
Abstract
Adenoid cystic carcinoma (ACC) is a rare tumor, with a documented annual incidence ranging from 3 to 4.5 cases per million. It constitutes approximately 1% of all head and neck malignancies and around 10% of salivary gland tumors. It is imperative to adopt a multidisciplinary approach to ensure the most appropriate therapeutic outcome. Treatment strategies usually involve a multidisciplinary approach and may include surgery, radiotherapy, chemotherapy, or various combinations of these. In this context, we present a clinical case of ACC originating in the palate of a woman. Throughout this article, we will detail the diagnostic challenges and multidisciplinary treatment strategies implemented, emphasizing the importance of a comprehensive approach in cases of palatal ACC. In addition, we will discuss the rehabilitation process and the outcomes observed during the follow-up of this case.
Introduction
Adenoid cystic carcinoma (ACC) is a rare tumor, with a documented annual incidence ranging from 3 to 4.5 cases per million. 1 It constitutes approximately 1% of all head and neck malignancies and around 10% of salivary gland tumors.1,2 In addition, it ranks among the most prevalent cancers affecting the major salivary glands, including the parotid, submandibular, and sublingual salivary glands. 3 ACC can also affect lacrimal and ceruminous glands, as well as other regions in the head and neck, including the nasal and paranasal sinuses, larynx, and trachea. 4 ACC is marked by gradual local growth, a high incidence of perineural invasion, rare regional metastases, and the frequent occurrence of local recurrences. It typically exhibits a slow and relatively indolent progression with distant metastases. 5
There are 3 histological subtypes of ACC: cribriform, tubular, and solid. These subtypes can occur independently or coexist within the same tumor. The solid subtype is recognized as the most aggressive among them. 6 The tumor is graded based on the criteria established by Szanto et al in cribriform or tubular (grade I), less than 30% solid (grade II), or greater than 30% solid (grade III). 7 Immunohistochemical stains, such as S100 and smooth muscle actin, assist in identifying these cell types and distinguishing ACC from other salivary gland tumors. 8
ACC commonly originates from the palate, with the tongue and oral mucosa being the subsequent frequent sites. In the case of palatal ACC, surgical removal is the primary treatment. Nonetheless, the challenging location of the tumor complicates achieving complete resection. Local recurrence may occur along the surgical margin, or dissemination may happen from the large nerve trunk. 9
Treatment strategies usually involve a multidisciplinary approach and may include surgery, radiotherapy, chemotherapy, or various combinations of these. Combined therapies, like surgery with radiotherapy or radiotherapy with chemotherapy, are frequently preferred. 10
Some studies showed superior 5 year and 10 year survival rates for the combination of surgery and postoperative radiotherapy, with survival rates compared for surgery alone. 11 In this context, we present a clinical case of ACC originating in the palate of a woman. Throughout this article, we will detail the diagnostic challenges and multidisciplinary treatment strategies implemented, emphasizing the importance of a comprehensive approach in cases of palatal ACC. In addition, we will discuss the rehabilitation process and the outcomes observed during the follow-up of this case.
Clinical Case
A 37-year-old patient, for the past 5 months, has been experiencing constipation and nasal congestion, nocturnal dyspnea, and subsequent development of an infiltrative ulcerated lesion in the palate with associated intermittent pain. There was no significant medical history. The physical examination revealed a painful ulcer compromising both the soft and hard palate on the left side. A biopsy of the lesion was performed, confirming ACC. Imaging studies, including a computed tomography scan and 18 Fluorodeoxiglucose (FDG) positron emission tomography (PET) scan, revealed a tumor, which originated in the soft palate, extended to the hard palate and the posterior wall of the left maxillary sinus. It also involved the palatine foramina and destroyed the medial pterygoid process on this side. It extended toward the left choana and, to a lesser extent, to the choana on the right side, contacting the posterior aspect of the nasal septum (Figure 1).
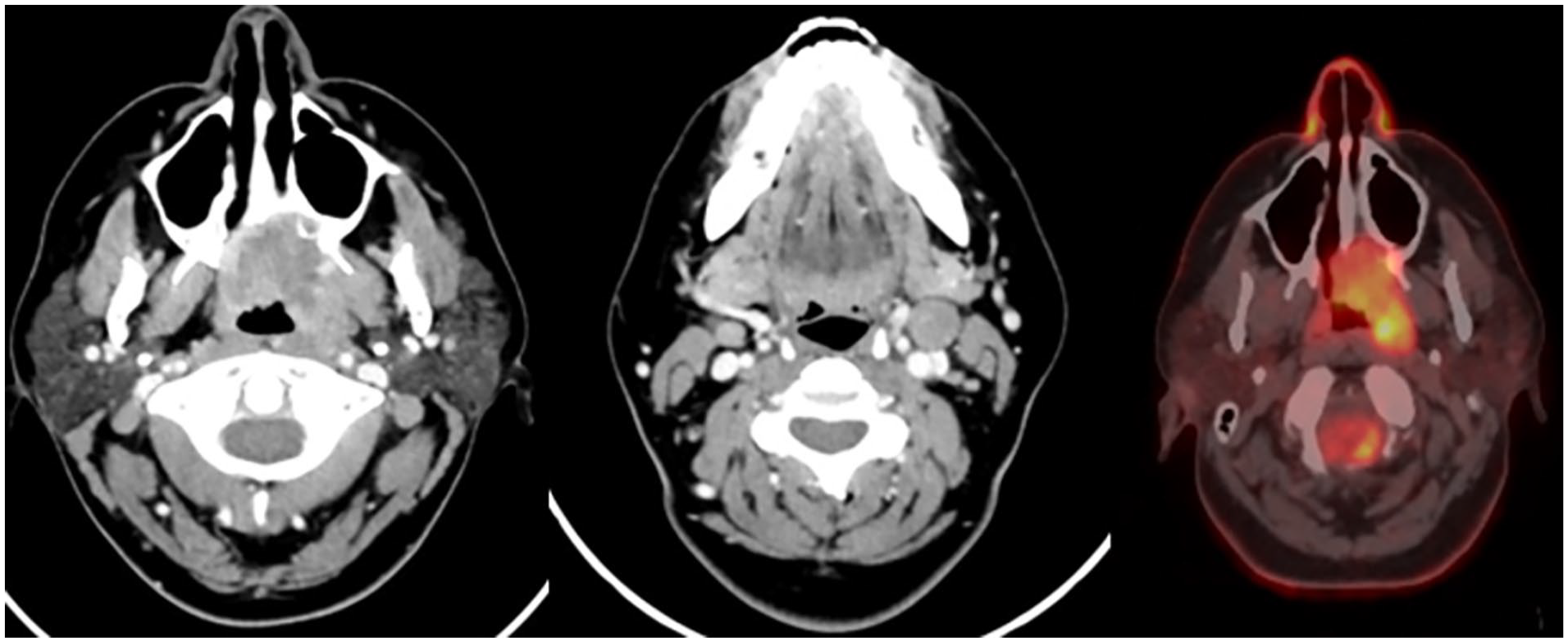
A 4 cm neoplastic-looking lesion in the left pharyngeal mucosal space involving the soft palate, eroding the hard palate, and the posterior wall of the left maxilla. It caudally extends toward the left choanae and posteriorly into the nasopharynx. Cervical adenopathy in level IIA suspicious of secondary neoplastic involvement. Both lesions show significant uptake on the PET scan. PET, positron emission tomography.
The patient was presented at a multidisciplinary board, considering that the best treatment was an initial surgical approach. The procedure included maxillectomy, bilateral modified radical neck dissection, endoscopic nasopharyngeal resection, and reconstruction using a radial free flap (Figure 2).
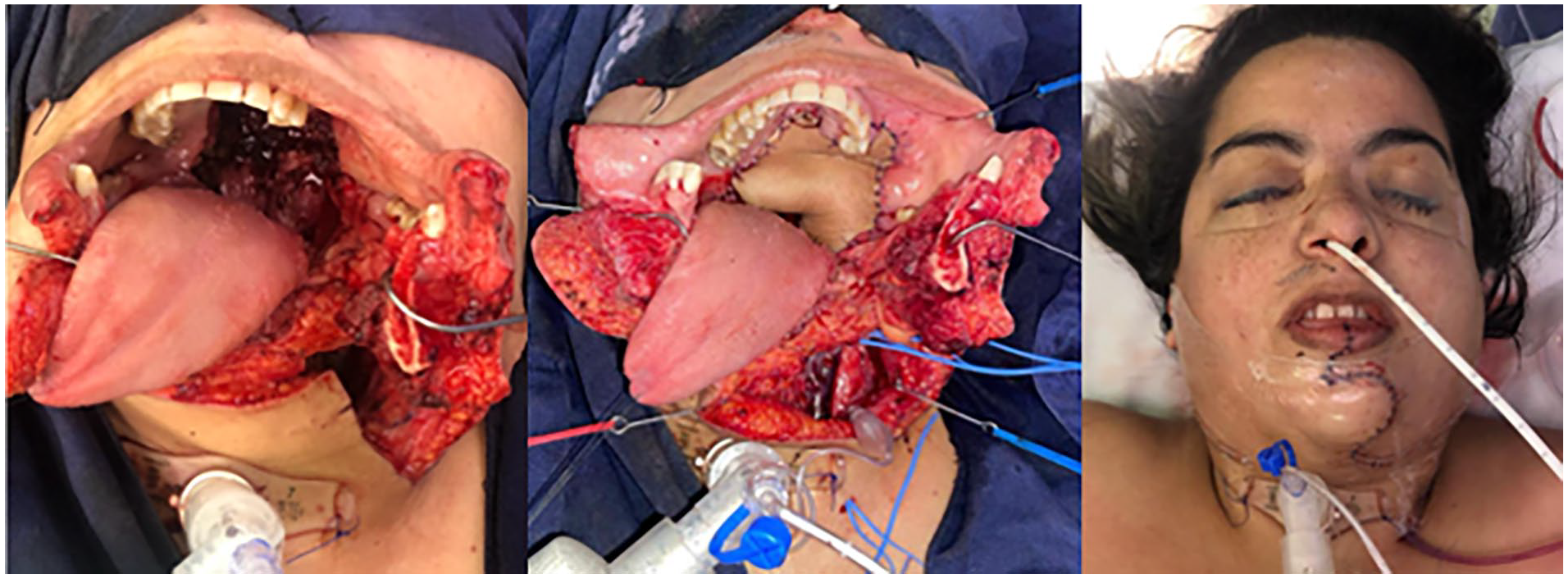
Exposure with mandibulotomy of infiltrative lesion in the palate. Coverage with radial free flap of the resected area.
The patient was transferred to the intensive care unit for 4 days, followed by management in the hospital for an additional 4 days. Discharge was carried out without complications. The patient was further managed for an additional week with enteral nutrition via a tube and a tracheostomy, both of which were subsequently removed.
Pathology confirmed a 4 cm tubular, cribriform, and solid pattern, low-grade ACC in the palate, with perineural and lymphovascular invasion. One out of 13 lymph nodes and surrounding soft tissues were involved. Adjuvant treatment was defined, consisting of 6000 cGy/200 cGy radiotherapy and platinum-based chemotherapy.
The patient has been monitored with favorable progress; a follow-up PET scan at 3 months showed no focal uptake. Follow-up at 18 months revealed no evidence of tumor recurrence, demonstrating satisfactory functional, aesthetic, and oncologic outcomes (Figure 3).

An 18 month follow-up with no evidence of tumor recurrence, satisfactory functional, aesthetic, and oncologic evolution.
Discussion
ACC is a malignant tumor composed of ductal cells and abluminal modified myoepithelial basaloid cells showing various microscopic patterns, The growth patterns are classified into cribriform, tubular, and solid structures. 12 The clinical stages were classified according to the American Joint Committee on Cancer’s Cancer Staging Manual. 13 Patients with ACC exhibit a 5 year survival rate ranging from 67% to 73%. Nevertheless, owing to the traits of delayed locoregional recurrence and distant metastasis, the 10 year and 20 year survival rates are considerably poorer. 14
Regarding the treatment, we find that radical excision with wide safety margins in combination with postoperative radiotherapy (or, depending on the case, concurrent chemotherapy) is the preferred treatment of ACC in the head and neck region; ACC originating from the minor salivary glands of the palate is a malignant tumor with life-threatening potential, primarily because of its elevated likelihood of recurrence and metastasis to multiple organs. The distinctive biological traits of ACC encompass local recurrence, perineural expansion, and delayed distant metastasis. 15
In complex cases like this, we consider it is imperative to adopt a multidisciplinary approach to ensure the most appropriate therapeutic outcome. In our hospital, we have a high-volume pathology center, supported by a specialized team in the interpretation of head and neck pathology. This group of experts collaborates closely with professionals in specialized radiology, head and neck oncologic surgery, reconstructive surgery, as well as clinical oncology and specialized radiotherapy, playing a crucial role in the initial therapeutic decision-making and the selection of the most suitable adjuvant treatment.
Furthermore, we recognize the importance of comprehensive support during treatment. Our multidisciplinary team includes professionals in nutrition, palliative support for pain management, and dentistry. These specialists provide significant support to enhance the patient’s quality of life throughout their treatment.
In conclusion, the comprehensive management of ACC requires a diligent and collaborative approach. The combination of advanced surgical techniques, postoperative radiotherapy, and, in some cases, concurrent chemotherapy proves to be essential in addressing the complexities of this tumor.
Footnotes
Data Availability
The case information was obtained in an authorized manner by the patient and the treating surgical group. The author agrees to share our research data in a suitable public repository subject to ethical considerations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This case report was carried out within the ethical principles for medical research in humans according to the Declaration of Helsinki—59th General Assembly, Seoul, Korea, October 2008. The national regulations of the Ministry of Health and Social Protection of Colombia Resolution 8430 of 1993 regarding Chapter I “Of the ethical aspects of research in human beings” were taken into account. This research is classified within the research category without risk, and with the informed consent of the patient. Authorization for this report was given by the patient and ethical approval is not applicable for this article.