
Abstract
Introduction
Thyroid carcinoma is the most common endocrine malignancy, and in the United States, its incidence has increased by greater than 3% annually. 1 Differentiated thyroid cancer represents around 95% of cases with papillary thyroid carcinoma (PTC), follicular thyroid carcinoma (FTC), and oncocytic thyroid carcinoma falling under this category. 2 Other subtypes include medullary thyroid carcinoma (MTC) and anaplastic thyroid carcinoma (ATC), which represent 1% to 5% percent of all thyroid carcinomas collectively. 1
The cervical lymph nodes are the most common site of thyroid carcinoma metastases and distant metastases are less common. 3 When they do occur, distant metastases typically involve the lungs, bones, and brain. 4 There have also been cases of cutaneous metastases, with the latest review on this subject being published in 1997 by Dahl et al. 5 Cutaneous metastasis is an uncommon finding and is often a marker for widely disseminated neoplasm. 5 Gross appearance of cutaneous metastases is variable, with studies reporting slow-growing nodules, erythematous papules, and ulcerated scrotal lesions.5-7 Lesions may not be painful or itchy and can be mistaken for a pimple or other harmless nodule. 8 Furthermore, histopathological analysis can be complicated as primary cutaneous malignancies may share similar features. 6
The current study aims to update and better elucidate the demographic, clinical, and histopathologic findings of patients with cutaneous metastases from thyroid carcinoma.
Methods
A review of the literature was conducted using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The search queried the Medline/PubMed, Cochrane, and Scopus databases using the terms (“thyroid cancer” OR “thyroid carcinoma”) AND (“metastasis” OR “metastatic”) AND (“skin” OR “dermal” OR “cutaneous”) to review the existing literature from inception to May 2023. Reference lists were checked to identify additional relevant studies. Excluded from the analysis were commentary articles and those that did not include information on the patient’s demographics and clinical and histologic findings of cutaneous metastases. Articles were also excluded if individual data were inextricable.
For full-text analysis, data extracted included patient age at diagnosis of cutaneous metastases, patient sex, thyroid carcinoma histotype, location of metastases, the time interval between diagnoses of thyroid carcinoma and cutaneous metastases, and overall survival from the time of cutaneous metastases (Figure 1). Descriptive statistics, including frequencies and percentages, were used to report demographic and clinical information.
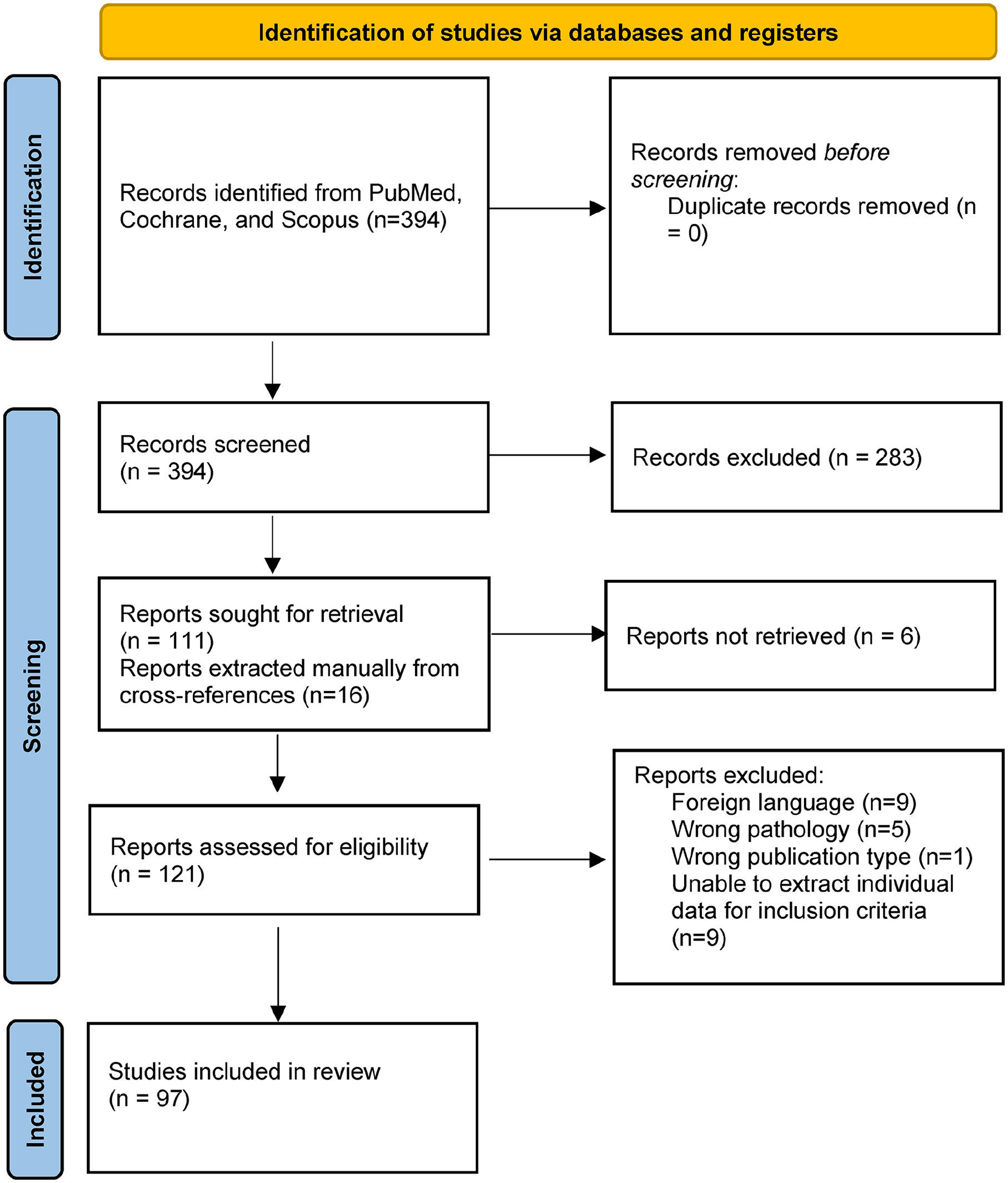
PRISMA 2020 flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Results
Study Selection
Database searches and manual cross-reference searches yielded 394 citations across 3 databases. After a review of the suitability of inclusion, 127 articles, including those extracted manually after reference lists, were checked to identify additional relevant studies. After full-text review, 30 articles were excluded because (1) full-text reports were not able to be obtained, (2) articles were published in a non-English language, (3) individual data were unable to be extracted from reports of many patients, (4) pathologies were not thyroid carcinoma, or (5) the publication was not the correct publication type. A total of 97 articles met the inclusion criteria after full-text review and were included yielding 136 patients for analysis.
Patient Characteristics
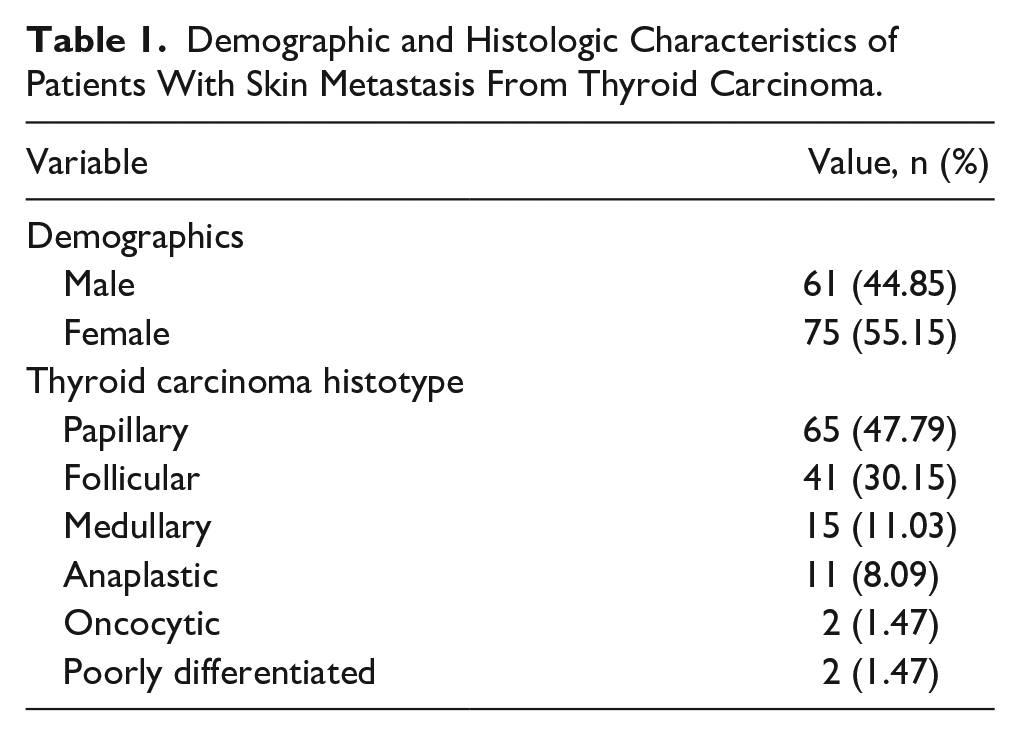
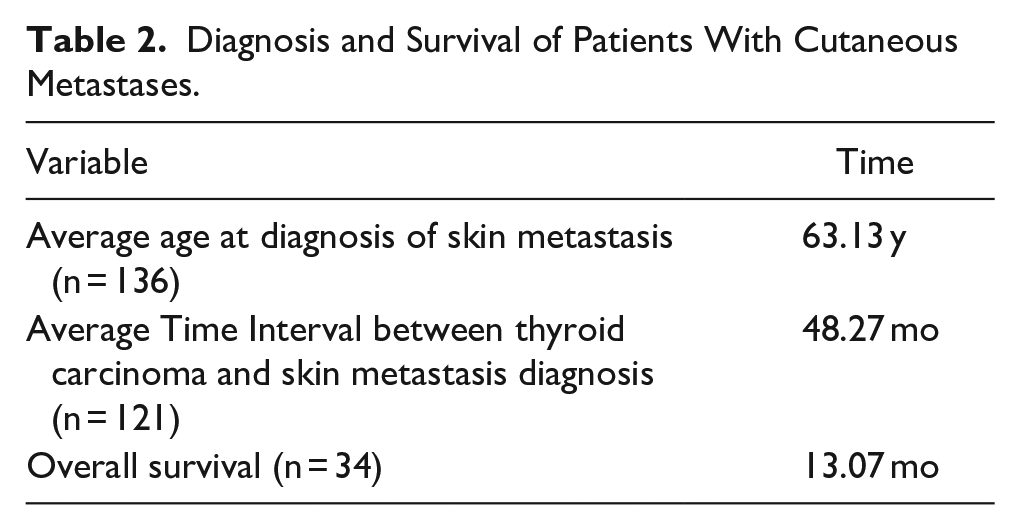
One hundred thirty-six distinct cases of cutaneous metastases from thyroid carcinoma were identified in the literature from 1966 to 2023. Patients’ ages at diagnosis of cutaneous metastases ranged from 21 to 95 years with an average age of 63.13 years. Our review showed slightly more females (n = 75/136, 55.15%) than males (n = 61/136, 44.85%).
Histology Findings
Of the pathologies reported, papillary carcinoma was the most commonly reported histotype (n = 65/136, 47.79%), followed by 41 FTC, 15 MTC, 11 ATC, 2 oncocytic thyroid carcinomas, and 2 poorly differentiated cases.
Clinical Findings
The relative time from diagnosis of cutaneous metastases to the diagnosis of thyroid carcinoma was reported on 130 patients with 95 patients being diagnosed with cutaneous metastases after their diagnosis of thyroid carcinoma, 33 patients being diagnosed at the same time, and 2 patients presented with cutaneous metastases before primary thyroid malignancy. A more specific time interval between both diagnoses was reported in 121 patients and was 48.27 months.
On review of the literature, there were different locations of cutaneous metastases. If metastases were present in more than 1 body area, the patients were considered to have diffuse cutaneous metastases. The scalp was the most common location of metastases (n = 48). However, there were 22 cases with diffuse metastases, 10 of which involved the scalp, adding additional cases of scalp metastases to the cohort. After the scalp, the most commonly reported locations were the neck (n = 33), chest (n = 14), and face (n = 10). Other locations included the back (n = 4), thigh (n = 1), sacrum (n = 1), abdomen (n = 1), inguinal region (n = 1), and hip (n = 1).
Out of 136 patients, 99 reported other sites of metastases. The most common sites of metastases were the lungs (n = 57), lymph nodes (n = 50), bone (n = 45), brain (n = 15), and liver (n = 14). Data on overall survival were not available in the majority of cases. Thirty-four patients had a reported time of death. The overall survival was 13.07 months from the time of diagnosis of cutaneous metastases. Of these patients, the histotypes were as follows: 10 MTC, 10 PTC, 9 ATC, and 5 FTC. In 5 of these patients (2 PTC, 1 MTC, 2 FTC), the cutaneous biopsy findings showed de-differentiation. Of these, 3 showed poorly differentiated carcinomas and 2 showed anaplastic carcinomas. Patients’ demographic and clinical information are summarized in Tables 1 and 2 and Figure 2.
Demographic and Histologic Characteristics of Patients With Skin Metastasis From Thyroid Carcinoma.
Diagnosis and Survival of Patients With Cutaneous Metastases.
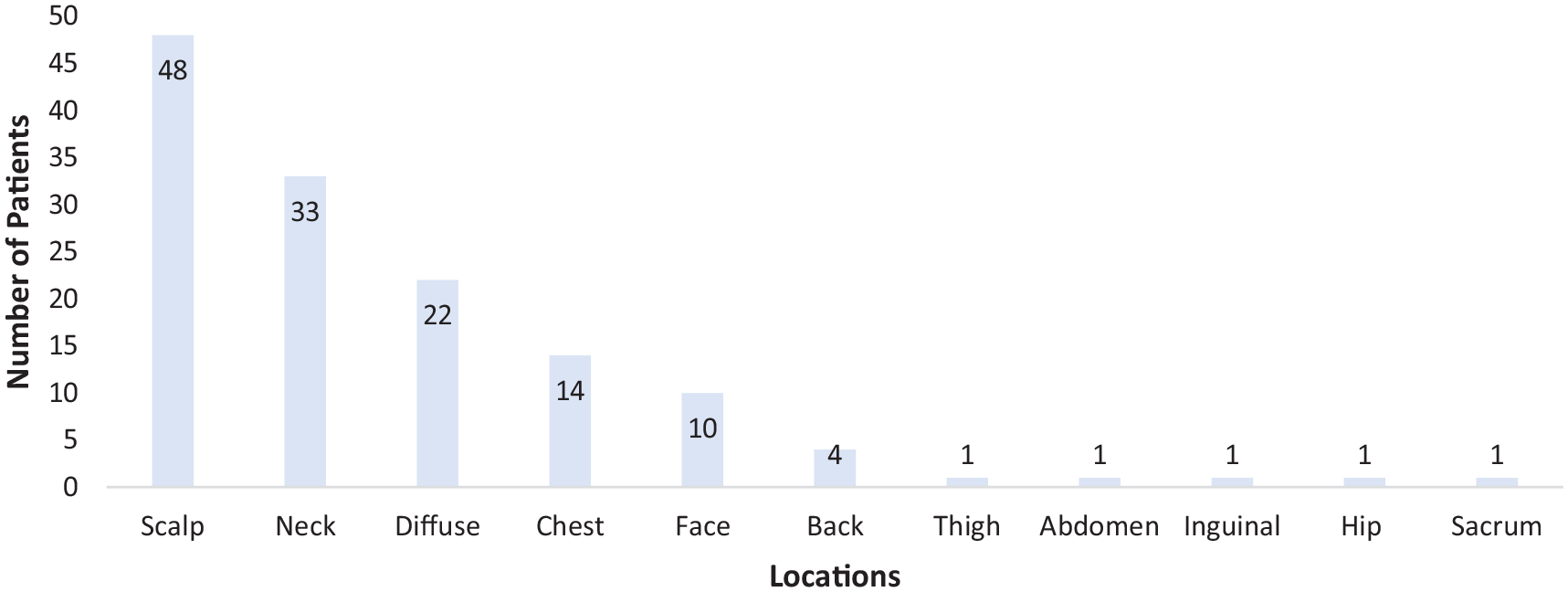
Locations of cutaneous metastases.
Discussion
Cutaneous metastases from carcinoma are relatively uncommon, but they are essential to recognize. 9 The most common malignancies to metastasize to the skin are cancers of the breast, lung, melanoma, and oral cavity.10-12 Cutaneous metastasis from thyroid carcinoma is a rare manifestation. In the present review of 136 cases in the literature of cutaneous metastases from thyroid carcinoma, the average age at diagnosis of metastases was 63.13 years, and the most common site was the scalp.
MTC and ATC are known to have higher distant metastasis rates than papillary and follicular carcinoma.3,13-15 Malignant neoplasms also typically metastasize to internal organs rather than the skin. 12 However, similar to our study, Dahl et al 5 reported that papillary carcinoma has the most significant preponderance for cutaneous metastases, and in our study, nearly half of the patients had PTC. In contrast, Koller et al 16 published a case series in 2009 and reported FTC as being more common. Although thyroid carcinoma is more prevalent in females, cutaneous metastases do not seem to have a sex predominance as 55% of the patients in our study were female. 1
Cutaneous metastases as the first sign of thyroid carcinoma are also not uncommon. In our study, 33 patients (24.26%) presented with skin metastasis as the first sign of an underlying malignancy, diagnosed at the same time as primary thyroid carcinoma. Our study even found 2 cases where the cutaneous metastases preceded the thyroid carcinoma diagnosis.17,18 Our study aligns with current literature that reports the scalp as the most common site of metastases. 5 From our study, cutaneous metastases can present as solitary or multiple lesions.
Currently, the pathophysiology of cutaneous metastasis from thyroid carcinoma is not clear. However, there are hypotheses about this, including the head and neck region, particularly the scalp, being the most common site of metastases due to the highly vascular network in this region. 19 Lymphatic and hematogenous spread are common routes of cutaneous metastases. 20 In response to external signals, neoplastic cells proliferate, undergo angiogenesis, and invade nearby tissues.12,21 For thyroid carcinoma, some reports also propose that metastases, particularly those found on the neck, result from needle tract seeding after fine needle aspiration or contamination during surgery.22,23 While the exact cause is not definitively known, if this is the case, it is possible that some of the neck lesions reported were local recurrences rather than true metastases.
Tumor genetics may also play a role in metastases. The BRAFV600E mutation is the most common mutation in PTC and may be associated with more aggressive features. 24 Erickson et al 25 evaluated genetic mutations in 16 cases of thyroid carcinoma metastatic to the skin and found that a BRAFV600E mutation was present in 5 of 11 cases of PTC and none of the cases of FTC. However, other studies suggest that a BRAFV600E mutation is not always a negative prognostic indicator of aggressive disease.26,27 A case of PTC metastatic to the face was shown to have a RET receptor tyrosine kinase mutation. 6 In another case of metastases from FTC, the thyroid was negative for BRAF and TERT promotor mutations, but the cutaneous lesion showed a mutation in the TERT promoter. 28 These mutations may have contributed to metastases and genetic analysis has led to the development of target therapy, but future studies are needed to identify which mutations are associated with metastases to the skin.
This review also highlights the variability in the morphology of cutaneous metastases. Lesions can present as papules or nodules and resemble benign cysts or primary cutaneous neoplasms.29,30 Some patients report having the lesion or nodule for months but did not seek care until much later.31,32 The average time interval between diagnoses of primary thyroid carcinoma and cutaneous metastases was 48.27 months, which may reflect an initially missed or delayed diagnosis. Increased awareness by patients and physicians may lead to more prompt diagnosis and management.
Definitive diagnosis of metastasis requires histologic examination of biopsy specimens.12,32 Possible treatments include surgical excision for localized lesions, followed by either radioactive iodine or radiation. 4 Unfortunately, cutaneous metastases are often a sign of disseminated neoplastic disease with poor overall survival. 7 Common sites of other metastases are the lungs, lymph nodes, and bone which is consistent with our study’s findings showing lung, lymph node, and bone metastasis in 42%, 37%, and 33% of cases, respectively.5,6,33,34 In 34 patients with a known overall survival time, the average time was 13.07 months, and 9 of these cases were ATC which was not surprising given the aggressive nature of this form. 35
While case reports are usually excluded from reviews, due to the rarity of cutaneous metastases from thyroid carcinoma, most of the available literature were case reports and case series with the lowest level of evidence. As with many rare diseases, it is important to note that the results found here may be susceptible to publication bias and many cases reported here may not entirely reflect the true population. Patients in case reports are often not followed long-term and thus a lot of information on treatment and overall survival is lacking. Due to the variable morphology of cutaneous metastases, there are likely many undiagnosed cases and the true prevalence is much higher than reported.
Conclusion
Thyroid carcinoma with cutaneous metastasis is rare and may be easily misdiagnosed. While our review is limited by publication bias, cutaneous metastases should remain on the differential diagnosis of lesions and nodules, especially if found on the scalp, in patients with a history of thyroid carcinoma. They should be followed by a thorough examination, biopsy, and immunostaining. Future studies should determine which genetic mutations are most likely to be associated with cutaneous metastases. Our study represents an up-to-date review of thyroid carcinoma with cutaneous metastases.
Footnotes
Authors’ Note
An oral presentation of this abstract was presented at the AHNS 11th International Conference on Head and Neck Cancer in Montreal, QC, Canada, on July 9, 2023.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was not required for this review.
Informed Consent
Informed consent was not required for this review.