
Abstract
Hairy polyps, considered a highly unusual congenital anomaly of the pharynx, are believed by many scholars to arise from the ectoderm and mesoderm during the embryonic stage. These growths often have a pear or sausage shape, are pedunculated, and their size ranges between 0.5 and 6 cm. They are typically grayish white or pink in color. This article discusses a 12-year-old female who had a growth at the Eustachian tube’s entrance on the left side of the nasopharyngeal wall, as identified by a computed tomography scan of the neck soft tissue; it was suspected to be a hairy polyp originating from the left Eustachian tube. The diagnosis of a hairy polyp was confirmed through pathology. The hairy polyp at the Eustachian tube, in this case, showed an irregular form with a wide base, making it look similar to an adenoid; thus, increasing the risk of it being misdiagnosed as residual adenoid tissue.
Introduction
Hairy polyps are a highly rare congenital anomaly of pharyngeal development, occurring mainly in newborns and infants. This condition is found more frequently in females than in males, with an extremely rare occurrence rate of less than 1 in 40,000 live births. The cause of hairy polyps is still not clear, although it is widely thought that they stem from the embryonic ectoderm and mesoderm. Usually, these polyps are pear-shaped or sausage-shaped with a pedunculated form and range in color from grayish white to pink. Their sizes vary between 0.5 and 6 cm. The case of the Eustachian tube hairy polyp discussed here is atypical due to its irregular shape and wide base, which resembles an adenoid closely. This distinct shape increases the likelihood of being mistakenly diagnosed as adenoid residual.
Case Presentation
A 12-year-old female patient was admitted to the hospital for ongoing nasal obstruction and purulent nasal discharge persisting over 3 years. Initially manifesting without a clear cause, these symptoms intermittently presented, often accompanied by snoring during sleep, though no sleep apnea episodes or excessive daytime sleepiness were reported. Despite a previous diagnosis of “chronic sinusitis and adenoid residual” at our facility and subsequent treatment with various medications, relief was not achieved. The symptoms were noted to exacerbate following a cold by the patient’s family. A reassessment in our outpatient department raised suspicions of a Eustachian tube obstruction, possibly from a hairy polyp, necessitating the patient’s admission. Furthermore, it was revealed that the patient had undergone surgery for the removal of a pharyngeal tumor at birth at another hospital due to respiratory difficulties. The family reported that the tumor was identified as a teratoma according to the pathology report from that surgery.
On admission, examination revealed that the patient’s ears and bilateral tympanic membranes were intact, and the external auditory canals were open. Nasal examination showed slight enlargement of the bilateral inferior turbinates and a minor deviation in the nasal septum. In the pharynx, a neoplastic protrusion with a smooth surface was observed on the left side of the soft palate on mouth opening.
Auxiliary examinations included an enhanced magnetic resonance imaging (MRI) of the nasopharynx, which identified a lesion on the left wall of the nasopharynx, indicative of a potential hairy polyp originating from the left Eustachian tube. Fluid accumulation in the left mastoid sinus and inflammation in the right maxillary and ethmoid sinuses were evident (Figure 1A). A temporal bone computed tomography (CT) scan with 3D reconstruction demonstrated a reduced air space within the left mastoid and an increased density in the mastoid air cells, tympanic cavity, and mastoid sinus. The ossicles appeared slightly irregular, but the internal auditory canal and external auditory canal were normal in size and density. No expansion of the cochlea was noted, and the temporal segment of the facial nerve canal showed no abnormalities. The opposite temporal bone appeared normal. The condition was diagnosed as chronic otitis media and mastoiditis (Figure 1B). In addition, a neck soft tissue CT scan with 3D reconstruction uncovered a lesion at the opening of the left Eustachian tube in the nasopharynx, raising suspicions of a hairy polyp originating from the left Eustachian tube, as the MRI scan had suggested. The scan also revealed dilation and air presence in the left Eustachian tube, alongside multiple enlarged cervical lymph nodes, slight enlargement of bilateral tonsils, and chronic left mastoiditis. An irregular bony protrusion was noted on the base of the left temporal bone (Figure 1C). Fiberoptic nasopharyngoscopy at our facility revealed a smooth-surfaced neoplastic protrusion on the dorsal side of the left soft palate, appearing to be connected to the left tonsil. The larynx exhibited no significant abnormalities, and vocal cord movements were normal (Figure 1D). A nasopharyngeal CT scan with 3D reconstruction and enhancement showed a mixed-density mass on the left nasopharyngeal wall, protruding into the nasopharyngeal cavity. This mass contained fat and soft tissue components with striated high-density shadows. Mild enhancement was observed with the contrast agent, causing compression and narrowing of the nasopharyngeal cavity. The bilateral oropharyngeal walls were slightly thickened, and multiple lymph nodes were present in the bilateral submandibular and carotid sheath areas. Fluid in the left mastoid and mucosal thickening in the right maxillary sinus were also noted. The contrast-enhanced scan showed mild enhancement of the mass, leading to compression and narrowing of the nasopharyngeal cavity. Slight thickening of the bilateral oropharyngeal walls was observed, along with multiple lymph nodes in the bilateral submandibular and carotid sheath areas. Fluid was present in the left mastoid, with mucosal thickening in the right maxillary sinus. In conclusion, a lesion suggestive of a potential hairy polyp was identified on the left nasopharyngeal wall, with clinical correlation advised. Thickening of the bilateral oropharyngeal walls and multiple lymph nodes in the bilateral submandibular and carotid sheath areas were noted, along with mucosal thickening in the right maxillary sinus (Figure 1E). Examination of the biopsy tissue from the left anterior skull base mass for salivary gland tissue, striated muscle, adipose tissue, squamous epithelium, and the presence of hair follicles and sebaceous glands under the epithelium was consistent with clinical findings of hairy polyps (Figure 2).
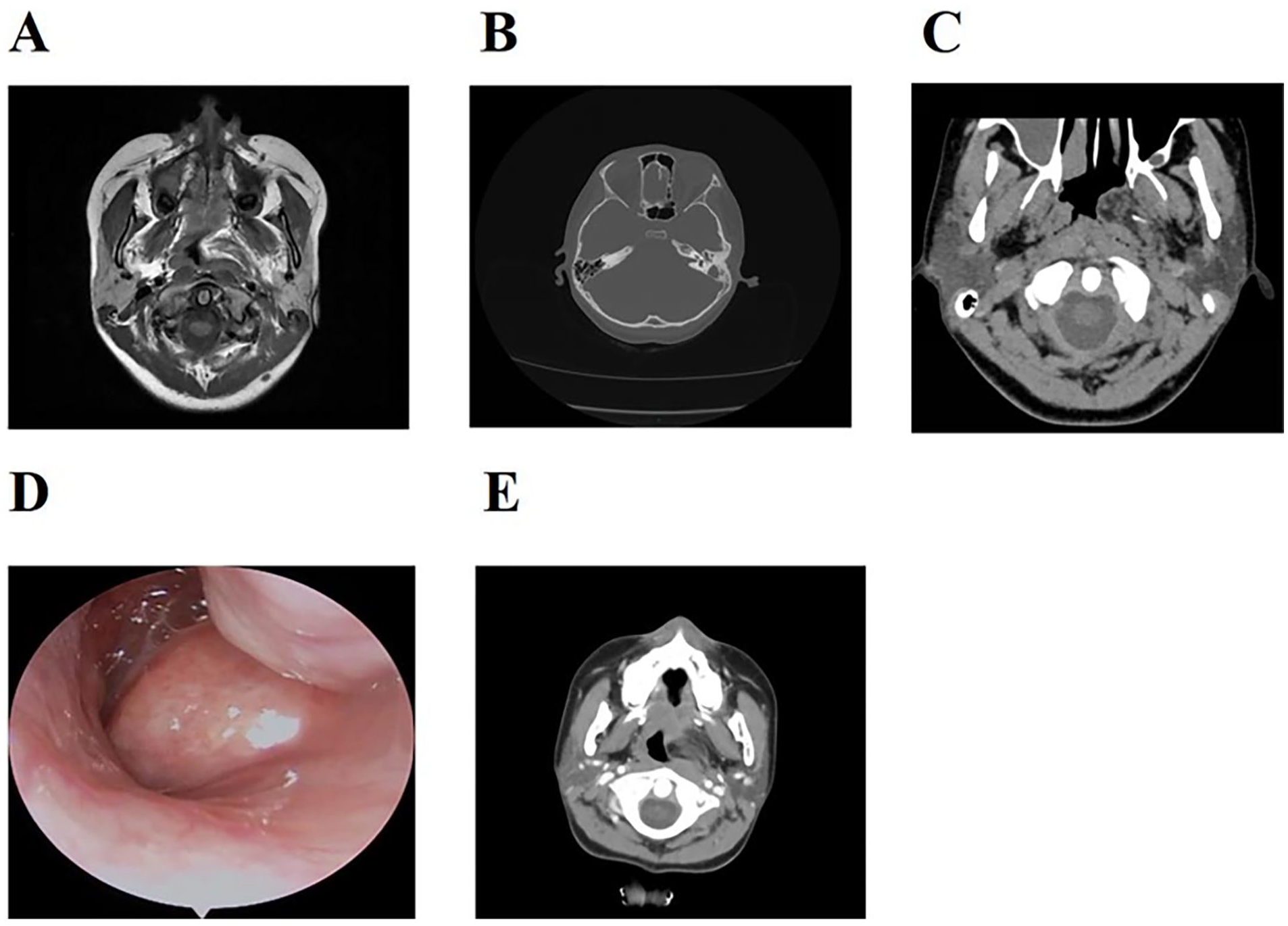
(A) A lesion on the left wall of the nasopharynx, suggestive of a possible hairy polyp originating from the left Eustachian tube. (B) The diagnosis was chronic otitis media and mastoiditis. (C) This lesion was suspected to be a hairy polyp originating from the left Eustachian tube, with the scan also indicating widening. (D) A smooth-surfaced neoplastic protrusion on the dorsal side of the left soft palate, appearing to be connected to the left tonsil. (E) A lesion on the left wall of the nasopharynx, suggesting a possible hairy polyp.
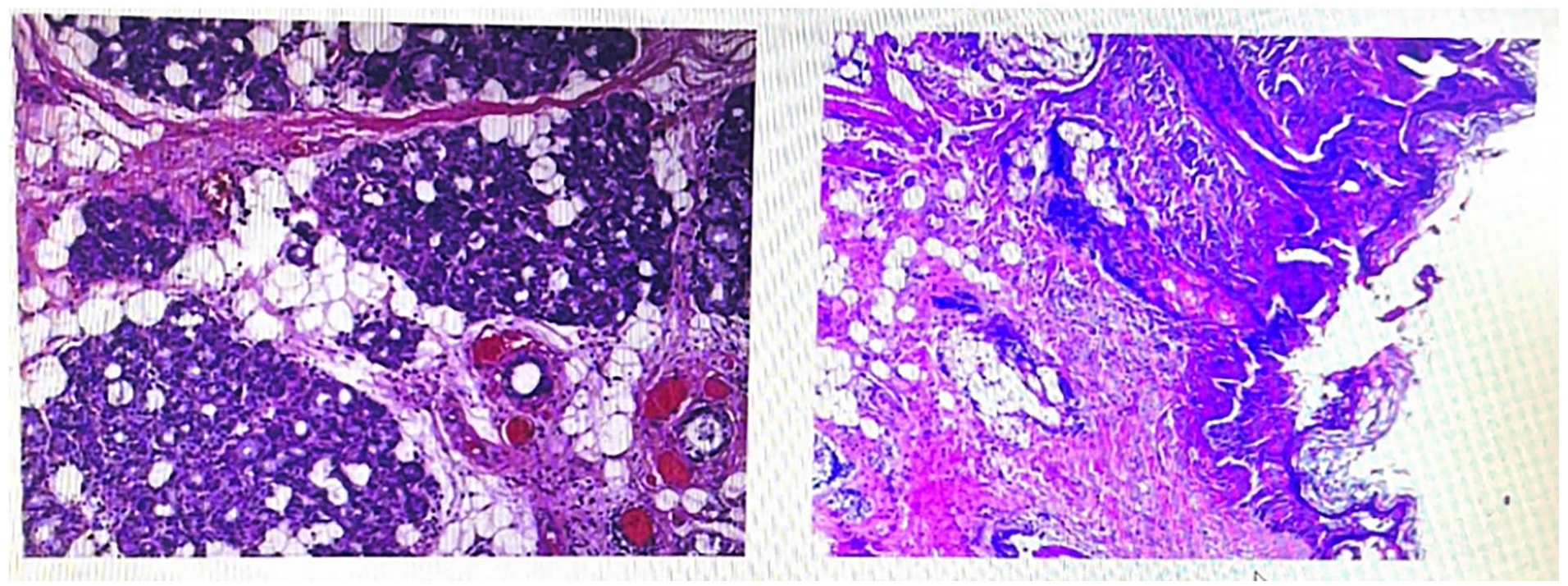
The biopsy tissue from the left anterior skull base mass was examined for salivary gland tissue, striated muscle, adipose tissue, squamous epithelium, and hair follicles and sebaceous glands under the epithelium, which could be consistent with clinical hairy polyps.
Preoperative diagnosis: (1) obstruction of the left Eustachian tube (possible hairy polyp); (2) chronic rhinosinusitis.
Surgical procedure: during the nasal endoscopy, a neoplastic protrusion was noted on the lateral wall of the left nasopharynx and the anterior area of the Eustachian tube. This growth extended from the skull base at the top of the nasopharynx to the upper portion of the tonsil, displaying smooth mucosa on the posterior wall of the nasopharynx. To enhance visibility of the lesion, a section of the left inferior turbinate was excised using a plasma knife. The mucosa surrounding the external edge of the neoplasm on the posterior lateral wall of the left nasal cavity was incised, allowing for simultaneous ablation and hemostasis. The tumor’s boundaries in the anterior and upper areas were excised, the pharyngeal cavity was accessed using a retractor, and the soft palate was drawn back with a catheter. The tumor’s boundaries in the anterior and lower areas were removed via the mouth, leading to a step-by-step complete excision of the neoplasm while preserving the normal muscle tissue and the anterior wall mucosa of the Eustachian tube. This was done to maintain the opening of the Eustachian tube and reduce the risk of adhesions. The tumor was carefully traced and excised up to the pterygoid process, with meticulous hemostasis ensured, concluding the surgery successfully.
Postoperative pathology: the biopsy tissue from the tumor at the left anterior cranial base included minor salivary gland tissue, striated muscle, and adipose tissue, with a covering of squamous epithelium. Beneath the epithelium, hair follicles, sebaceous glands, and other skin appendage structures were found, aligning with a diagnosis of a hairy polyp based on clinical correlation (Figure 2).
Postoperative diagnosis: (1) tumor at the left cranial base (Eustachian tube hairy polyp); (2) obstruction of the left Eustachian tube; (3) chronic rhinosinusitis.
Discussion
Hairy polyps are relatively uncommon benign congenital anomalies detected in infants and young children. These conditions are more frequently observed in newborns and infants, with a higher occurrence in females compared to males. This condition is considered rare, with an incidence rate of less than 1 in 40,000 live births. 1 The earliest documented mention of hairy polyps dates back to 1784, attributed to Koike and others. 2 Arnold, in 1870, was the first to describe hairy polyps in the nasopharynx and to differentiate them from teratomas, teratoid tumors, adenomas, and similar entities. 3 The classification of hairy polyps in scientific literature has been somewhat confusing, as they have been referred to as teratomas, hamartomas, dermoid cysts, and choristomas. There has been a discussion among researchers about distinguishing between teratomas and hairy polyps, as teratomas are characterized by their progressive growth and the potential for metastasis. 3 Most important, there have been no reported cases of malignant transformation in hairy polyps, and instances of recurrence after surgical removal are exceptionally rare. 4
The pathogenesis of hairy polyps remains unclear, although most theories propose that they originate from the embryonic ectoderm and mesoderm. 3 Schuring (1964) suggested that hairy polyps might develop from an accessory auricle originating from the first branchial arch. 5 This theory was strongly supported by Kanzaki et al (1988), who reported a case of a hairy polyp with a gross and histological appearance similar to that of an auricle. 6 Kelly offered an alternative theory, suggesting that the location of these lesions indicates their origin from the second branchial arch. 7
Histopathologically, hairy polyps consist of elements derived from both the mesoderm and ectoderm. The mesenchymal component frequently includes fat and cartilage, while the ectodermal component is characterized by keratinized squamous epithelium and appendage structures such as hair follicles, leading to the term “hairy polyp.” 8
Various congenital anomalies, including congenital left carotid artery occlusion, ankyloglossia, cleft palate, facial hemihypertrophy, and external ear anomalies, have been reported in association with nasopharyngeal hairy polyps. 9 However, none of these related issues were identified in the case discussed here.
Hairy polyps located in the external auditory canal and middle ear may lead to hearing loss, while those situated in the nasopharynx can cause symptoms such as nasal congestion and rhinorrhea. In the oropharynx, these conditions might result in respiratory distress and dysphagia. Typically, these polyps are pear- or sausage-like in shape, pedunculated, and vary in color from grayish white to pink. Their size ranges from 0.5 to 6 cm. 10 In this case, the Eustachian tube hairy polyp had an irregular shape with a broad base, closely resembling an adenoid, which significantly increased the risk of misdiagnosis as adenoid residual.
The initial misdiagnosis and overlooked diagnosis in this case can be ascribed to several factors: (1) the patient’s symptoms were atypical. Despite the presence of hairy polyps in the nasopharyngeal area and the Eustachian tube, no hearing changes were observed. (2) The primary complaints were nasal obstruction and rhinorrhea. These symptoms, coupled with the patient’s age and the growth location of the hairy polyp, led to confusion with adenoid hypertrophy, typically distinguishable via CT scans.
To avoid such misdiagnoses and overlooked diagnoses in the future, the following recommendations are proposed: (1) clinically, when encountering patients with abnormal nasopharyngeal protrusions, a biopsy should be performed under local anesthesia for further diagnosis. This method minimizes subjective errors influenced by various factors and ensures timely and appropriate auxiliary examinations and differential diagnosis. (2) Moreover, a detailed and comprehensive analysis of all auxiliary examination data should be conducted, including a review of the textual reports of these examinations.
Conclusion
This case report underscores the rarity of a misdiagnosed Eustachian tube hairy polyp and highlights the critical role of auxiliary examinations in the diagnostic process. It emphasizes the necessity for clinicians to conduct systematic and standardized initial assessments of patients, steering clear of biases based on subjective impressions. It is imperative for attending physicians to undertake relevant auxiliary examinations to accurately differentiate and swiftly exclude other conditions; thus, mitigating the risks of misdiagnosis, overlooked diagnoses, or more severe outcomes.
Footnotes
Acknowledgements
We would like to thank the Department of Otolaryngology, Affiliated Hospital of Zunyi Medical University, for my learning opportunities and platform and thank teachers Li Chunlei, Yang Tianwen, and Long Yilin for their guidance and help in my study. At the same time, I also thank Xu Wenbo and Tangliwen for helping me sort out the data.
Data Availability
All the data generated or analyzed during this study are included in this published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The study was reviewed and approved by the Ethics Committee of the Affiliated Hospital of Zunyi Medical University (KLL-2024-006).
Informed Consent
All participants gave their informed consent to participate.