
Abstract
Keywords
Introduction
Telemedicine, as defined by the World Health Organization, is the delivery of healthcare services by physicians using information and communication technologies (ICT) to help diagnose, treat, and prevent disease. 1 ICTs include computers, the internet, broadcasting technologies, mobile, and videoconferencing. 1 The use of telemedicine has been steadily growing, with an estimated expansion from 0.35 million to 7 million users between 2013 and 2018. 2 Despite the availability of telemedicine for patients at more than half of the American hospitals prior to the COVID-19 pandemic, widespread adoption was limited partly due to provider hesitation,3,4 insurance coverage restrictions for telehealth services, 5 and targeted focus on rural healthcare delivery.6,7 This changed during the outset of the SARS-CoV-2 (COVID-19) pandemic when national emergency declarations resulted in expanded telehealth coverage. 8 Telemedicine experienced unprecedented, widespread adoption. In fact, 1 week at the outset of the pandemic, the number of telehealth visits experienced a 154% increase compared to a similar period during the year prior. 9 While telemedicine became pervasive, it was not well understood in terms of patient perspective.
Studies in various patient populations suggest that telemedicine access and use can be affected by socioeconomic factors such as education, occupation, age, and income.10-12 This is supported by key literature findings published prior to the COVID-19 pandemic, indicating that users of telehealth and electronic patient portals tended to be young, of higher socioeconomic status, urban-dwelling, and White.5,13-17 Larger single-center observational studies of telehealth use have revealed persistent disparities in initial telehealth adoption with decreased use associated with older, Black, Hispanic, and publicly insured populations.3,18,19 When given a choice, individuals with these demographics are more likely to request in-person appointments.20,21 These findings likely reflect the observed digital divide affecting individuals who are older, Black or Hispanic, disabled, or of lower educational attainment. 19
Within otolaryngology—head and neck surgery, much still needs to be understood on the effects of the rapid telehealth deployment on access to care, especially in the urban setting. Previous studies have examined access disparities for head and neck cancer and pediatric otolaryngology care in nonurban populations during the initial COVID-19 surge, suggesting an effect of insurance status and income level on telehealth use.22,23 Few studies have investigated the use of telemedicine in otolaryngology at different time points of the COVID-19 pandemic in an urban setting in the United States. 24 However, there is limited understanding of the association between demographic characteristics and access to telehealth in otolaryngology across these time periods. Understanding how telemedicine access has evolved across the pandemic can help identify persistent barriers to address and develop interventions to improve access. In this study, we assessed the sociodemographic profiles of patients accessing otolaryngology telemedicine services at a single institution in New York City during the outset and later periods of the COVID-19 pandemic. We hypothesized that individuals with disadvantaged sociodemographic characteristics used otolaryngology telemedicine services less, reflecting disparities in access.
Methods
Institutional review boards approved the collection of study data at New York Presbyterian-Weill Cornell, a tertiary academic medical center in New York City. This study was a single-center, retrospective cohort comparison study.
Study Sample
This study included 4 cohorts of adult patients seen either in person or via telemedicine at a tertiary urban medical center otolaryngology practice during four 8 week time periods: 1 year before the pandemic (prepandemic: March 17, 2019-May 11, 2019), at the onset of the pandemic (pandemic onset: March 17, 2020-May 11, 2020), 6 months after the start of the pandemic (late pandemic 1: September 7, 2020-October 30, 2020), and another year later (late pandemic 2: September 7, 2021-October 30, 2021). These pandemic time periods overlayed with new positive COVID-19 cases in New York City are shown in Figure 1. Telemedicine visits in our study were defined as any telephone or video encounter between patients and physicians. The video and teleconferencing applications are integrated in the portal application for patients and in the electronic medical record for providers. 25
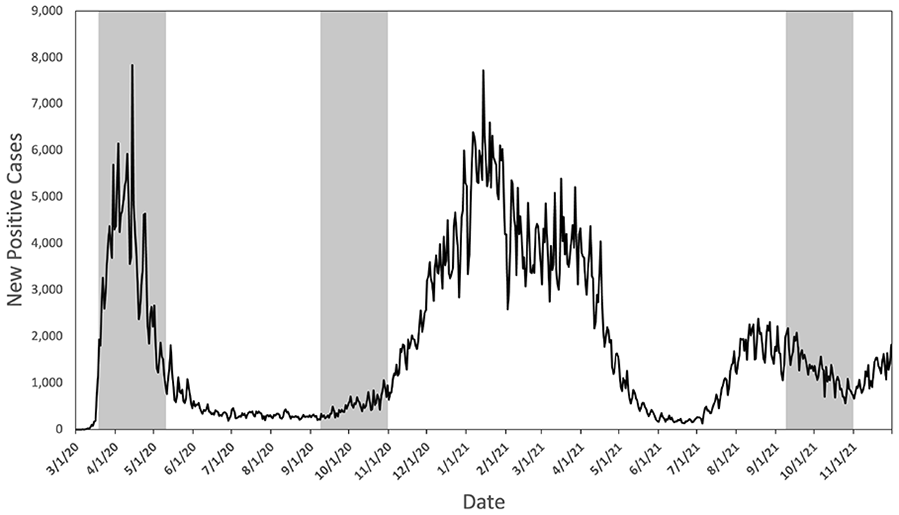
Positive COVID-19 cases from March 1, 2020, to December 1, 2021, in New York City. Pandemic time periods analyzed in this study are shaded in gray.
Study Variables
Variables included in this study were date of birth, sex, race, primary language, portal status, zip code, service period, insurance payor name, and visit type (telemedicine vs in-person). Telemedicine visits included both audio and video visits that could not be separated for analysis because the data were not well captured. Income estimates were derived from the US Census data 26 by linking zip code to median income. Income data were downloaded for each year separately (2019-2021) and merged with the corresponding rows in the final dataset. Race data were extracted from the electronic health record and categorized as American Indian or Alaska Native, Asian or Pacific Islander, Black or African American, White, or other combination not described. Race data were collected in conjunction with other sociodemographic data to help assess whether it served as a social determinant for access to telemedicine care in otolaryngology. Patients who identified as American Indian or Alaska Native were grouped with patients of other race combinations not described during regression analysis due to a small sample size. Ethnicity, sexual orientation, and gender identity were not included in our data set because these variables were not well populated in our electronic health record, consistent with other institutions, suggesting these data are systemically lacking.27,28
Statistical Analysis
Descriptive variables were summarized by mean (±SD) for continuous variables and n (%) for categorical variables. Where appropriate, chi-squared, Kruskal-Wallis, and Wilcoxon signed-rank tests were used to compare various demographic factors of interest between the different cohorts. A logistic regression model was estimated to assess the association between the modality of care as a dependent variable, controlling for patient sex, race, age, income, portal status, primary language, and insurance coverage type. Analyses were conducted using R version 3.6.2 (R Foundation for Statistical Computing), and statistical significance was determined using 2-tailed tests at P < .05. 29
Results
Study Population and Baseline Characteristics
A total of 22,147 unique patients and 46,131 otolaryngology outpatient appointments were contained in the initial data set. After excluding visits with patients over the age of 110, patients under the age of 18 years, and patients with incomplete race data, and visits not relevant to our study (allied health/nurse, anticoagulation, home visit, surgery encounters, and erroneous encounters), the final sample included 14,240 (64.3%) unique patients with an average of 2 visits during the study periods, resulting in a total of 29,457 (59.5%) observations that were collectively analyzed across all 4 timeframes.
Among all observations, 27,918 (94.8%) were in-person visits and 1539 (5.2%) were telemedicine visits. No patients during the prepandemic timeframe underwent a telemedicine visit. The proportion of telemedicine visits fell from 14.3% during the onset of the pandemic to 7.3% during late pandemic period 1 and 4.1% during late pandemic period 2 (Figure 2). The patients in this study were predominantly female (57.9%) with a median age of 58 years (range, 18-107 years). Baseline characteristics of the patients associated with in-person and telemedicine visit type during the 4 time periods are summarized in Table 1.
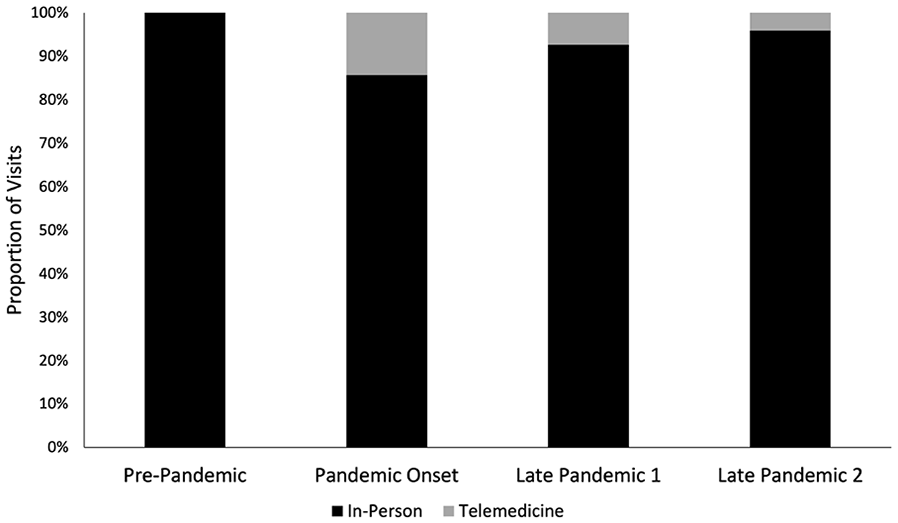
Distribution of in-person and telemedicine visits during four 8 week time periods surrounding the COVID-19 pandemic. Prepandemic (March 17, 2019-May 11, 2019), pandemic onset (March 17, 2020-May 11, 2020), late-pandemic period 1 (September 7, 2020-October 30, 2020), and late pandemic period 2 (September 7, 2021-October 30, 2021).
Baseline Characteristics of Patients Undergoing Otolaryngologic In-Person and Telemedicine Appointments.
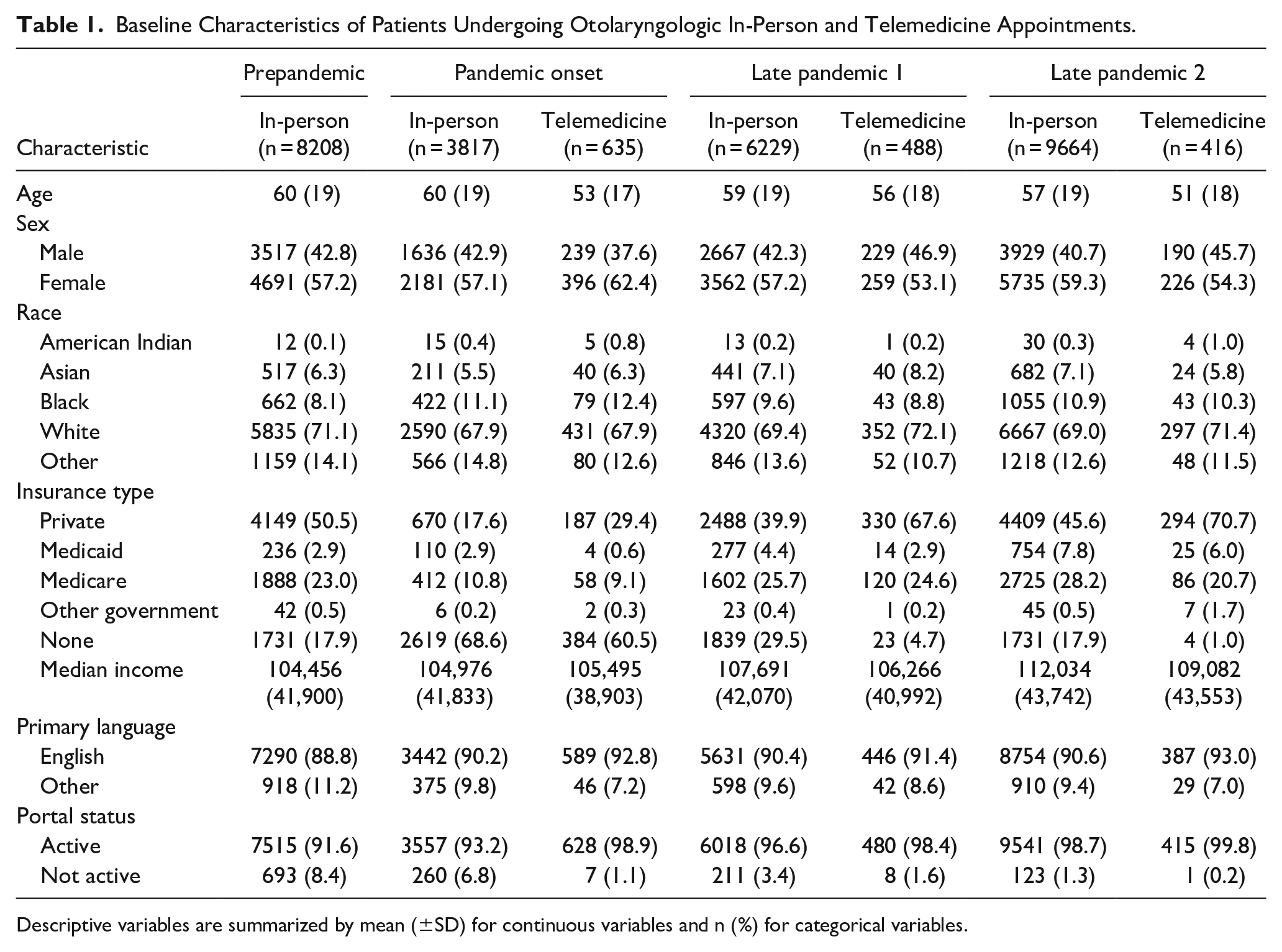
Descriptive variables are summarized by mean (±SD) for continuous variables and n (%) for categorical variables.
Univariable Analysis of Sociodemographic Risk Factors on Telemedicine Visits
A chi-square test showed that there was no significant difference between the proportion of telemedicine visits undergone by males versus females (P = .85). A Kruskal-Wallis test showed that patients seen in person were older than those using telemedicine (P < .001). Post hoc analysis using a pairwise Wilcoxon rank-sum test with Bonferroni correction revealed that there was no significant difference in age between patients during the pandemic onset and prepandemic (P = .50), late pandemic 1 and pandemic onset (P = .99), and late pandemic 1 and prepandemic service periods (P = .32). However, there was a significant difference in age between patients in late pandemic period 2 and the earlier service periods (P < .001), with patients being older during the earlier service periods.
A chi-squared test followed by a pairwise proportion test with Bonferroni correction showed a statistically significant difference in the distribution of insurance payors across time periods (P < .001) and between telemedicine and in-person visits (P < .001). The proportion of visits by patients with Medicare significantly decreased during the pandemic onset (from 23.0% to 10.6%) but increased again in the late pandemic periods (25.6% in late pandemic 1 and 27.9% in late pandemic 2). The proportion of visits by patients with Medicaid decreased during the pandemic onset (from 2.9% to 2.6%) but increased well above prepandemic levels in the late pandemic periods (4.3% in late pandemic 1 and 7.7% in late pandemic 2). The proportion of visits by patients with private insurance had a significant decrease during the pandemic onset (from 50.5% to 19.2%) but increased again in the late pandemic periods (42.0% in late pandemic 1 and 46.7% in late pandemic 2), although not reaching the prepandemic level. The proportion of visits by patients with no insurance increased sharply during the pandemic onset (from 17.9% to 67.5%) and then decreased in the late pandemic periods (27.7% in late pandemic 1 and 17.2% in late pandemic 2), falling well below the prepandemic level. Compared to in-person visits during the pandemic, telemedicine visits included a higher proportion of patients with private insurance (52.7% vs 38.4%) and a smaller proportion with government (20.6% vs 30.2%) or no insurance (26.7% vs 31.4%).
Race was significantly different across the different time periods (P < .001) and between in-person and telemedicine visits (P = .009). During the onset of the pandemic, there was a slightly higher proportion of Asian (6.3% vs 5.5%) and Black (12.4% vs 11.1) patients among telemedicine appointments than in-person appointments. During the late pandemic periods, the proportion of Black patients among telemedicine appointments fell below than that among in-person appointments (8.8% vs 9.6% in late pandemic 1 and 10.3% vs 10.9% in late pandemic 2). The proportion of White patients among telemedicine appointments was the same or greater than in-person appointments across all time periods. Patients who had their portal accounts activated were more likely to use telemedicine (P < .001). While primary language was not significantly different across the time periods (P = .08), there were significant differences in primary language between telemedicine and in-person visits (P = .002). Similarly, income was significantly different between the time periods (P < .001) with median income increasing from the prepandemic to late pandemic periods, but there were no differences between those who had telemedicine visits compared to in-person visits (P = .16).
Multivariable Analysis of Sociodemographic Risk Factors on Telemedicine Visits
Logistic regression analysis is summarized in Figure 3. Age was found to have a significant negative effect on the likelihood of using telemedicine, with each additional year of age associated with a decrease in telemedicine use, holding all other variables constant (P < .001). Individuals with private insurance were more likely to use telemedicine compared to government insurance (Medicare, Medicaid, or other form of government insurance) after controlling for other factors (P < .001), while those with no insurance were not significantly more likely to use telemedicine compared to government insurance (P = .31). Portal status was also found to be significantly associated with the likelihood of using telemedicine. Participants with portal access were more likely to use telemedicine compared to those without portal, holding all other variables constant (P < .001). On the other hand, female sex (P = .36), non-White race (P > .05 for all groups), income (P = .09), and English as primary language (P = .09) were not found to have a significant effect on telemedicine use on multivariable analysis.
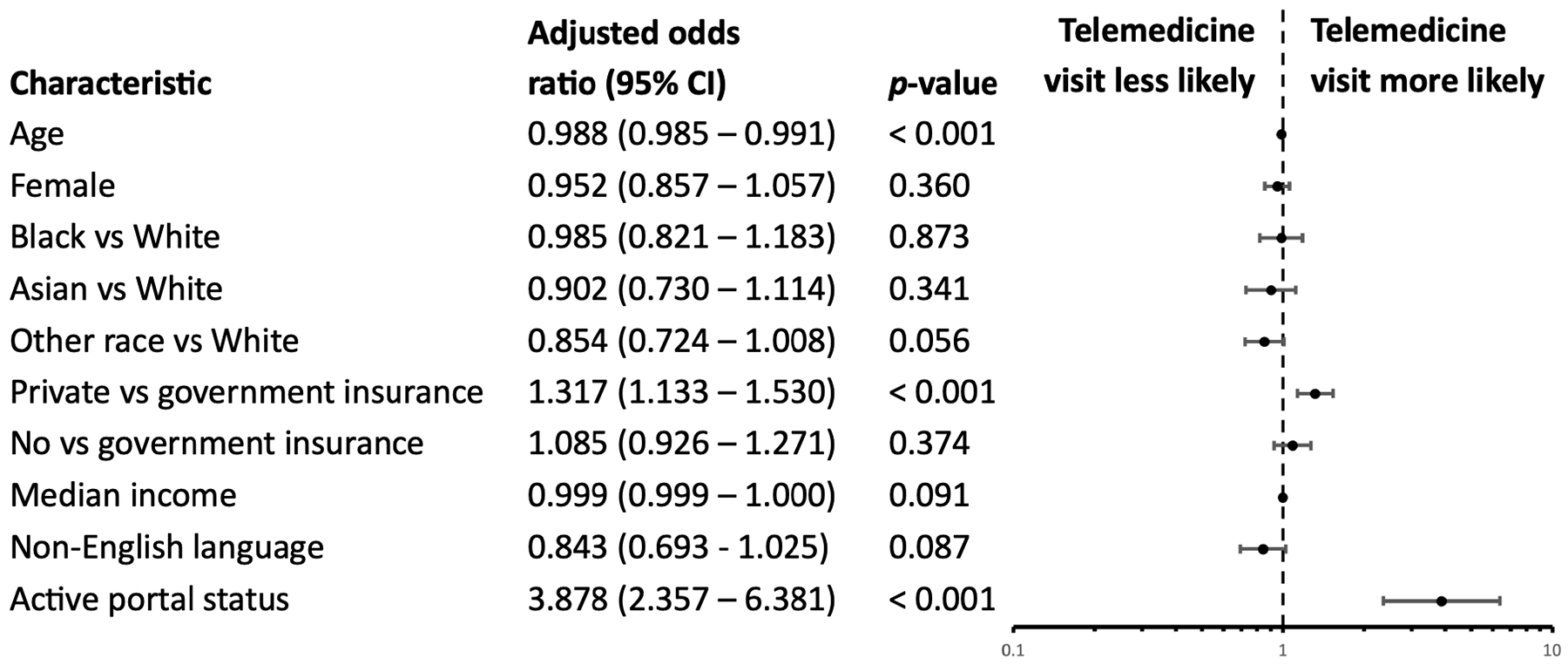
Multivariable logistic regression for utilization of telemedicine compared to in-person otolaryngologic care across the pandemic.
Discussion
Outpatient nonurgent evaluation in otolaryngology—head and neck surgery was particularly affected due to initial concerns about increased risk of COVID-19 transmission during routine nasopharyngoscopy via aerosolization of viral particles.30,31 Telemedicine practice rapidly expanded as a safe alternative to in-person visits, with patient satisfaction, visit show rates, and completion rates noted to be significantly higher across all otolaryngologic subspecialties compared to that of in-person visits before the pandemic. 24 Some studies have shown that certain subspecialities within otolaryngology, such as laryngology, speech-language pathology, and head and neck oncology, may derive greater benefits from telehealth systems.32,33 However, the digital divide has the potential to worsen disparities that already exist with regard to access to and utilization of technology. 34 Telemedicine rapid deployment during the pandemic provided a unique opportunity to study equity issues related to access for vulnerable and underserved populations.
Among sociodemographic characteristics associated with lower adoption of telemedicine during the COVID-19 pandemic, older age has been independently associated with both lower video use and lower telemedicine. This is thought to be in part due to lower internet availability, privacy concerns surrounding digital health use, and slower rates of technological adoption.35-38 Comorbid conditions including impaired eyesight, motor skills, and hearing can additionally make telemedicine visits challenging for older patients.39,40 Consistent with these prior findings, we found that, across the COVID-19 pandemic, the average age of patients who attended otolaryngologic telemedicine appointments was significantly lower than those who attended in-person appointments. Multivariable analysis showed that each additional year of age was associated with a decrease in telemedicine use. In addition, older patients have been shown to use online portals less, making it more difficult to engage in telemedicine. 37 We also found that patients with active portals were significantly more likely to have a telemedicine appointment than patients who did not have an active portal. These trends suggest that focusing on lowering barriers to digital health for older adults is an important step in mitigating differential access to telemedicine in otolaryngology. Prior studies have demonstrated high level of acceptance and satisfaction among elderly patients effectively engaging with telemedicine thanks to its convenience. 37 Providing help with setting up an active portal may facilitate access in this age group.
Patients with Medicaid and Medicare as well as patients with lower income requiring otolaryngologic care have had significant improvements in appointment completion rates after transitioning to telemedicine visits. 24 In our institution, while there were no differences between the average income of patients utilizing telemedicine versus in-person visits, patients with private insurance were more likely to undergo a telemedicine appointment than patients with government insurance. This was despite the enactment of the 1135 wavier authority and Coronavirus Preparedness and Response Supplemental Appropriation Act by the Centers for Medicare & Medicaid Services, which helped expand coverage for telemedicine visits under Medicare. 41 Older age among Medicare recipients may in part explain the lesser use of telemedicine in the cohort with government insurance, although understanding other possible barriers requires further investigation. The sharp rise in patients with no insurance in our cohort is likely due to the pandemic-driven recession that caused millions of Americans to lose their health insurance in 2020. 42 These levels returned to below prepandemic levels in the later pandemic. Patients with no insurance made up a significantly smaller proportion of telemedicine users in our cohort, underlying the importance of insurance coverage for access to telemedicine in the United States.
Previous studies have suggested that use of telemedicine services for Asian, Black, and Latinx patients is significantly lower compared to White patients. 43 Barriers to access include poorer quality patient-doctor relationships and more frequent negative interactions with providers due to bias, likely worsened by increased racism against subgroups during the pandemic. 44 Black and Latinx individuals are disproportionally represented among essential workers and had longer in-person work hours during the pandemic, possibly contributing to limited access to telemedicine. In contrast with prior studies, however, Black patients in our cohort scheduled and attended more telemedicine visits overall compared to in-person visits. 43 While there were differences in racial distributions of patients receiving otolaryngologic care across different time periods, we did not find any significant differences between racial groups in the likelihood of undergoing a telemedicine appointment. Being a non-English speaker has been independently associated with lower telemedicine visit completion. 22 However, we did not find a difference in the likelihood of undergoing a telemedicine appointment between English and non-English speakers. Despite these findings, we must continue to be intentional with how telemedicine is implemented to remove any possible barriers for historically marginalized groups.
Our study demonstrates decline in telemedicine use across the selected periods of the COVID-19 pandemic at our institution in New York City. This decline has been attributed to patient and physician preference for face-to-face interactions over remote visits, especially for more complicated patients, and increasing comfort in hospitals and other in-person healthcare settings. 45 The decline may also be attributed to the lack of reimbursement associated with telemedicine, 46 especially within the field of otolaryngology where providers are unable to perform in-office endoscopies and procedures. Furthermore, many surgeons are not trained to assess patients via telemedicine and report that investing resources to learn how to engage with patients meaningfully through telemedicine would be too burdensome, unsafe, and inefficient. 47 New federal data from the National Electronic Health Records Survey show that fewer surgical specialists felt they can provide similar quality care via telemedicine than primary care and medical specialists. 48
However, while rates of telemedicine use have declined, they remain substantially higher than prepandemic, as evidenced by the lack of any telemedicine appointments during the prepandemic period at our institution. Moving forward, telemedicine will likely continue to play a role in otolaryngologic care. Telemedicine has the power to expand otolaryngologic services to underserved areas and populations by breaking down geographic barriers to care access. It can also potentially help reduce healthcare spending, medication nonadherence, and unnecessary emergency room visits. For telemedicine to be scalable and sustainable, we will need telemedicine platforms that are simple to use and accessible to all patients and specific tools for visualization for otolaryngologists to conduct examinations remotely. Furthermore, we need to prioritize teaching future generations of physicians how to provide quality care via telemedicine and have appropriate documentation, follow-up, adverse event reporting, and patient privacy protocols in place. 49
Our study has several limitations. Despite a large sample of outpatient otolaryngologic appointments, the analysis was confined to a single tertiary medical center resulting in unique demographics that may not be representative of all outpatient otolaryngologic care. Appointments that were cancelled before the visit could not be counted, leading to potential underestimation of the number of patients who could not be seen in person at the outset of the pandemic. The incidence of COVID-19 cases in New York City differed between the studied time periods, which may have affected telemedicine use. We also did not analyze audio versus video visits because it was not captured in our data. Studies show that vulnerable patients tend to participate more in audio visits, which are not as great for patient-provider relationship and quality of care. 50 Our analysis of differences in telemedicine use between racial and ethnic groups was limited because we did not include ethnicity or the Latinx population as its own subgroup because these fields were not well populated in our data set. Zip code was used to estimate income, limiting accurate representation of income across the different time periods. Furthermore, the nature of conditions treated including chief complaints, subspecialty, diagnoses, new versus return status, and acuity were not explored in this study. Future work should explore these disease-related aspects of care to better understand the role of telemedicine versus in-patient visits in otolaryngology—head and neck surgery.
Conclusions
At our institution, we found significant differences in sociodemographic characteristics between patients undergoing in-person versus otolaryngologic care in the setting of COVID-19 across different time periods before and during the pandemic, reflecting possible barriers to care. Telemedicine may be a viable alternative to in-person visits for certain types of otolaryngologic care. However, further study is needed to identify specific barriers and develop interventions to improve access for vulnerable patient populations.
Footnotes
Author Contributions
YS: concept and design; acquisition, analysis, and interpretation of data; statistical analysis; writing of manuscript; and critical revision of the manuscript for important intellectual context. KA: concept and design; acquisition, analysis, and interpretation of data; statistical analysis; writing of manuscript; and critical revision of the manuscript for important intellectual context. SSB: acquisition, analysis, and interpretation of data; and writing of manuscript. AR: concept and design; acquisition, analysis, and interpretation of data; writing of manuscript; critical revision of the manuscript for important intellectual context; administrative, technical, or material support; and supervision.
Data Availability
The data that support the findings of this study are available from the corresponding author, AR, on reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Anaïs Rameau owns equity of Perceptron Health, Inc. Anaïs Rameau is a medical advisor for Sound Health Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Anaïs Rameau was supported by a Paul B. Beeson Emerging Leaders Career Development Award in Aging (K76 AG079040) from the National Institute on Aging and by the Bridge2AI award (OT2 OD032720) from the NIH Common Fund.
Ethical Approval
This study was approved by the Weill Cornell Medical College Institutional Review Board (20-05022166) on February 24, 2022.
Informed Consent
No informed was obtained, as this was a retrospective study.