
Abstract
Sinonasal teratocarcinosarcoma (SNTCS) is one of the rarest and most highly invasive malignant neoplasms often found in the nasal cavity and paranasal sinuses. SNTCS is often misdiagnosed because of its morphological heterogeneity. Due to its rarity, clinical characteristics and optimal therapy have not been well-established. Here, we present a case of SNTCS with orbital and intracranial extensions. A 48-year-old male patient presented with left-side nasal obstruction for 3 years. He appeared with visual and neurological symptoms 2 months ago. On radiographic examination, a mass was observed in the left paranasal sinuses with orbital and intracranial extension involvement. The mass was surgically resected. In the future, knowledge of this entity may assist in the accurate diagnosis and proper management of SNTCS.
Introduction
Malignant sinonasal tumors comprise not more than 5% of all head and neck malignancies, with an annual incidence of 0.83 cases per 100,000 people. 1 Sinonasal teratocarcinosarcoma (SNTCS), in particular, is an extremely uncommon, highly invasive malignant tumor that frequently occurs in the nasal cavity and paranasal sinuses, can metastasize, and has a disease-specific mortality rate of 60%–70% at 5 years.2-4 The tumor is no more than 1% of all neoplasm and about 3% of all malignant tumors of the head and neck. 5 SNTCS are often misdiagnosed, and difficult to optimize outcomes due to their infrequency and complex mixture of elements. Treating this carcinoma occurs mainly through surgery and radiation; however, the overall survival of patients remains unsatisfactory owing to the aggressive and rapid progression, recurrence, and intracranial extension of SNTCS. Currently, to the best of our knowledge, only 137 cases have been reported.6-11 Among them, only a few cases are presented with orbital and intracranial extension. In this study, we report a rare case of SNTCS involving the maxillary, anterior ethmoid, and frontal sinuses with orbital and intracranial extensions. We hope that this study helps clinically diagnose and treat this illness in the future.
Case Presentation
Clinical History
A 48-year-old male presented to the ENT (Ear, Nose, and Throat) department in a local hospital with complaints of left nasal obstruction for 3 years. In addition, he reported some specific sinonasal symptoms, such as nasal discharge, hyposmia, and visual impairment. He visited Wuhan Union Hospital for evaluation and treatment.
Imaging
SNTCS usually lacks specific computed tomography (CT) features. In this case, a CT scan revealed that the left frontal, maxillary, anterior ethmoid sinuses, and middle meatus were filled with soft tissue. However, the posterior ethmoid sinus appeared normal. In addition, erosion of the lamina papyracea and skull base was observed (Figure 1A). The diffuse mass infiltrated the left lamina papyracea with erosion of the left orbit. Furthermore, we found that the soft tissue mass destroyed the anterior arterial bone canal with an extension of the anterior ethmoid artery (Figures 1B–D). We also observed that the frontal bone was partially destroyed and the subcutaneous fat layer (Figure 1E). A chest CT revealed no evidence of metastasis. CT scan of the paranasal sinuses. (A–C) Coronal scan, (D) Axial scan, (E) Sagittal scan. (A) A soft tissue mass filling the left frontal, maxillary, anterior ethmoid, and middle meatus extending to the lamina papyracea and skull base (red arrow). (B) A soft tissue mass destroyed the anterior arterial bone canal with the extension of the anterior ethmoid artery. (C) The posterior ethmoid sinus appeared normal. (D) Analysis of the axial section revealed a diffuse mass infiltrated to the left lamina papyracea with erosion into the left orbit. (E) Sagittal section revealed that the frontal bone was partially destroyed and the subcutaneous fat layer. 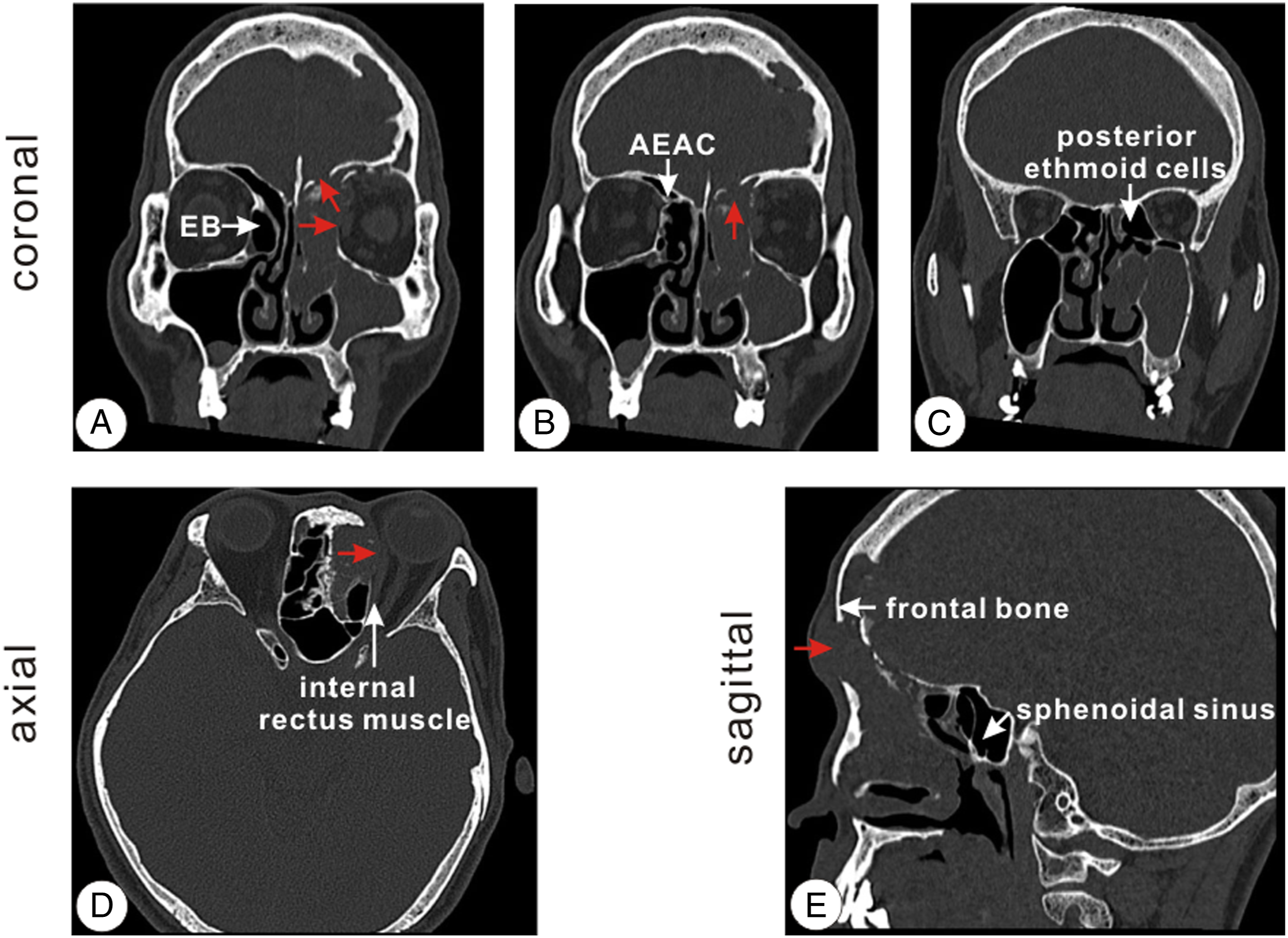
Treatment Strategy
Although there is no defined treatment protocol, radical endoscopic sinus surgery was suggested to the patient after a systematic assessment. Under general anesthesia, the soft tumor in the left middle meatus was completely resected. Because of the extensive tumor invasion (including the left maxillary, anterior ethmoid, and frontal sinus), the lesion lies posterior to and involves the area around the anterior ethmoidal artery; therefore, a modified endoscopic Lothrop procedure (MELP) was performed to remove the tumor completely.
Pathological Examination
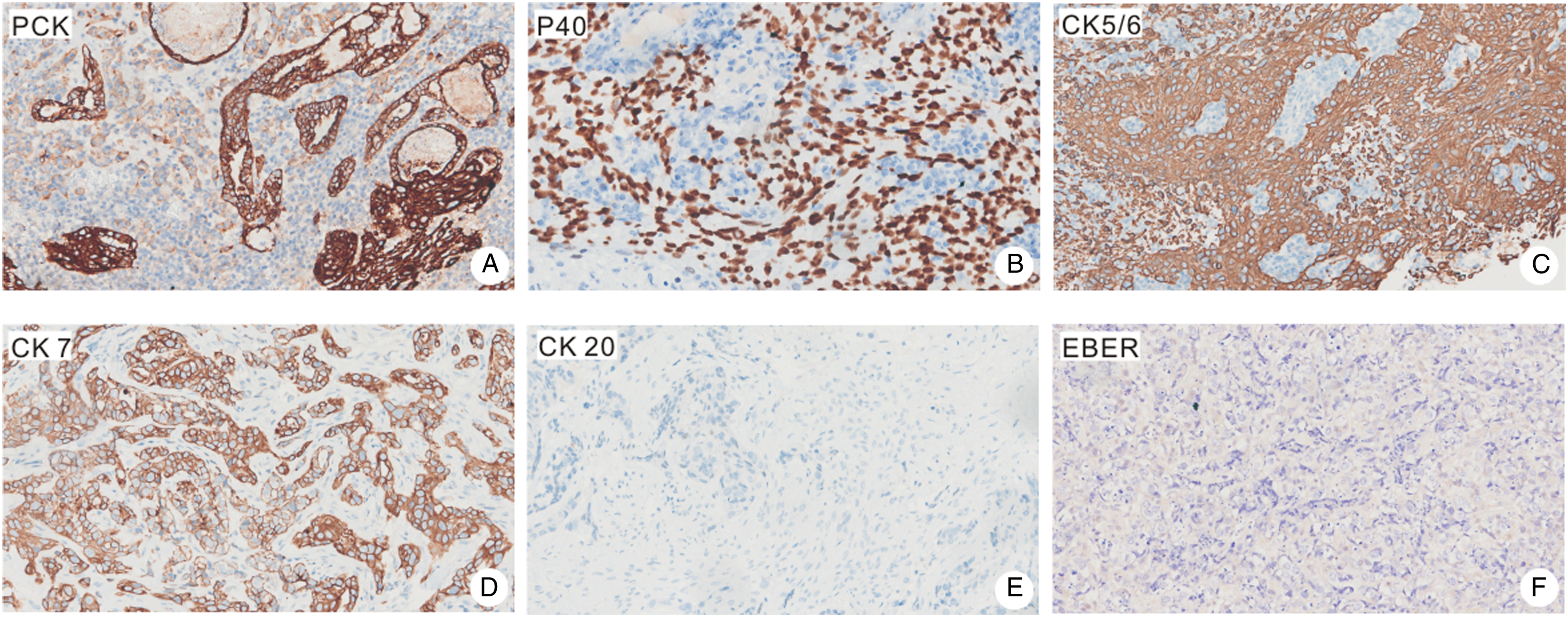
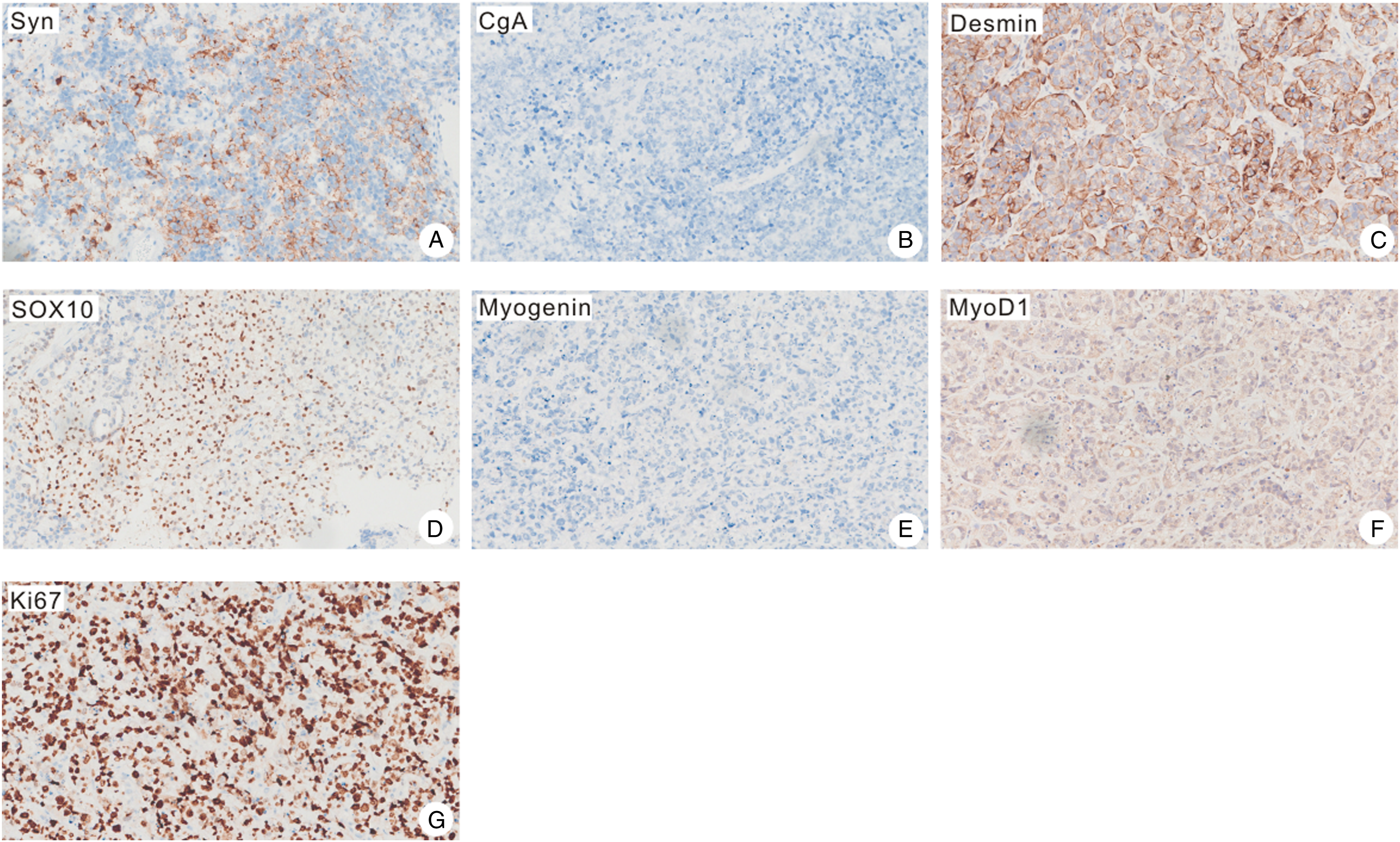
The pathological findings showed non-keratinized and columnar squamous epithelia on the surface of the tumor. The immature squamous cell nests containing clear cells in the core were also observed (Figures 2A and B). In addition, poorly differentiated adenocarcinomic structures were obvious (Figure 2C). The sarcomatous component predominantly had chondroid differentiation, with foci of endochondral calcification (Figures 2C and D). In solid sheets, areas of moderately differentiated adenocarcinoma were noted along with undifferentiated primitive neuroectodermal elements (Figure 2E). The immunohistochemical staining revealed that the tumor and neural epithelia were positive for PCK, P40, CK5/6, and CK7 but negative for CK20 and EBER (Figure 3). In the mesenchymal components, the staining results were positive for Syn, Desmin, SOX10, Ki67, and MyoD1 but negative for CgA or Myogenin (Figure 4). Finally, according to the pathological and immunohistochemistry results, the patient was diagnosed with SNTC; he was recommended to receive radiotherapy after surgery. Pathological analysis of a sinonasal teratocarcinosarcoma. (A) Low magnification of hematoxylin-eosin stain (H&E stain) showing the overall variegated appearance (40X). (B) Areas of well and poorly differentiated squamous cell carcinoma (200X). (C) Poorly differentiated adenocarcinoma structures accompanied by cancerous glands (200X). (D) Low magnification of H&E staining (200X). (E) Rhabdomyosarcomatous differentiation (200X). (F) Primitive neuroectodermal component (200X). The tumor and neural epithelia were positive for PCK (A), P40 (B), CK5/6 (C), and CK7 (D) but negative for CK20 (E) and EBER (F). The mesenchymal components were positive for Syn (A), Desmin (C), SOX10 (D), Ki67 (G), and MyoD1(F) but negative for CgA (B) or Myogenin (E).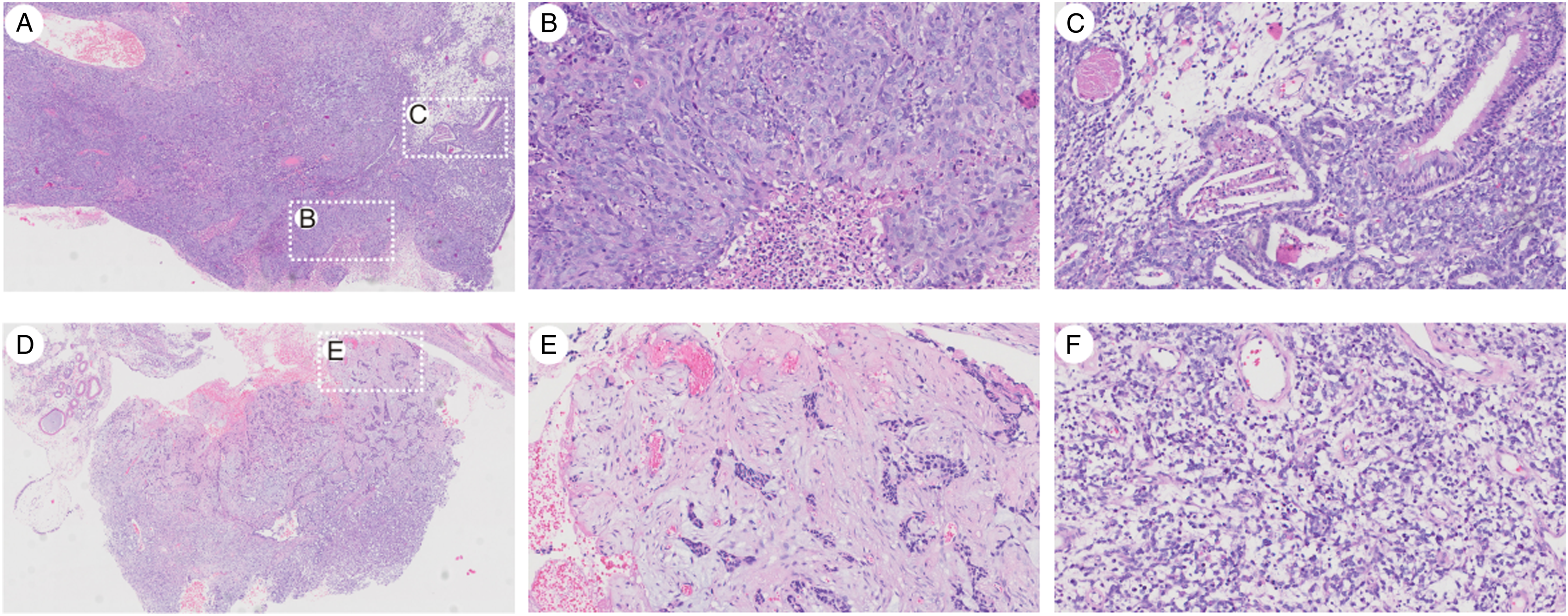
Discussion
Sinonasal teratocarcinosarcoma is an exceptionally unusual and aggressive neoplasm with a poor prognosis. This tumor usually occurs in adults over the age of 35 and has an 8:1 predilection toward men. 9 The most common clinical presentation of this lesion includes nasal obstruction and epistaxis.5,12 However, when the mass occupies the frontal lobes, it could appear with a predominantly cranial presentation, such as confusion and abnormal behavior. 13 Diagnosis may be assisted by pathology and immunohistochemistry. A typical tumor exhibits benign and malignant epithelia, mesenchymal tissue, and neural components. 14 The presentation and management of the disease are variant due to its rarity and heterogenous nature. To date, only fewer than 150 cases of this rare tumor have been reported in the English literature, and only about 10 cases have occurred in China. 6
Nearly all SNTCS arise within the nasal cavity and paranasal sinuses.9,10 A few literatures have also reported orbital and/or cranial invasion at presentation, or progression.12,13,15 In some cases, the site of origin could not be determined due to the rapid growth of the tumor and its involvement with adjacent structures. 5 Our patient presented with orbit and intracranial involvement and relative manifestations, such as diminished vision and headache.
Sinonasal teratocarcinosarcoma are a rapidly growing, aggressive neoplasm with a poor prognosis. Most patients progress to extensive disease within 3 years. 13 Currently, surgery adjuvant radiochemotherapy has been considered the optimal treatment strategy.6,16,17 Surgery alone is challenging to guarantee complete tumor resection because of the metastasis of the tumor and the anatomical complexity of the nasal sinuses. In this case, CT imaging typically demonstrates an infiltrating mass with medium or high signal intensity. The recommended treatment is resection, but extensive local destruction often precludes complete removal. Adjuvant radiation therapy may be helpful, but aggressive chemotherapy is less well-established.6,13 Our patient received radiation therapy after surgery; later, he underwent follow-up.
This case illustrates that SNTCS is an extremely uncommon and unique sinonasal neoplasm. Sinonasal teratocarcinosarcoma often poses a diagnostic challenge, particularly in small biopsy samples or partially removed tumor specimens. To avoid an erroneous diagnosis, aggressive sampling with histopathological examination is required. Given the extremely poor prognosis, multimodality treatment in the form of postoperative radiotherapy and chemotherapy must be standardized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the National Natural Science Foundation of China (81771005, ZT), the Research Grant of Union Hospital, Tongji Medical College, HUST (F016.02004.21003.126, ZT), and Open Project of Key Laboratory of Molecular Imaging (2021fzyx017, SH).
Ethical/consent statement
Ethics approval and consent to participate: Not applicable.
Grant Number and Data Availability statement
All data generated or analyzed during this study are included in this published article [and its supplementary information files].