
Abstract
Osteoblastoma is a typically noncancerous bone tumor commonly found in the spine and long bones of the arms and legs. It is exceedingly rare for this tumor to occur in the paranasal sinuses. We present a case of osteoblastoma in a 13-year-old boy affecting the ethmoid sinus, which manifested as exophthalmos. A computed tomography scan revealed an expansive lesion in the right ethmoid sinus, causing compression and displacement of the orbital contents to the right. The lesion exhibited a mix of ground glass opacity and dense bone. On magnetic resonance imaging, the less dense areas of the tumor showed strong enhancement, while the densely sclerotic regions appeared as signal voids on all imaging sequences. A combined transorbital and transnasal approach was performed to remove the tumor. Histologically, the tumor consisted expansile growth surrounded by a sclerotic rim of inter-anastomosing trabeculae of woven bone set within loose edematous fibrovascular stroma. This case highlights the unusual occurrence of osteoblastoma in the ethmoid sinus, a location seldom associated with this type of tumor, and adds to the existing literature on this topic and offers a new surgical approach to managing this entity.
Keywords
Introduction
Osteoblastoma was first described in 1932 when it was referred to as an “osteoblastic osteoid tissue-forming tumor” that arose in the fourth metacarpal bone. It is historically known as giant osteoid osteoma, calling to attention its histopathologic similarities to osteoid osteoma1,2 or as some authors have considered as an entity of variant expressions of the exact pathological mechanism; however, the new data and common opinions support that they are distinct pathological entities with varying clinical, radiological, and histopathological presentations.
The osteoblastoma prevalence is approximately 1% of all primary bone tumors.3,4 It was known as a benign bone tumor that most often occurs in the vertebral column, the long and small bones of the extremities (the hands and feet). Osteoblastoma is known previously to have a more male predominance. Its occurrence in the skull and jaw bones is considered relatively rare and represents only 15% of all osteoblastoma.5,6 Moreover, head and neck, maxilla, mandibular, orbital, and especially paranasal sinus involvement are very rare, with approximately 5 reported cases involving the frontal sinus, for example, and less than 10 cases reported to have affected the ethmoid solely and around 3 cases describing an ethmoid osteoblastoma with orbital involvement.7,8
A Case Report
We report an osteoblastoma of the ethmoid sinus in a 13-year-old male, a previously known carrier of sickle cell disease trait, came to our attention with a 2 month history of right eye exophthalmos with proptosis, headaches, and progressive sense of right-sided nasal obstruction. General physical examination and rigid nasal endoscopic examination did not demonstrate any abnormalities. Ophthalmological examination demonstrated ipsilateral visual acuity of 20/20, lateral displacement of the globe with no inferior displacement, full extraocular motion, and diplopia on right head tilt. The patient underwent computed tomography (CT) scan imaging study which demonstrated mixed osseous and ground glass density lesion occupying the right anterior ethmoid air cell executing its expansion and mass effect on the adjacent orbital structures (Figure 1A and B). Magnetic resonance imaging demonstrated evidence of moderate-sized expansile mixed signal intensity mass lesion seen within the right anterior ethmoid air cells and consists of soft tissue components dominating the medial aspect and curvilinear lateral osseous tissue. It causes a lateral temporal displacement of the right eye globe and corresponding structures, more pronounced at the medial rectus muscle without signal alteration. The soft tissue complement exhibits a low T1/T2 intensity and mixed flair signal intensity and partial medial rim enhancement on the postcontrast images, while the osseous component exhibits bone signal intensity in all sequences (Figure 1C and D). A combination of endoscopic endonasal technique with image guidance and a medial orbitotomy was chosen. The medial orbital wall was reconstructed using a polydioxanone plate. The orbital structures were preserved and a complete removal of the mass was accomplished. At gross examination, the lesion showed a red granular appearance with a thick shell-like bony component (Figure 2A). Microscopically, the tumor presented an anastomosing bony trabeculae rimmed with a single layer of osteoblasts (Figure 2B and C). The patient recovered well and was free of sinonasal or ocular symptoms, with no radiological evidence of recurrence at a 6 month follow-up visit (Figure 1E and F, Table 1).
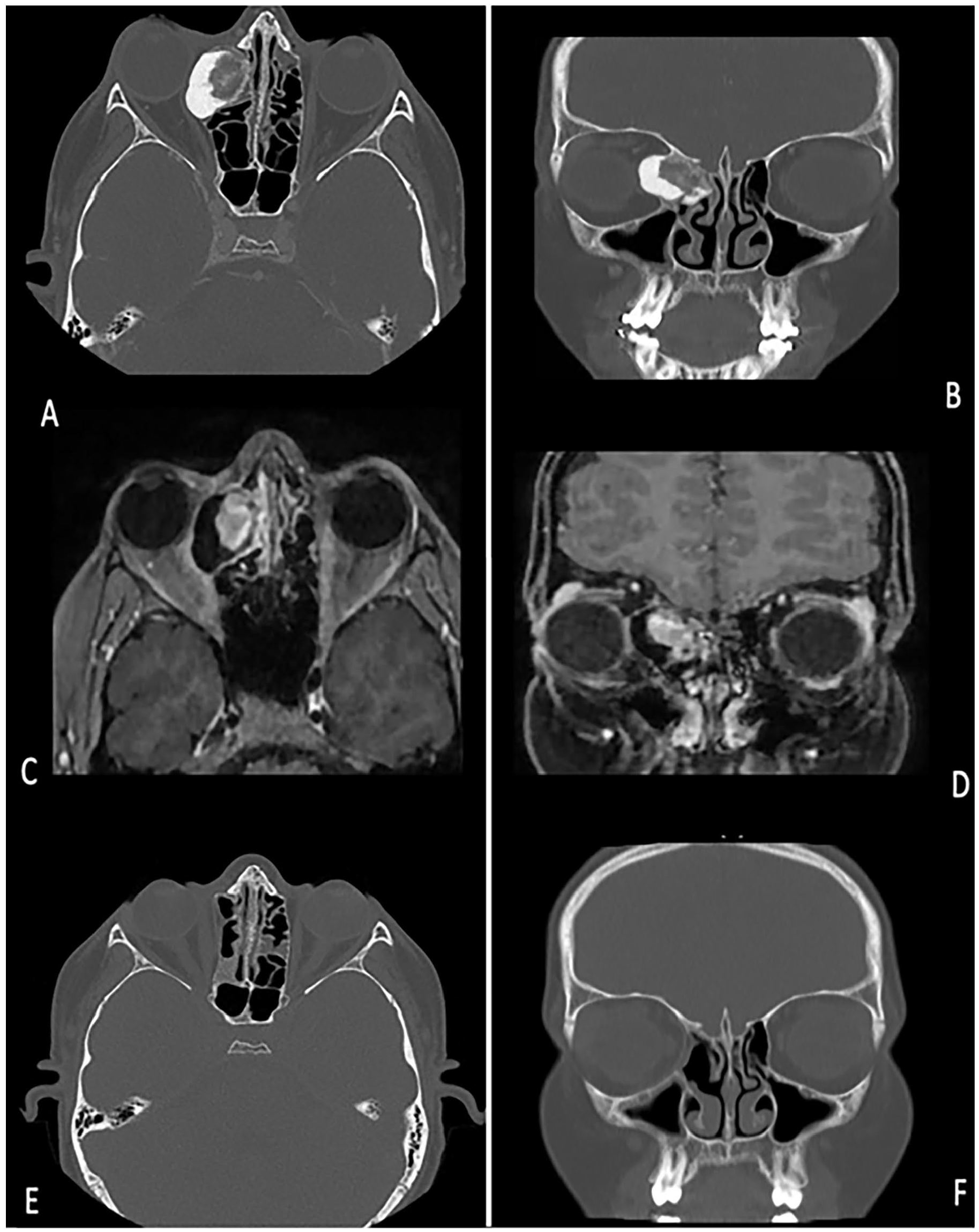
(A) and (B) showing coronal and axial view of CT scan showcasing an expandable lobulated mass in left ethmoidal sinus extending to the orbital cavity. Images (C) and (D) showing coronal and axial view of T1-weighted contrast MRI with mixed flair signal intensity and medial rim enhancement. Images (E) and (F) showing coronal and axial view of CT scan postoperatively which shows no recurrence, no remnant tumor, and adequate tumor resection. CT, computed tomography; MRI, magnetic resonance imaging.
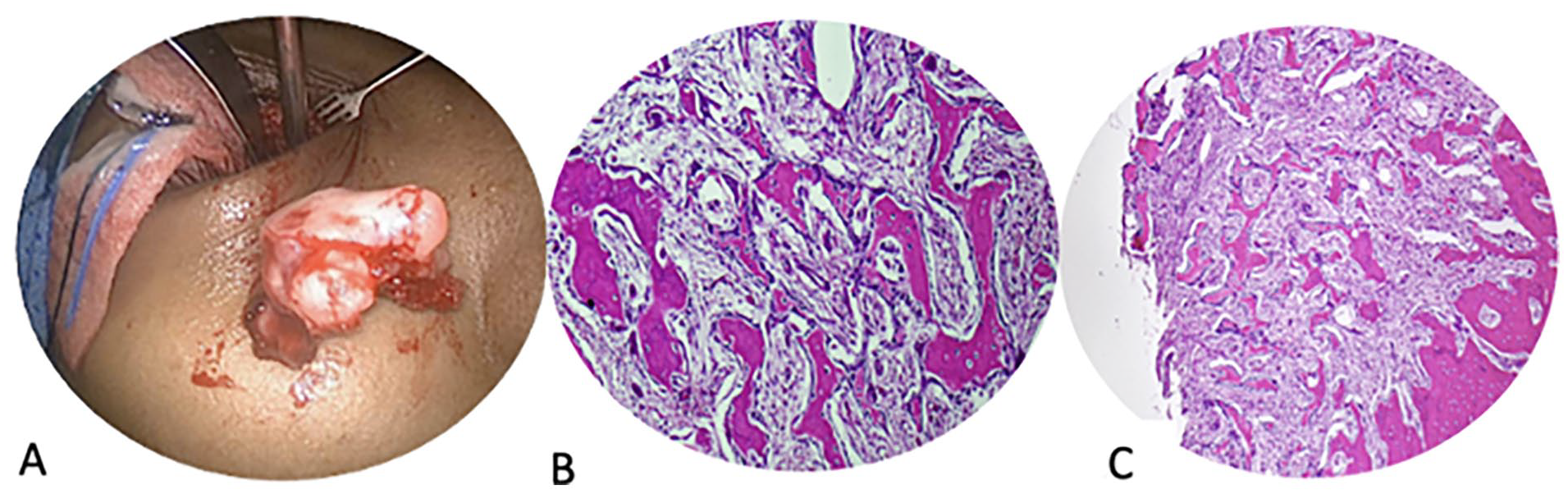
(A) On gross examination, the lesion showed a red granular appearance with a thick shell-like bony component. (B) Microscopic image shows expansile growth surrounded by a sclerotic rim of inter-anastomosing trabeculae of woven bone set within loose edematous fibrovascular stroma. H&E, 40×. (C) Microscopic image shows broad anastomosing trabeculae of woven bone which are lined by a single layer of osteoblasts, a scattered osteoclast type multinucleated giant cells are also present. H&E, 200×. H&E, hematoxylin and eosin
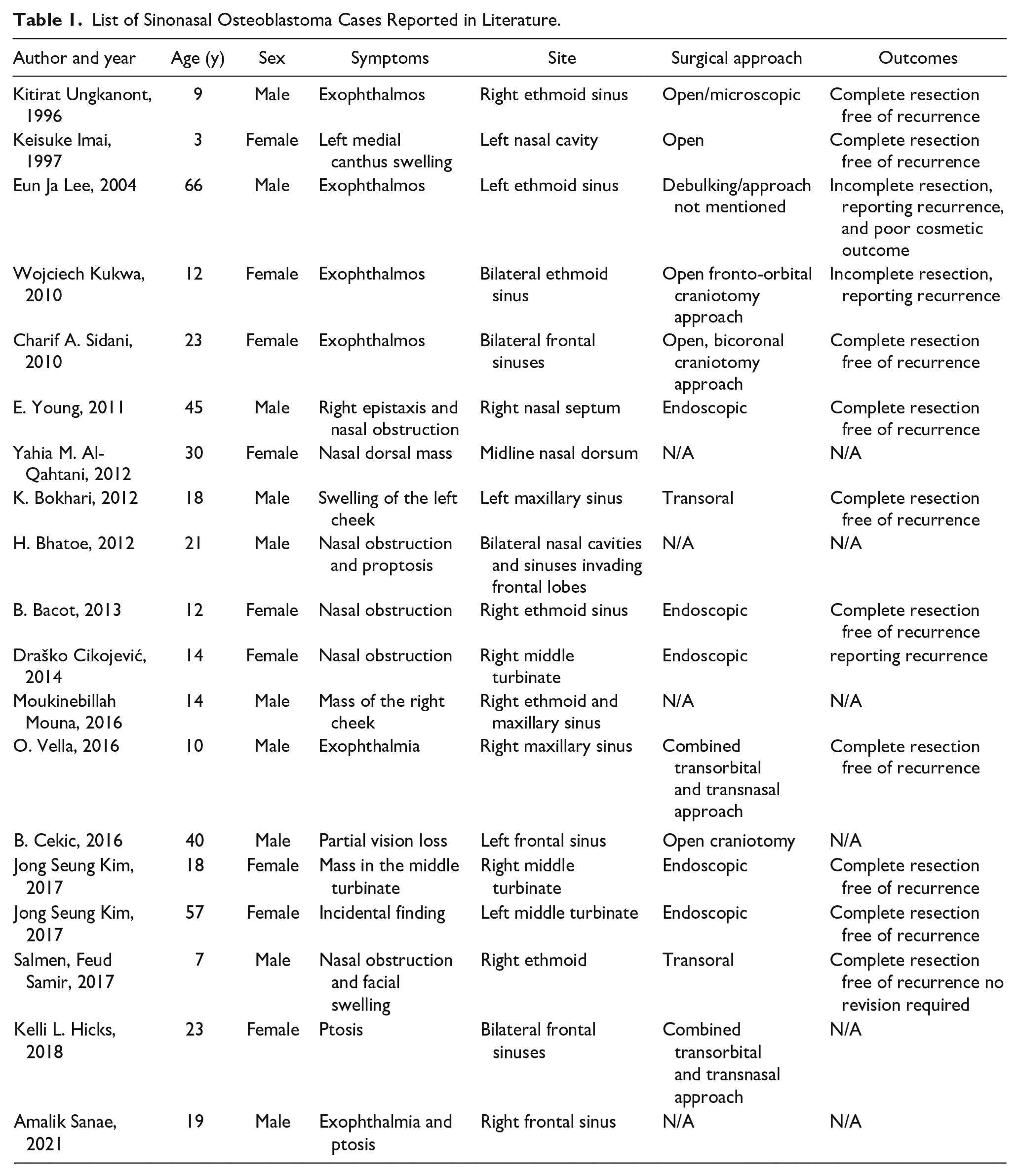
List of Sinonasal Osteoblastoma Cases Reported in Literature.
Discussion
Osteoblastomas in the nasal cavity and paranasal sinuses are rare, with only around 24 reported cases in the literature.9-12 This study aimed to document and summarize cases from 1995 to 2023 to provide valuable information to otolaryngologists regarding the clinical presentation, radiological features, and management options for these tumors.
Presentations varied greatly depending on the organs involved and the lesion’s extension, taking a thorough medical history and physical examination essential. Imaging through CT scans aids in diagnosing the lesion’s exact location, size, and characteristics to guide the physician management. Confirming the diagnosis depends primarily on histological examination after surgical resection, with the most pathognomonic features being the presence of islands of osteoids and considerable osteoblastic activity in a well-vascularized stroma.9-12
The study recommends that physicians consider osteoblastoma as a diagnosis of interest when faced with a heterogeneous osseous/fibrous lesion.13,14 The choice of approach depends on the location and size of the tumor, as well as the surgeon’s expertise. Osteoblastomas tend to recur, so careful surgical management and follow-up are essential.15,16 However, even with a limited conservative approach, complete resolution or regression has occurred in some cases, emphasizing the need for close long-term follow-up.17-20 Endoscopic surgery is generally preferred for tumors located within the boundaries of the sinuses. In some cases, a combined surgical approach may be necessary to ensure complete resection and preserve vital organs, as demonstrated in this report.21-24
In our analysis of the pooled cases, we found the right ethmoid sinus to be the most common site of involvement, overall (3 out of 15 cases, 20%; Figure 3). We also found that these surgical cases had an estimated 2:1 male to female ratio (5 female cases or 33% vs 10 male cases or 67% of total 15 cases). Interestingly, all the cases of right ethmoid sinus were male, and in lower age groups (2 children and 1 adolescent). For recurrence, the data were available for 60% of the cases, whereas it was not available for 40% of cases. Out of 60%, 53% did not have any recurrence, whereas 7% had confirmed recurrence. The recurrence rate is, thus, at least, 7%.
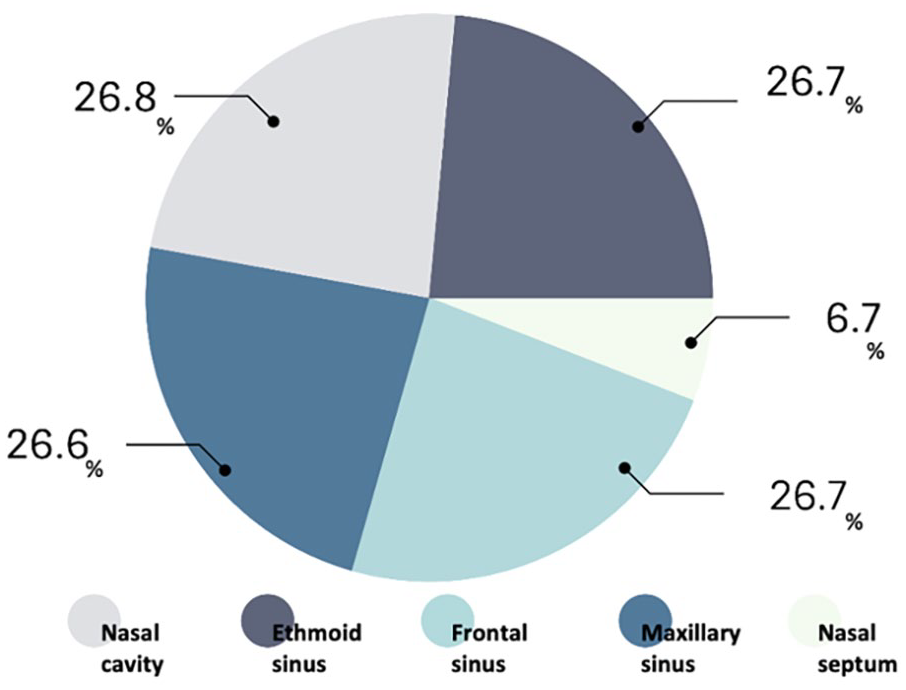
The above chart demonstrating the most common sites of osteoblastoma in the sinonasal region.
Regarding the choice of surgical approach, open and endoscopic surgeries were the 2 preferred choices (each in 3 cases, out of 15). Comparing surgical approaches and outcomes, it becomes evident that the choice of approach can significantly affect results. Open surgeries achieved complete resection without recurrence or revision, showcasing the effectiveness of this approach in one of the reported cases in the literature; debulking procedure with unspecified approaches resulted in incomplete resection and poor cosmetic outcomes. Endoscopic approaches demonstrated favorable outcomes with no recurrence in 5 cases. In contrast, cases with unspecified or nonstandardized approaches lack clear information on outcomes due to variability in surgical methods. The combined transorbital and transnasal approach used in our study resulted in good cosmetic results and no reported recurrences, along with 3 other reported cases in the literature. Therefore, our approach appears to offer favorable outcomes compared to some other approaches, particularly when clear resection margins and cosmetic results are essential considerations. Further research and standardized reporting can provide more comprehensive insights into the best surgical approaches for these case.25-28
Conclusion
We present a case of an osteoblastoma of the right anterior ethmoid sinus cells, with right orbital involvement. In our case, the lesion was removed entirely with the transorbital and transnasal approach. We demonstrate this to be a feasible, effective, and safe technique for complete excision. Further studies are needed to compare outcomes between these various techniques in patients with similar and different extensive ethmoid pathologies with orbital involvement.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
As per manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: King Saud University, Riyadh, Saudi Arabia.