
Abstract
Ameloblastic carcinoma (AC) represents a distinct challenge in the realm of odontogenic malignancies due to its rarity and aggressive nature. We present a unique case of AC in a 70-year-old male, retired dry cleaner, with symptoms initially suggestive of chronic allergic rhinitis and recurrent acute sinusitis with asymmetric facial edema and paresthesia. Detailed evaluation revealed a prominent mass in the right maxillary sinus with extensive cortical destruction. Pathological assessment post-right maxillectomy identified a high-grade AC with malignant spindle cell transformation. The patient underwent subsequent interventions, including neck dissection and radiation therapy. Twelve months post-presentation, the patient was recovering appropriately without evidence of recurrence of malignancy. This case highlights the diagnostic challenges posed by AC as well as its unique presentations emphasizing the importance of a comprehensive approach and multidisciplinary management. It also raises considerations about potential chemical exposure implications in AC development.
Introduction
Ameloblastic carcinoma (AC) is a rare malignancy of odontogenic epithelial origin with potential for significant growth. It is characterized by its potential for invasion and distant metastasis, contributing to significant morbidity and mortality.1,2 AC accounts for approximately 2% of all odontogenic tumors according to one retrospective study. 3 Thus, the rarity of this malignancy has resulted in a limited understanding of its clinical presentation, pathogenesis, and optimal treatment approaches. These gaps in understanding underscore the need for further investigation into AC. Through detailed and unique case reports and studies, we can enhance the understanding of this uncommon malignancy, improving diagnostic accuracy, treatment protocols, and patient outcomes. This report aims to contribute to a growing body of knowledge by presenting a unique case of AC as well as its identification, treatment, and outcomes.
Case Report
A 70-year-old man who is a retired dry cleaner presented to our clinic with complaints persisting over 3 months. His symptoms were characterized by numbness in the right upper teeth, persistent right facial pressure and swelling, odynophagia, right epiphora, and bilateral nasal congestion worse in the mornings with a milky discharge. He recounted a long-standing history of allergic rhinitis, which was addressed with subcutaneous immunotherapy 3 decades prior. In addition, he experienced episodes of sinusitis 2 to 3 times annually over the past 10 years managed conservatively with antibiotics, steroids, fluticasone, and nasal rinsing.
The patient denied any changes in olfactory or visual acuity, epistaxis, or unexplained weight reductions. He also confirmed a nonsmoking status and denied any use of nasal illicit substances. His medical background was unremarkable for any sinonasal surgical interventions.
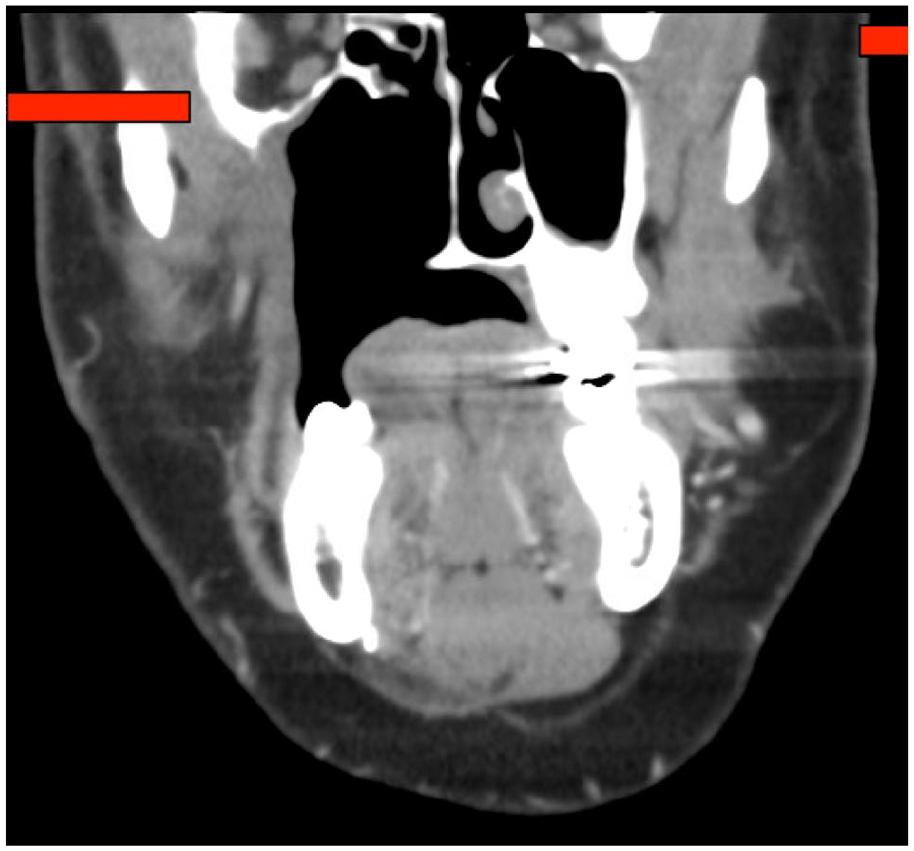
Rigid nasal endoscopy revealed right middle meatus fullness with inflamed mucosa diffusely. No frank masses were noted. A contrast-enhanced computed tomography (CT) scan of the sinuses elucidated a prominent mass within the right maxillary sinus with extensive cortical destruction, with notable extensions into multiple regions including the right orbital floor, pterygopalatine fissure, middle meatus, anterior maxillary sinus wall, and down to the roots of the first and second molar teeth. The left maxillary sinus displayed an oroantral fistula without other significant anomalies (Figure 1).
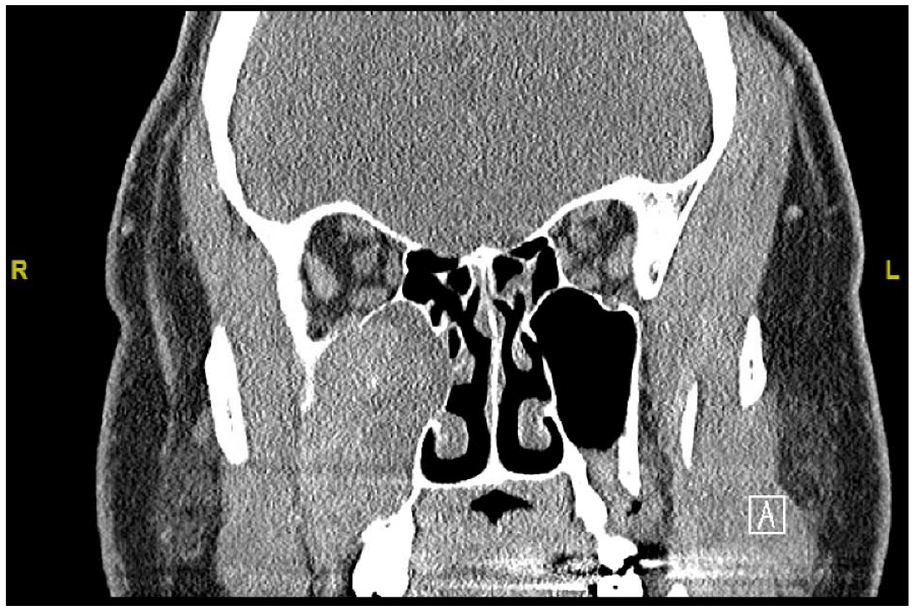
Preoperative computed tomography scan of the sinuses with contrast demonstrating a large mass in the right maxillary sinus, cortical destruction of the right orbital floor, and a left oroantral fistula.
Further evaluation using a nuclear medicine positron emission tomography (PET) scan with CT showed hypermetabolic activity in the right level 2 lymph nodes (Figure 2). Two months post-presentation, a nasal biopsy demonstrated invasive squamous cell carcinoma with basaloid characteristics. Immunohistochemistry was positive for CK5/6, P63, P40, and P16 while being negative for CK7, S100, CD117, and smooth muscle actin. This resulted in the lesion being characterized as a T4acN0M0 squamous cell carcinoma with basaloid features.
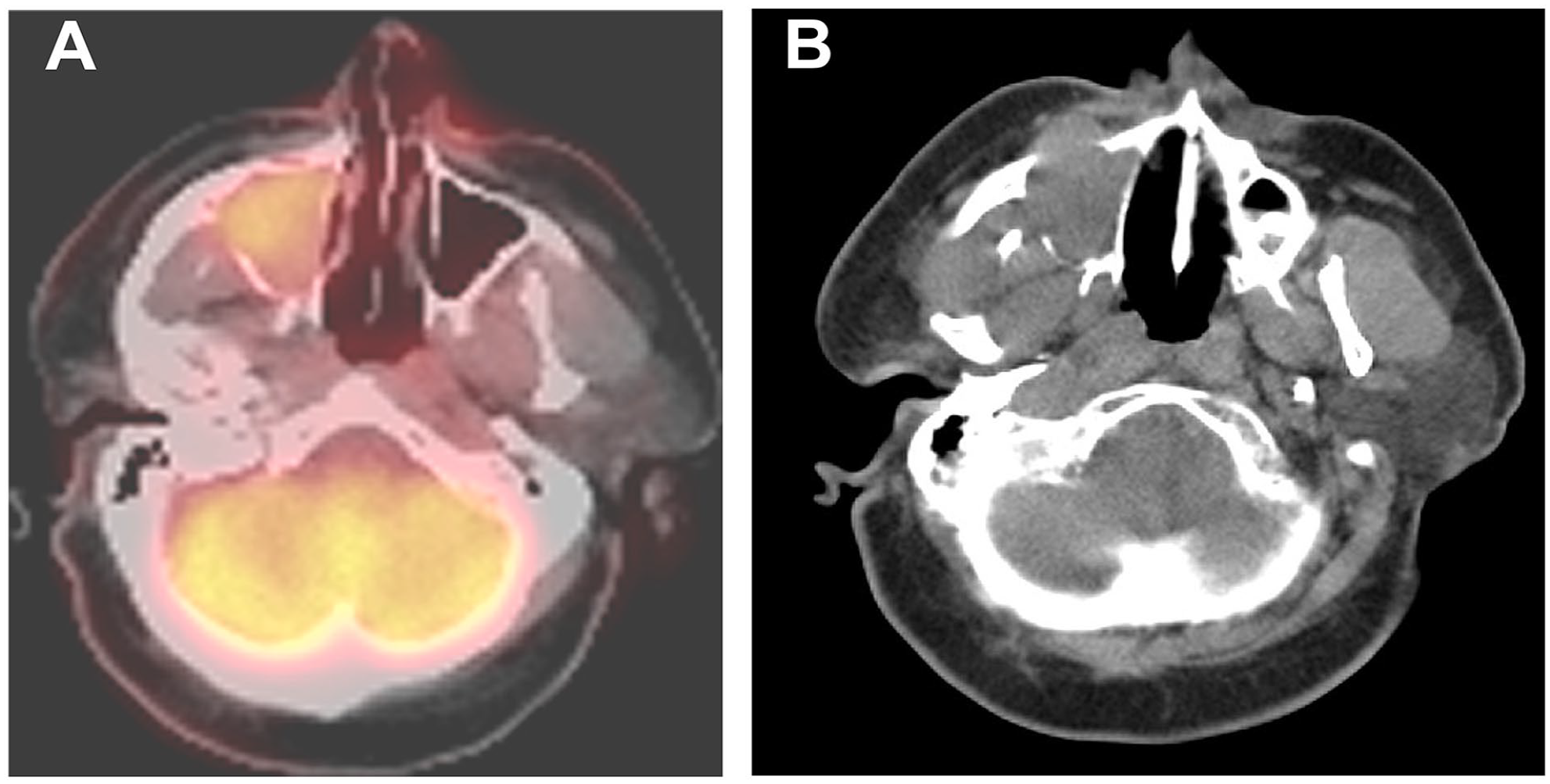
This figure presents side-by-side imaging of the lesion in the right maxillary sinus. Panel A shows an axial fused F-18 FDG PET/CT image, revealing a mildly hypermetabolic lesion occupying most of the right maxillary sinus. Panel B, a companion axial CT image at the same level, depicts the lesion with local osseous erosion—most notably in the anterior wall—and its invasion into the right orbital floor, nasal cavity, and through to the soft tissues of the cheek. F-18 FDG, 18-fluoro-deoxyglucose; PET, positron emission tomography; CT, computed tomography.
The patient subsequently underwent a right maxillectomy and dacryocystorhinostomy without orbital exenteration in a multidisciplinary approach involving oral maxillofacial surgery and plastic surgery. Surgical margins were negative, following which an obturator was affixed by the oral maxillofacial team. Subsequent to an uneventful postoperative phase, the patient was discharged on the first postoperative day.
Microscopically, there was an infiltrative basaloid mass with epithelioid and spindle cell components. The epithelioid component had areas of ameloblastic differentiation with basaloid cells with peripheral palisading, reverse polarization of the nuclei away from the basement membrane and stellate reticulum as well as foci of clear cell change, and squamous differentiation. The cells had a significant degree of atypia with nuclear enlargement, pleomorphism, hyperchromasia, and a high nuclear to cytoplasmic ratio. There was increased mitotic activity with atypical forms as well as tumor necrosis, perineural invasion, and microscopic invasion into the maxillary bone (Figure 3). The spindle cell component had a sarcomatous appearance with areas of cartilaginous differentiation and had a high degree of nuclear atypia (Figure 4). Immunohistochemical stains were interpreted as positive for p63/CK5, p40, CD56, and keratin in the epithelioid component and focally positive in the spindle cell component. p16 was positive and CK7, S100, SOX-10, smooth muscle actin, calponin, chromogranin, synaptophysin, calretinin, and GFAP were negative in both components. Outside consultation was obtained and additional immunostains were positive for SOX-2 and negative for p53 with BRAF, BRG1, and LEF1 intact. The final rendered diagnosis was AC with malignant spindle cell component (sarcomatoid AC).
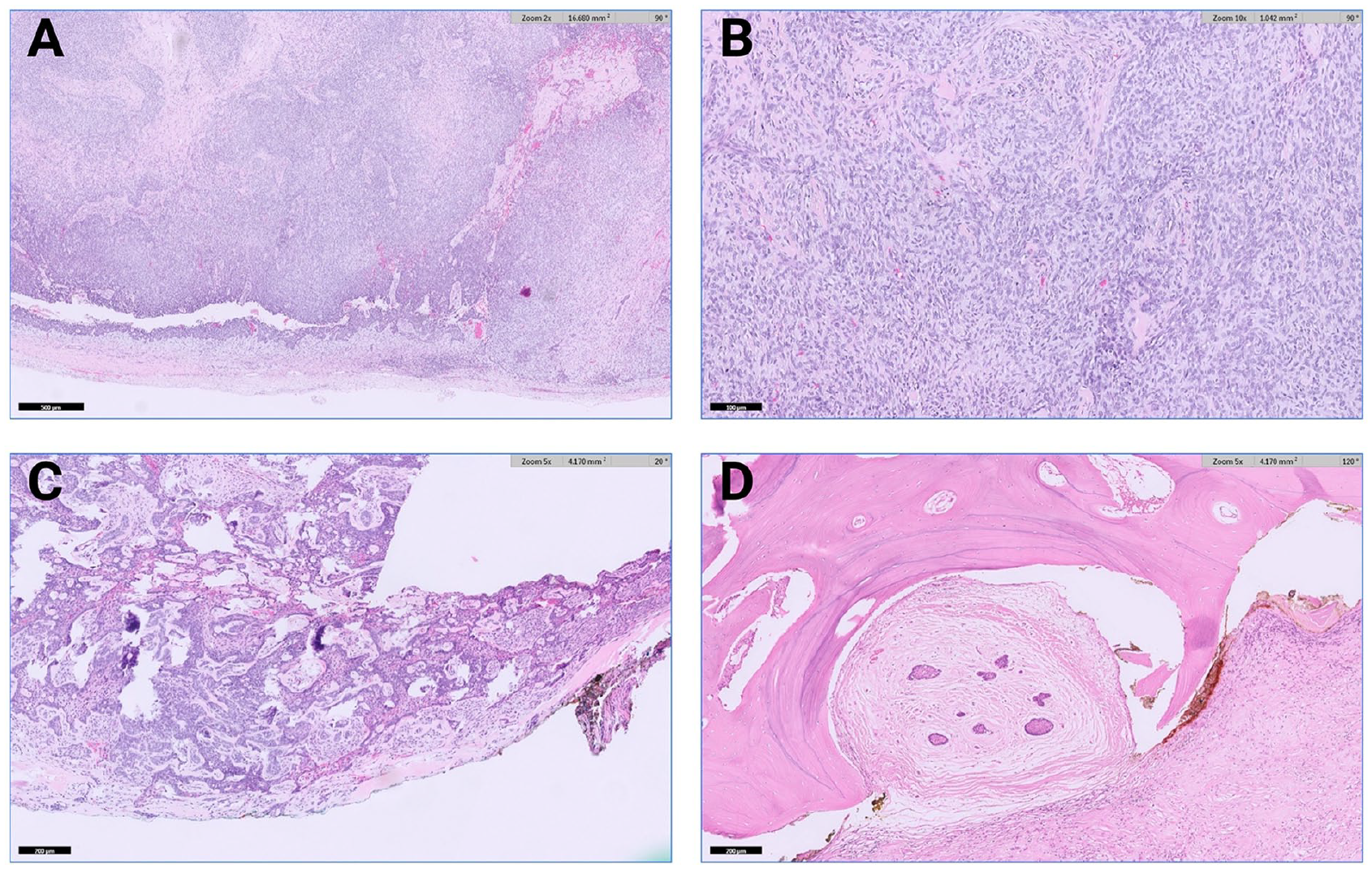
Key histopathological features of the neoplasm. Panel A (2× magnification) shows the overall infiltrating pattern of the basaloid neoplasm. Panel B (10× magnification) highlights the epithelioid component. Panel C (5× magnification) focuses on areas of ameloblastic differentiation alongside focal squamous differentiation. Panel D (5× magnification) demonstrates microscopic bone invasion, underlining the tumor’s aggressive behavior.
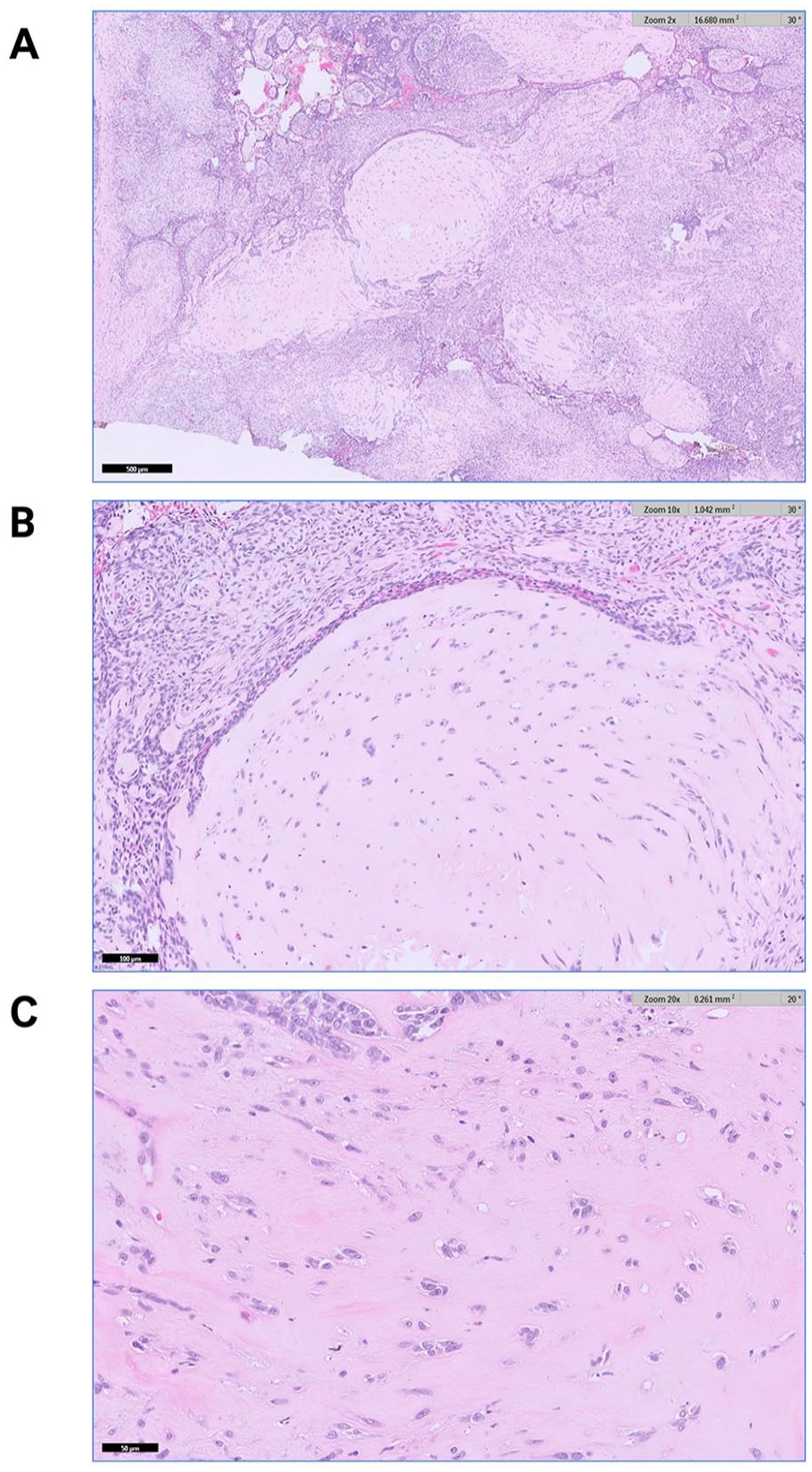
Panels A (2× magnification), B (5× magnification), and C (20× magnification) depict the spindle and epithelioid components of the ameloblastic carcinoma.
One month postoperatively, a neck dissection encompassing levels 1A, 1b, 2A, 3, and 4 was performed due to the aforementioned PET scan findings with negative results. Therefore, the mass was categorized as a T3pN0M0 AC with basaloid, spindle cell, and sarcomatoid traits. The patient received 5 fractions of 600 cGy twice weekly in accordance with tumor board re-commendations.
Twelve months postoperatively, the patient was healing appropriately from maxillectomy and CT scan of neck reaffirmed the absence of recurrent malignancy. Right dacryocystorhinostomy and posterior nasal nerve cryoablation were performed for unremitting epiphora and rhinorrhea with good results (Figure 5).
Twelve-month postoperative computed tomography scan of the neck with contrast demonstrating stable right maxillectomy without evidence of recurrence of malignancy.
Discussion
The term ameloblastic carcinoma and its categorization in the World Health Organization classification system were first proposed by Elzay in the year 1982. 4 In the latest release of the Classification of Odontogenic Lesions from the World Health Organization in 2022, AC was considered a primary odontogenic carcinoma that resembles ameloblastoma, histologically, rather than a malignant counterpart as previously defined in 2017. 5
The 2 and 5 year overall survival rate was determined to be 87% and 69%, respectively, according to one analysis. It was previously thought that AC had equal occurrences in both sexes, but more recent work has indicated a greater likelihood in males with the mandible being considered the most common site of tumor location followed by the maxilla. 6 A study conducted at the China West Hospital of Stomatology, Sichuan University found that of 12 known AC patients, 11 cases were located in the mandible. 7 Thus, the necessitation of a maxillectomy is also of significance due to its lower likelihood and historical presentation. Our patient presented with a complex symptomatology, notably allergic rhinitis and episodic sinusitis, which, on further investigation, was intricately linked to a uniquely extending tumor in the maxillary sinus and its surrounding structures. The mass in the maxillary sinus provides a plausible explanation for many of his chronic symptoms due to its mass effect. The obstruction of mucous drainage pathways likely led to mucous stasis, precipitating recurrent sinus infections. Moreover, sensory numbness and facial edema served as red flag symptoms, indicating a growing mass invading surrounding structures. Specifically, tooth numbness can be attributed to the disruption of cranial nerve V2 by the mass, while facial swelling was caused by the physical expansion of the mass. Thus, while his initial presentation to the clinic was highly suspicious for a mass, his history of sinus infections prior to clinical presentation may have been instigated by an obstructive, growing mass that had not yet attained a size sufficient to cause more overt and concerning symptoms. This case underscores the necessity of a meticulous and interdisciplinary approach to diagnosis and management to ensure optimal treatment outcomes, especially considering the diagnostic challenges posed by the intertwining of diverse symptomatology and tumor extension. The initial diagnosis of T4acN0M0 squamous cell carcinoma with basaloid features which was later revised after significant surgical intervention further underscores the complexity in the diagnosis and categorization of such malignancies.
The decisions made to undergo right maxillectomy, followed by neck dissection and radiation therapy, aligns with the literature’s emphasis of early aggressive surgical intervention. Retrospective analyses have found that the treatment method with the most favorable outcomes is early surgical intervention irrespective of supplementary chemotherapy or radiotherapy. 8 The postoperative course including the development of right epiphora from nasolacrimal duct obstruction and subsequent interventions further underscores the multifaceted challenges and con-siderations in the management of AC and the need for close postoperative monitoring.
From a clinical perspective, our case underscores the necessity of a comprehensive diagnostic approach, especially considering the absence of a visualized mass during the initial nasal endoscopy. Despite a history of allergic rhinitis and sinusitis, the patient’s asymmetric facial edema and paresthesia were pivotal in prompting further investigation. These red flag symptoms underscore the imperative of astute clinical and radiographic evaluation, amid seemingly explanatory historical data, to address the underlying pathology effectively. Our case also underscores the importance of a multidisciplinary approach, bringing together expertise from pathology, plastic surgery, oral surgery, radiation oncology during comprehensive tumor board discussion to ensure optimal patient care. Furthermore, it is essential to consider the potential implications of the patient’s chemical exposure in the dry-cleaning industry, especially to agents like perchloroethylene, on the development of AC. Notably, perchloroethylene exposure has been associated with an increased risk of head and neck cancer in certain populations. 9 This case offers valuable insights into the potential presentation of AC including its challenges in diagnosis and management, and vigilant postoperative care should be prioritized and understood as essential components in the management of such cases.
Footnotes
Acknowledgements
Not applicable.
Data Availability
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Patient Consent
Informed consent was obtained from the patient for the publication of this case report.
Trial Registration
Not applicable.
Grant Number
Not applicable.