
Abstract
Paranasal sinus tumors are a heterogeneous group of neoplasms (with paranasal schwannomas being a rare subtype) that are often present with non-specific symptoms, such as nasal obstruction and epistaxis. Thus, early diagnosis is crucial for optimal management. This study presents 2 cases of paranasal schwannomas, detailing their clinical presentation, diagnostic methods, and treatment approaches. Both patients underwent endoscopic sinus surgery with successful tumor excision and had no significant complications or recurrences during follow-up. Diagnosis was based on a combination of clinical examination, radiological imaging (computed tomography and magnetic resonance imaging), and histopathological confirmation with immunohistochemical staining. Treatment consisted primarily of endonasal resection, with consideration of frontal craniotomy if necessary. This study aims to contribute to the understanding of paranasal schwannomas and emphasizes the importance of early detection and treatment to improve patient outcomes.
Introduction
Paranasal sinus tumors are a diverse group of neoplasms arising from the paranasal sinuses and nasal cavity, accounting for approximately 3% of all head and neck tumors. Early diagnosis and appropriate management are essential as these tumors can lead to significant morbidity and potential mortality if left untreated. Paranasal sinus tumors can be classified into different subtypes—such as epithelial, mesenchymal, and neurogenic—with schwannomas being a rare type of neurogenic tumor. Schwannomas, also known as neurilemmomas, are benign peripheral nerve sheath tumors that arise from Schwann cells. They typically occur in the head and neck region (25%-45% of cases); however, paranasal schwannomas account for only 4% of all sinonasal tumors.1,2 Due to their unusual location and rarity, sinonasal schwannomas are low on the differential diagnosis of masses in the anterior skull base or nasal cavity.
The clinical presentation of paranasal schwannomas varies depending on the location and size of the tumor, but often includes nasal obstruction, epistaxis, and facial pain or tenderness. Diagnosis involves a combination of clinical examination, radiological imaging [eg, computed tomography (CT) and magnetic resonance imaging (MRI)], and histopathological confirmation by biopsy. The treatment of choice for paranasal schwannomas is complete surgical excision, often supplemented by radiotherapy in selected cases. 3 Overall, the prognosis for paranasal schwannomas is favorable, with a low recurrence rate following complete resection.
Through a detailed review of the clinical presentation, diagnostic methods, and treatment approaches, this study aims to contribute to existing literature and improve the understanding of paranasal schwannomas. By reporting these unique cases, we aim to emphasize the importance of early detection and management of paranasal schwannomas.
Case Report
Case 1
A 39-year-old woman initially consulted her general practitioner (GP) because of a 6-month history of nasal obstruction and nasal discharge without episodes of nasal bleeding. After identifying a nasal tumor in the left nasal cavity, her GP recommended further evaluation at a nearby hospital. After a thorough examination at the designated hospital, a biopsy was performed, and the results indicated the presence of a nasal schwannoma. She was then referred to our department for further treatment. On arrival at our hospital, a smooth surface tumor was observed that blocked the left nasal cavity, and the origin could not be identified (Figure 1A). The patient underwent a series of imaging studies, including CT and MRI. CT revealed an expanding mass effect extending from the left medial meatus to the anterior ethmoidal sinus; MRI showed an isointense signal on T1-weighted sequences and an iso- to hyperintense signal on T2-weighted sequences within the same area, accompanied by an inhomogeneous internal composition. (Figure 1B and C)
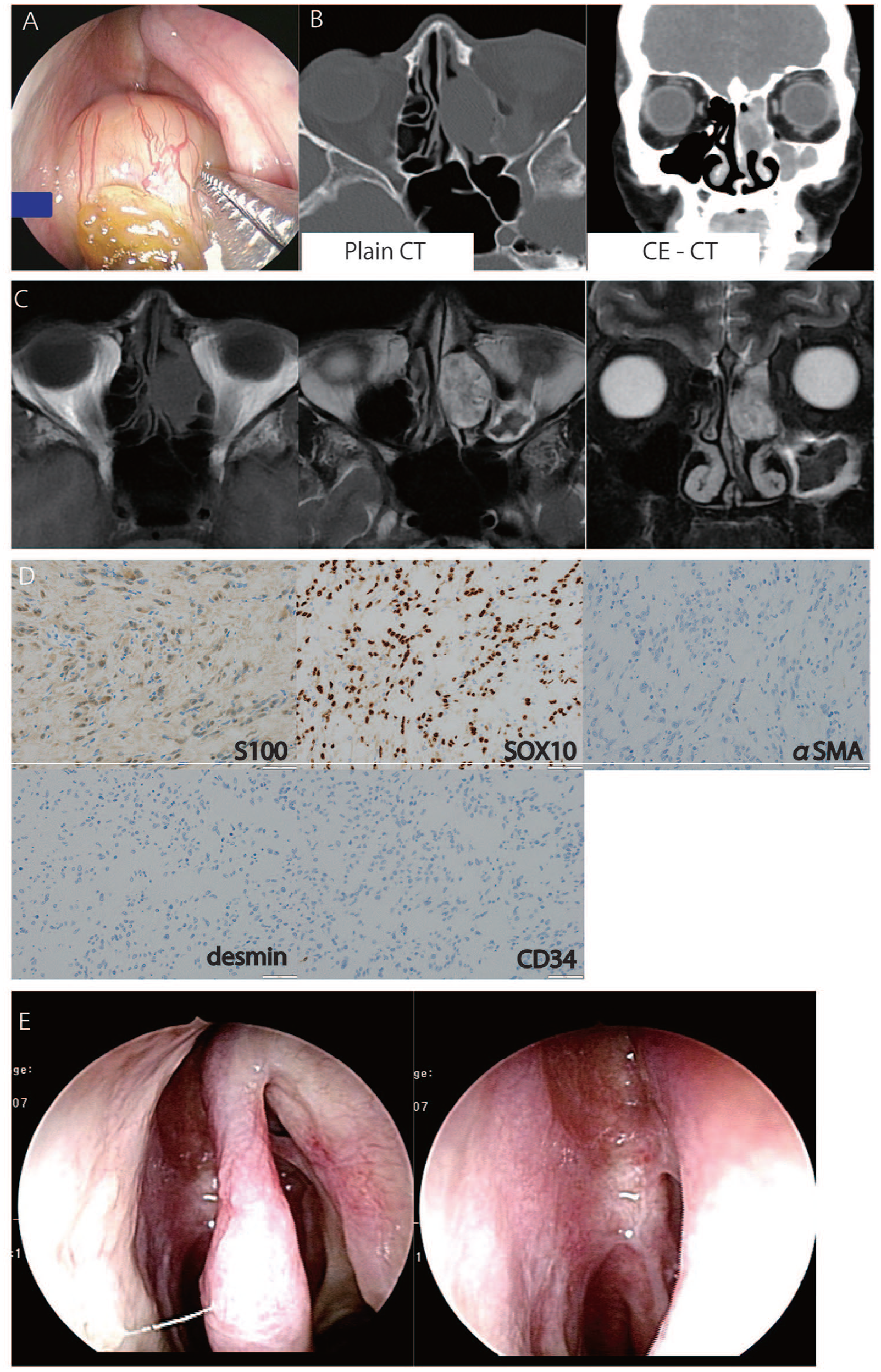
(A) Endonasal fiber findings at initial examination. A smooth surface mass lesion was detected. The tumor filled the left nasal cavity, making identification of the tumor stem difficult. (B) Nasal and paranasal sinus computed tomography findings. A filling shadow is observed in the left nasal cavity. The frontal sinus, anterior ethmoidal sinus, and maxillary sinus also showing shadows with no obvious bone destruction. (C) Nasal and paranasal MRI findings. Nasal tumor showing an isointense signal on T1-weighted sequences and an iso- to hyperintense signal on T2-weighted sequences. The frontal sinus displaying iso-intensity on both T1- and T2-weighted imaging, while the maxillary sinus exhibiting hyperintensity on T1-weighted imaging and hypointensity on T2-weighted imaging, indicative of a probable diagnosis of chronic rhinosinusitis. (D) Extraction of pathology observations with immunohisotochemical staining S100 (+), SOX10 (+), αSMA(−), desmin (−), and CD34 (−) tumor cells infiltration is evident. (E) Intranasal findings at 18 months postoperatively. No tumor recurrence is observed.
The patient then underwent endoscopic sinus surgery under general anesthesia to excise the tumor. Intra-operative findings revealed that the tumor originated from the olfactory fissure. The tumor was very delicate and difficult to resect in one piece, thus it was divided into sections and removed. The procedure was completed without any complications. Pathological examination revealed that the tumor was S100 positive, SOX10 positive, αSMA negative, desmin negative, and CD34 negative with no obvious malignant features (Figure 1D). The final diagnosis was therefore confirmed schwannoma. At her 18-months postoperative follow-up, the patient reported no recurrence of symptoms; and no evidence of tumor recurrence was observed (Figure 1E).
Case 2
A 56-year-old woman presented with persistent nasal obstruction and discharge that had been present for a year without pain or nasal bleeding and without significant change in symptoms. At her first hospital visit, a tumor was discovered in her left nasal cavity. A biopsy confirmed the diagnosis of schwannoma, and she was subsequently referred to our hospital for treatment. The patient had no family history of similar conditions.
Arriving at our hospital, the patient underwent a CT scan, that revealed a mass without bone destruction in the left nasal cavity with heterogeneous contrast enhancement (Figure 2A). No sinusitis was observed. In addition, multiple highly calcified intracranial neoplastic lesions were identified. MRI of the nasal tumor displayed low intensity on T1-weighted images and high intensity on T2-weighted images with some heterogeneous isointensity areas internally (Figure 2B). The patient was referred to the neurosurgery department, where multiple meningiomas were diagnosed. She then underwent endoscopic sinus surgery under general anesthesia for symptomatic relief. The tumor had a smooth surface and its base was located posterior to the nasal septum. An incision was made in the mucosa surrounding the base, and the tumor was carefully dissected subperiosteally before being removed in 1 piece (Figure 2C). No significant intraoperative or postoperative complications were encountered. Pathological examination revealed that the tumor was S100 positive. The final diagnosis was therefore confirmed as schwannoma. At her 3-month postoperative follow-up, the wound had apparently healed (Figure 2D).
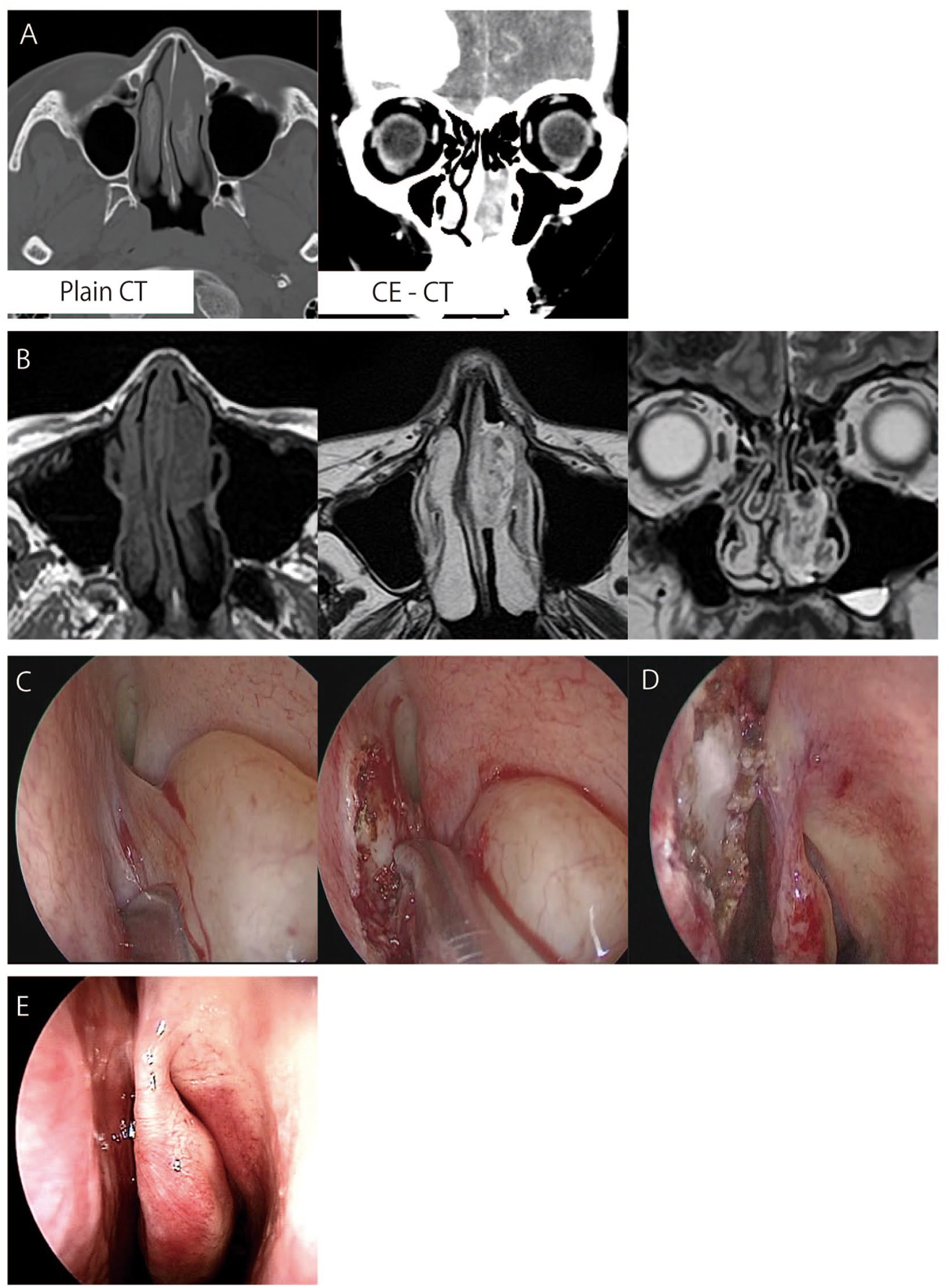
(A) Nasal and paranasal CT findings. A shadow without bone destruction is visible anteriorly on the left middle turbinate. The mass was accompanied by a contrast effect. No obvious shadow is observed in the paranasal sinuses. (B) Nasal and paranasal MRI findings. Nasal tumor showing low intensity on T1-weighted images and high intensity on T2-weighted images with some heterogeneous isointensity areas internally. (C) Intraoperative findings. The tumor originating from the nasal septum. (D) Findings at the end of surgery. The nasal septal mucosa resected with a 2-mm margin around the tumor stem. The nasal septal cartilage is preserved. (E) Nasal findings 6 months postoperatively. The wound is epithelialized well with no obvious abnormality.
Discussion
Sinonasal schwannomas are rare and benign tumors that originate from Schwann cells in the nasal cavity or the anterior skull base.4 -6 Histologically, they can present as Antoni Type A and Antoni Type B architectures. Schwannoma cells can be characterized by a positive S-100 immunohistochemical stain, further narrowing the differentiation of nasal tumors. 7 On CT, schwannomas appear isodense compared to the rest of the brain with moderate enhancement using contrast-enhanced CT; and on MRI, they show iso- to hypointense masses on T1-weighted images with prominent heterogeneous enhancement and T2 hyperintensity. Hemosiderin deposition can be visualized in some schwannomas on T2-weighed images, offering a critical diagnostic clue.
Many lesions have overlapping nonspecific symptoms, including esthesioneuroblastoma, adenocarcinoma, sinonasal undifferentiated carcinoma, squamous cell carcinoma, inverted papilloma, sinonasal neurofibromas, and olfactory ensheathing cell tumors. While radiographic features may help with clinical differentiation, diagnosis hinges on a tissue biopsy. Specialized immunostaining can aid in a more accurate diagnosis. In the present case, the endoscopic findings revealed a smooth surface; and no evidence of bleeding or papillary growth, leading to the diagnosis of a possible benign tumor that was confirmed by biopsy.
Treatment for schwannomas consists of endonasal resection, with frontal craniotomy when needed. In some cases, postoperative radiation therapy may be considered if the disease has become malignant. 8 Potential treatment complications include cerebrospinal fluid leak (CSF) leaks or neurologic deficits in the literature review. 9 No postoperative complications were observed in either of the 2 cases, and no mixed malignant findings were found in the pathology results.Therefore, no additional treatment was provided, and the patient is currently under observation.
To summarize, sinonasal schwannomas are rare tumors that can present with nonspecific symptoms and radiographic features overlapping with other lesions. Diagnosis relies on a combination of imaging findings, histopathology, and immunohistochemical staining. Treatment typically involves endonasal resection and, if necessary, frontal craniotomy. Identifying the basis of tumor origin and management of schwannomas can lead to successful outcomes for patients.
Footnotes
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author, T.T. The data are not publicly available due to restrictions, for example, their containing information that could compromise the privacy of research participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethics committee of Osaka University (No. 16329).
Statement of Human and Animal Rights
No humans or animals were harmed during this study.
Statement of Informed Consent
Informed consent was obtained from the patient for their anonymized information to be published in this article.