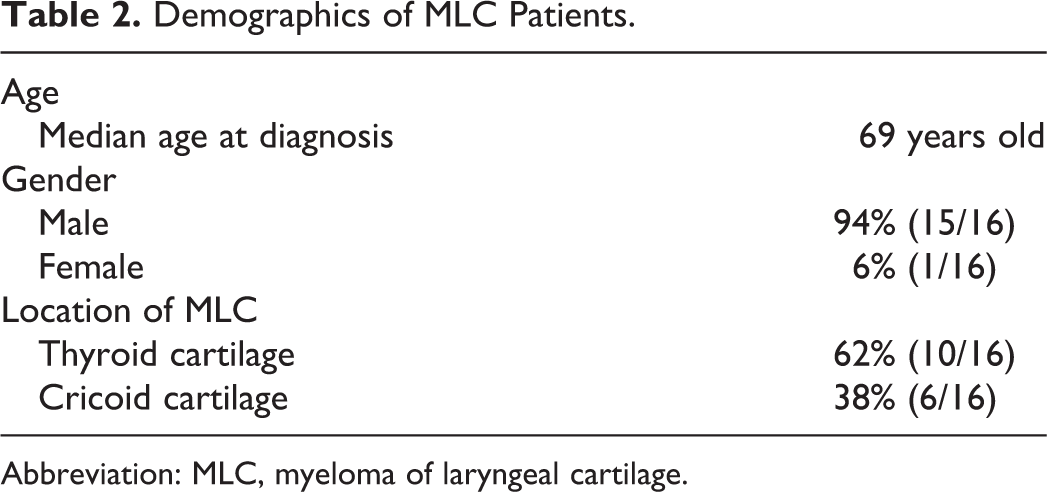
Abbreviation: MLC, myeloma of laryngeal cartilage.
Myeloma of laryngeal cartilages were more commonly encountered as a manifestation of MM (81%) as shown in Table 3. This could be due to the presence of systemic symptoms in MM that warrant more comprehensive investigation, thus increasing likelihood of detection compared to EMP. At the time of MLC diagnosis, 63% (5/8) of patients without previously known background of hematological malignancy were found to have MM. Although locations of affected cartilage were relatively evenly distributed between thyroid and cricoid cartilage (62% and 38%, respectively), all reported cases of EMP were found within the cricoid cartilage. 15,19,23 Two of the 3 EMP cases progressed to systemic disease (MM) within 3 years. 19,23
Characteristics of MM and EMP.
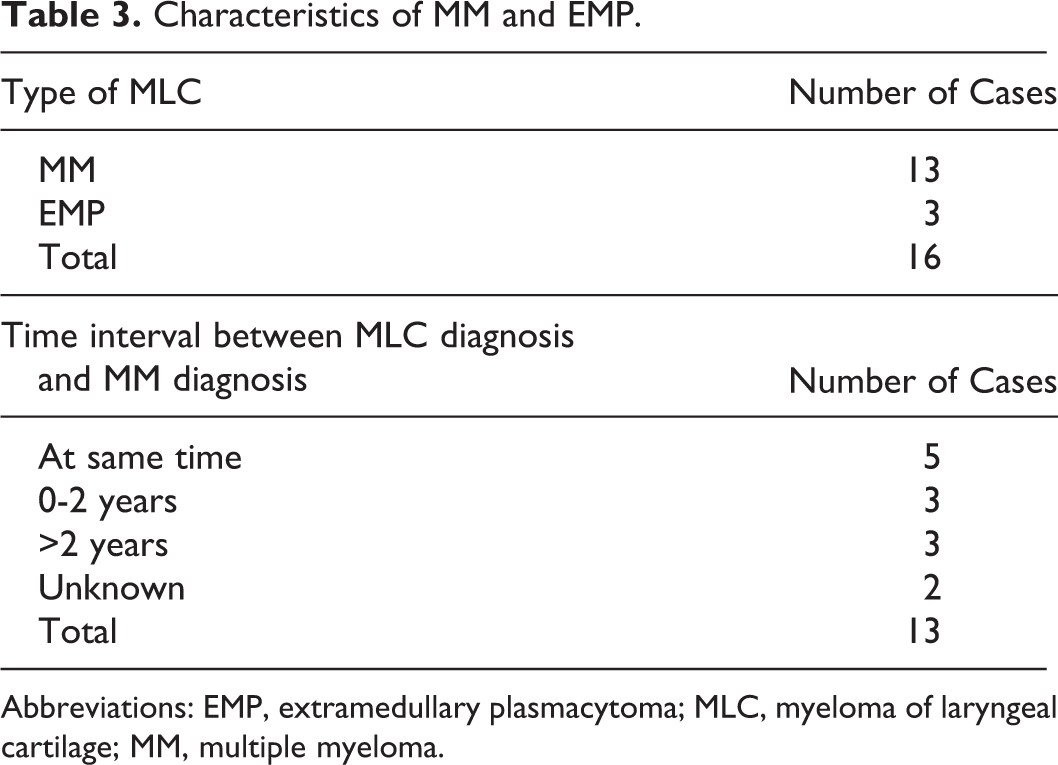
Abbreviations: EMP, extramedullary plasmacytoma; MLC, myeloma of laryngeal cartilage; MM, multiple myeloma.
Clinical Features
Main presenting symptoms were those resulting from progressive airway obstruction, including worsening dyspnea, stridor, hoarseness, and dysphagia. A palpable neck mass was reported in 38% (6/16) cases. 5,13,17,20,22 Rate of symptom development varied from progression over months to acute airway obstruction, with some cases requiring emergency interventions. 14,18,19,23 In one case, MLC was an incidental finding in an asymptomatic patient. 21
A common findings on indirect laryngoscopy included supra- or subglottic stenosis caused by a bulging mass. Where reported, mucosa overlying the mass was always normal in appearance. 5,10 -12,17 Additionally, ipsilateral vocal cord edema and palsy were also observed in some cases 4,7,9,20
Thus far in the literature, there have been no reports of lymph node involvement in MLC. In one case, 23 a possible malignant involvement of lymph nodes was suspected on CT; however, this was excluded on further investigation. There were no common risk factors of MLC that could be identified from this literature review.
Investigations
Being a localized disease, patients with EMPs have much better prognosis than their MM counterparts—with most causes of their mortality being unrelated to PCNs, 6 compared to MM which is associated with only 48.5% 5-year relative survival rate at diagnosis. 28 Since approach to patient management, as well as prognosis, vary widely depending on different PCN diagnosis, accurate diagnosis is vital. 24 All 3 areas of histology, radiology, and laboratory testing 8,26 need to be investigated before diagnosis can be made.
Radiological investigations
Computed tomography, with or without contrast, used to evaluate local extensions identified low-density masses 18,21 varying in size from 2 cm to 5 cm. 12,17 -20 They were often characterized by thin expansion of cortical cartilage 5,11,13,17,21 with presence of small punctate calcifications. 12,13,22 In some cases, invasion of adjacent structures were also observed. 16,20
On positron emission tomography (PET) scan, MLC showed increased fluorodeoxyglucose (FDG) and sodium fluoride (NaF) uptake, with relatively more intense increase in NaF uptake. 15,29 Positron emission tomography scan was also used to detect and screen for subsequent occult disease. 23 Oral et al proposed that F-NaF PET-CT may be superior to standard F-FDG PET-CT or CT studies in detecting small lesions due to its relatively higher sensitivity to lytic and early marrow-based metastatic changes. 29 However, there has not been any other case utilizing F-NaF PET-CT scans in the current literature. 29
Other radiological investigations used to screen for whole-body dissemination of disease include skeletal surveys using low-dose CT scans, plain radiographs, whole-body scintigraphy, and bone scans. 5,10,13,14,16,18,19,21 -23 Areas commonly involved in occult lytic lesions include vertebrae, ribs, skull, and sternum. 12 -14,16,18,21,22
Histopathological investigations
Histopathological diagnosis of PCN is made by presence of atypical plasma cells from either tissue biopsy 13,14,16,17,22 or cytology from a fine needle aspiration. 16,17 On immunohistochemical staining, MLC can be further categorized, as λ or κ restricting, according to the type of monoclonal antibody expansion. 10,13,15,17,19 Atypical plasma cells may also stain positive for cell marker CD138, CD56, CD79a. 15,17,19
In one case report by Jones et al, macroscopic signs of metaplastic ossification were identified through the presence of hemopoietic bone marrow within the laryngeal cartilage, thus providing support for etiological theory of cartilaginous metaplastic ossification. 14
Laboratory investigations
In all cases where MLC was the first presentation of disease, patients were worked up to exclude any systemic disease. As a result, 63% (5/8) of these cases were subsequently diagnosed with MM. 10,11,13,21,22
This workup included bone marrow biopsy, full blood count, blood chemistry including serum calcium and creatinine levels, and serum and/or urine monoclonal electrophoresis with evaluation for the presence of a monoclonal peak. 26
Treatment
Currently, there is no evidence for efficacy or superiority between different treatment methods. From the analyzed literature, the usual treatment approach comprises of providing local treatment with surgery or radiotherapy, and withholding systemic chemotherapy until fulminant systemic disease has ensued. No use of prophylactic systemic treatments have been reported in literature.
Localized treatment
According to the current literature, most patients are treated with radiotherapy for local manifestations, with 63% (10/16) patients undergoing fractionated radiotherapy to larynx and/or neck region. 10,12,13,15,17 -19,21,22,30 Administered radiation doses varied from 30 Gy to 50 Gy, with 2 cases requiring additional radiotherapy due to initial therapy being of inadequate dose to cause a reduction in mass size. 15,22
Two patients underwent definitive surgical management of en bloc resection, 16 and partial laryngectomy, 23 in both cases, no further local treatments were required.
Systemic treatment
Although chemotherapy was indicated in all MM involvement of laryngeal cartilage, it was only administered to 7 cases in the literature. 5,11,13,17,19,22,23 Reasons for withholding chemotherapy included patient refusal, 16,20 and unsuitable condition of patient for chemotherapy. 20,21 In one case, 10 diagnosis of early stage MM with 10% plasma cell infiltration of bone marrow favored a “watch-and-wait” approach of delaying chemotherapy until fulminant MM developed.
The chemotherapeutic agents used varied between different institutions. This was mostly based on preferences and clinical judgments of treating team, as there were no identifiable patterns or changes in prognosis associated with different agents. Agents that have been used include lenalidomide, 17 melphalan, 13,22 CVD, and VAD (vincristine, doxorubicin and dexamethasone). 11,13,22
Follow-Up
No regular pattern of follow-up was identified during the analysis of the current literature. All cases used a variation of all or some of the following intervals: 2 weeks, 1 month, 6 months, 12 months, and annual review up to 5 years after treatment is completed.
The method of monitoring also varied between laboratory investigations, clinical evaluation, and radiological imaging. There appears to be no current consensus on the best monitoring methods. Shimada et al described a follow-up regime of monthly blood examination and half-yearly CT scan until 3 years post completion of therapy. 21
Prognosis
Patients usually had good outcomes from local treatment, resulting in complete relief from symptoms associated with airway stenosis. To date, there has not been a reported case of recurrent MLC.
Of 16 cases, 6 (38%) patients died during follow-up—all due to septicemia caused by secondary infections. 10,13,16,19 However, due to the variation in follow-up regimens between institutions, exact mortality rate of MLC is unable to be determined.
Conclusion
Myeloma of laryngeal cartilage is a rare but important differential diagnosis for a laryngeal cartilage mass. This is especially the case in elderly males presenting with symptoms relating to airway obstruction. Although the currently proposed mechanisms of etiology are widely accepted by clinicians, more evidence is needed to confirm these theories. Myeloma of laryngeal cartilages can herald the presence of systemic disease, such as undiagnosed underlying MM, hence comprehensive workup using a combination of histopathology, radiology, and clinical evaluation is necessary to distinguish between different PCN entities. This may need to be repeated at regular intervals as up to 66% of laryngeals EMPs can eventually progress to MM. Due to the large institutional variations in treatment and follow-up regimes, more studies are needed to develop evidence-based protocols for managing practitioners.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.